
Changes in Sleep Problems in Patients Who Underwent Surgical Treatment for Degenerative Spinal Disease with a Concurrent Sleep Disorder: A Nationwide Cohort Study in 3183 Patients during a Two-Year Perioperative Period

Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Patients
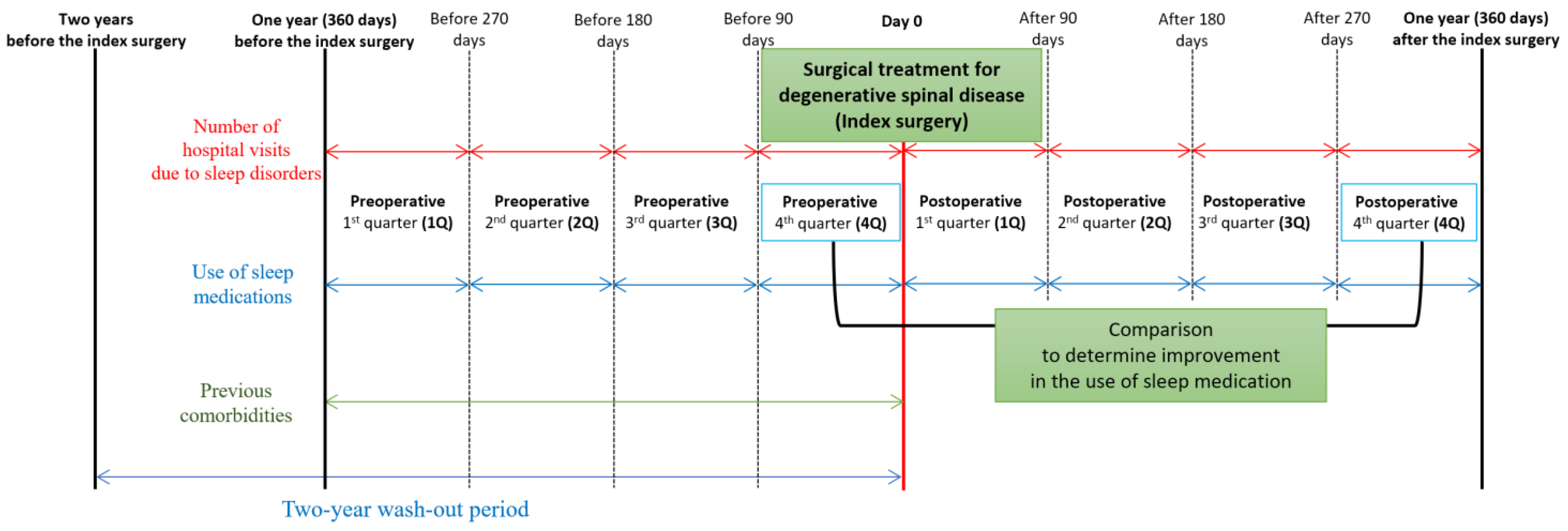
2.3. Two Target Outcomes Associated with Sleep Disturbance: Use of Sleep Medication and Hospital Visits Owing to Sleep Disorders
2.4. Definition of the Eight Quarters of Perioperative Periods
2.5. Evaluation of Perioperative Changes in the Two Target Outcomes
2.6. Statistical Analysis
3. Results
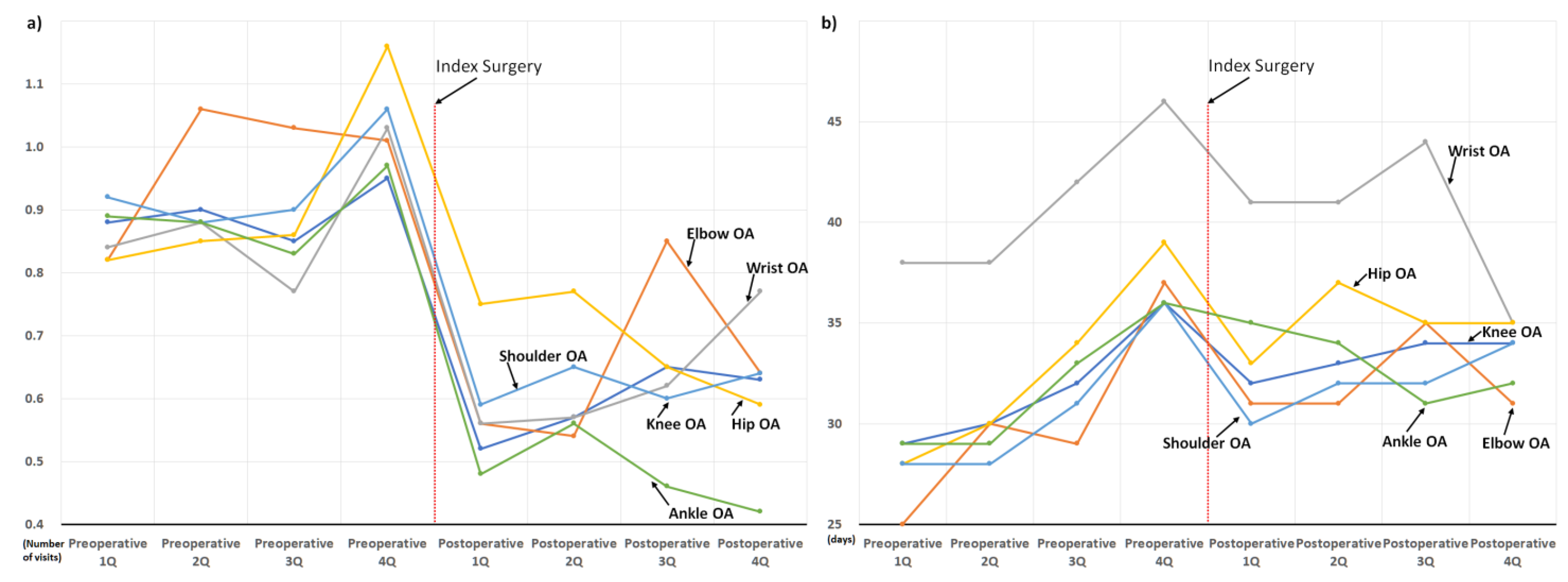
3.1. Overall Perioperative Changes in the Two Target Outcomes
3.2. Perioperative Changes in the Two Target Outcomes: According to the Demographics and Spinal Regions
3.3. Perioperative Changes in the Two Target Outcomes: According to the Comorbidities
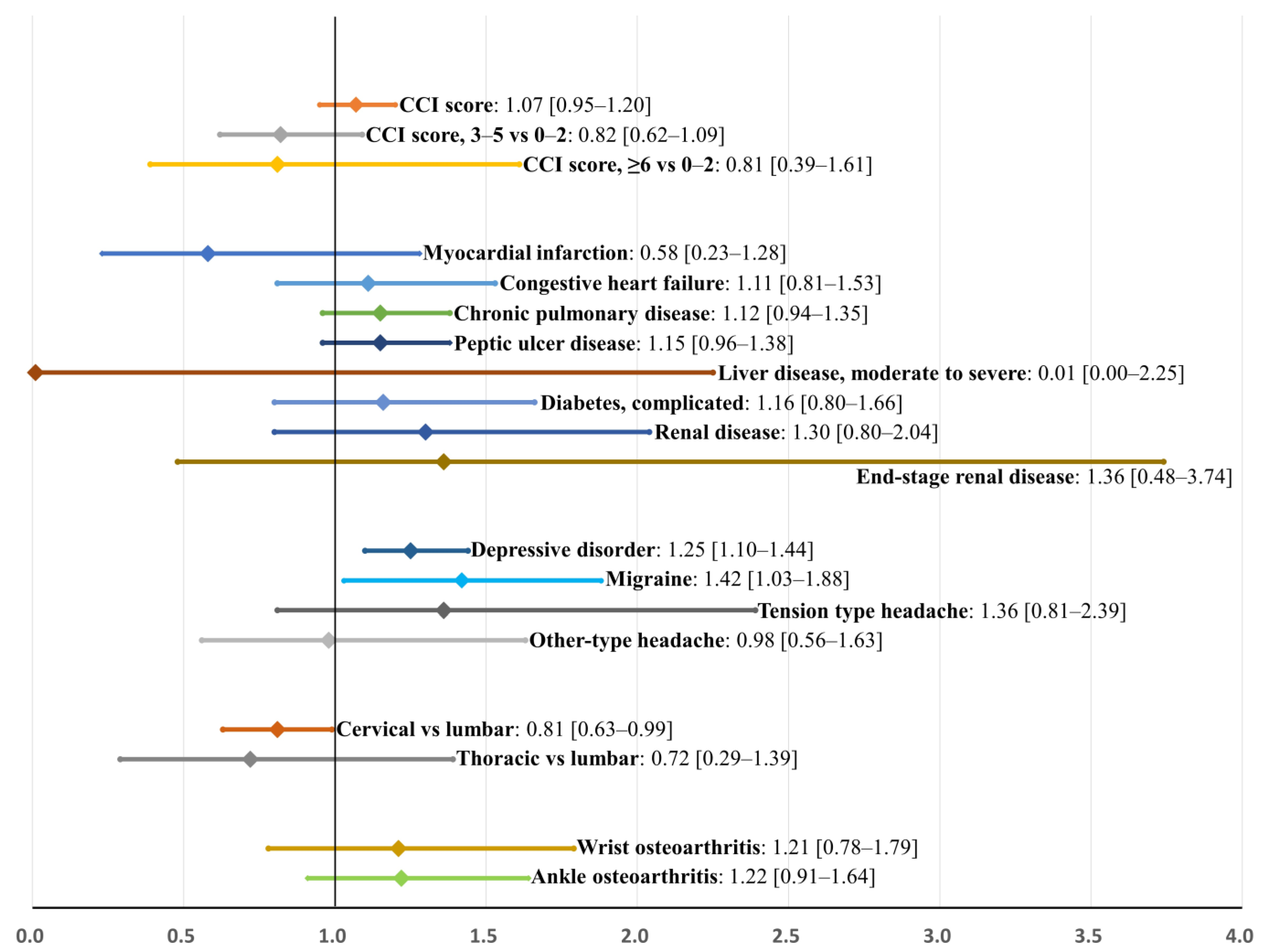
3.4. Factors Associated with Poor Improvement in the Sleep Medication after Surgery: Internal Validation Using Bootstrap Sampling
4. Discussions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dattilo, M.; Antunes, H.K.; Medeiros, A.; Mônico Neto, M.; Souza, H.S.; Tufik, S.; de Mello, M.T. Sleep and muscle recovery: Endocrinological and molecular basis for a new and promising hypothesis. Med. Hypotheses 2011, 77, 220–222. [Google Scholar] [CrossRef]
- Cirelli, C.; Tononi, G. Is sleep essential? PLoS Biol. 2008, 6, e216. [Google Scholar] [CrossRef] [Green Version]
- Luyster, F.S.; Strollo, P.J., Jr.; Zee, P.C.; Walsh, J.K. Sleep: A health imperative. Sleep 2012, 35, 727–734. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef]
- Stranges, S.; Tigbe, W.; Gómez-Olivé, F.X.; Thorogood, M.; Kandala, N.B. Sleep problems: An emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep 2012, 35, 1173–1181. [Google Scholar] [CrossRef] [Green Version]
- Sutton, D.A.; Moldofsky, H.; Badley, E.M. Insomnia and health problems in Canadians. Sleep 2001, 24, 665–670. [Google Scholar] [CrossRef]
- Hossain, J.L.; Shapiro, C.M. The prevalence, cost implications, and management of sleep disorders: An overview. Sleep Breath. = Schlaf Atm. 2002, 6, 85–102. [Google Scholar] [CrossRef]
- Schubert, C.R.; Cruickshanks, K.J.; Dalton, D.S.; Klein, B.E.; Klein, R.; Nondahl, D.M. Prevalence of sleep problems and quality of life in an older population. Sleep 2002, 25, 889–893. [Google Scholar]
- Mystakidou, K.; Parpa, E.; Tsilika, E.; Pathiaki, M.; Gennatas, K.; Smyrniotis, V.; Vassiliou, I. The relationship of subjective sleep quality, pain, and quality of life in advanced cancer patients. Sleep 2007, 30, 737–742. [Google Scholar] [CrossRef]
- Nagasaka, T.; Washida, N.; Uchiyama, K.; Hama, E.Y.; Kusahana, E.; Nakayama, T.; Yasuda, I.; Morimoto, K.; Itoh, H. Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis. Healthcare 2022, 10, 1030. [Google Scholar] [CrossRef]
- Broström, A.; Strömberg, A.; Dahlström, U.; Fridlund, B. Sleep difficulties, daytime sleepiness, and health-related quality of life in patients with chronic heart failure. J. Cardiovasc. Nurs. 2004, 19, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Nunes, D.M.; Mota, R.M.; de Pontes Neto, O.L.; Pereira, E.D.; de Bruin, V.M.; de Bruin, P.F. Impaired sleep reduces quality of life in chronic obstructive pulmonary disease. Lung 2009, 187, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Oh, J.K.; Kim, S.W.; Yee, J.S.; Kim, T.H. Risk factors for sleep disturbance in patients with cervical myelopathy and its clinical significance: A cross-sectional study. Spine J. Off. J. N. Am. Spine Soc. 2021, 21, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, J.; Kim, S.W.; Oh, J.K.; Park, M.S.; Kim, Y.W.; Kim, T.H. Prevalence of sleep disturbance in patients with lumbar spinal stenosis and analysis of the risk factors. Spine J. Off. J. N. Am. Spine Soc. 2020, 20, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Hong, S.J.; Park, J.H.; Ki, H. Sleep Disturbance and Its Clinical Implication in Patients with Adult Spinal Deformity: Comparison with Lumbar Spinal Stenosis. Pain Res. Manag. 2020, 2020, 6294151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artner, J.; Cakir, B.; Spiekermann, J.-A.; Kurz, S.; Leucht, F.; Reichel, H.; Lattig, F. Prevalence of sleep deprivation in patients with chronic neck and back pain: A retrospective evaluation of 1016 patients. J. Pain Res. 2013, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, K.N.; Gifford, C.S.; Qaqish, H.; Alexander, C.; Ren, G.; Caras, A.; Miller, W.K.; Schroeder, J.L. A Population-Based Study of Patients with Sleep-Wake Disorders Undergoing Elective Instrumented Spinal Surgery. World Neurosurg. 2022, 160, e335–e343. [Google Scholar] [CrossRef]
- Kim, J.; Kim, G.; Kim, S.W.; Oh, J.K.; Park, M.S.; Kim, Y.W.; Kim, T.H. Changes in sleep disturbance in patients with cervical myelopathy: Comparison between surgical treatment and conservative treatment. Spine J. Off. J. N. Am. Spine Soc. 2021, 21, 586–597. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.H.; Kim, T.H. Improvement of sleep quality after treatment in patients with lumbar spinal stenosis: A prospective comparative study between conservative versus surgical treatment. Sci. Rep. 2020, 10, 14135. [Google Scholar] [CrossRef]
- Buser, Z.; Ortega, B.; D’Oro, A.; Pannell, W.; Cohen, J.R.; Wang, J.; Golish, R.; Reed, M.; Wang, J.C. Spine Degenerative Conditions and Their Treatments: National Trends in the United States of America. Glob. Spine J. 2017, 8, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kang, M.S.; Kim, T.-H. Prevalence of Sleep Disturbance and Its Risk Factors in Patients Who Undergo Surgical Treatment for Degenerative Spinal Disease: A Nationwide Study of 106,837 Patients. J. Clin. Med. 2022, 11, 5932. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Ibáñez, V.; Silva, J.; Cauli, O. A survey on sleep assessment methods. PeerJ 2018, 6, e4849. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.; Youn, S.; Um, Y.H.; Kim, T.W.; Ju, G.; Lee, H.J.; Lee, C.; Lee, S.D.; Bae, K.; Kim, S.J.; et al. Korean Clinical Practice Guideline for the Diagnosis and Treatment of Insomnia in Adults. Psychiatry Investig. 2020, 17, 1048–1059. [Google Scholar] [CrossRef]
- Kim, J.; Ryu, H.; Kim, T.-H. Early Reoperation Rates and Its Risk Factors after Instrumented Spinal Fusion Surgery for Degenerative Spinal Disease: A Nationwide Cohort Study of 65,355 Patients. J. Clin. Med. 2022, 11, 3338. [Google Scholar] [CrossRef]
- Lim, J.S.; Kim, T.-H. Recurrence Rates and Its Associated Factors after Early Spinal Instrumentation for Pyogenic Spondylodiscitis: A Nationwide Cohort Study of 2148 Patients. J. Clin. Med. 2022, 11, 3356. [Google Scholar] [CrossRef]
- Kim, J.; Kim, T.-H. Risk Factors for Postoperative Deep Infection after Instrumented Spinal Fusion Surgeries for Degenerative Spinal Disease: A Nationwide Cohort Study of 194,036 Patients. J. Clin. Med. 2022, 11, 778. [Google Scholar] [CrossRef]
- Frenkel, W.J.; Jongerius, E.J.; van Mandjes Uitert, M.J.; van Munster, B.C.; de Rooij, S.E. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: A prospective cohort study. J. Am. Geriatr. Soc. 2014, 62, 342–346. [Google Scholar] [CrossRef]
- Park, H.-R.; Im, S.; Kim, H.; Jung, S.-Y.; Kim, D.; Jang, E.; Sung, Y.-K.; Cho, S.-K. Validation of algorithms to identify knee osteoarthritis patients in the claims database. Int. J. Rheum. Dis. 2019, 22, 890–896. [Google Scholar] [CrossRef]
- Burgess, H.J.; Burns, J.W.; Buvanendran, A.; Gupta, R.; Chont, M.; Kennedy, M.; Bruehl, S. Associations Between Sleep Disturbance and Chronic Pain Intensity and Function: A Test of Direct and Indirect Pathways. Clin. J. Pain 2019, 35, 569–576. [Google Scholar] [CrossRef]
- Onen, S.H.; Onen, F. Chronic Medical Conditions and Sleep in the Older Adult. Sleep Med. Clin. 2018, 13, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, E.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Inoue, R.; Chiba, D.; Okubo, N.; Takahashi, I.; Nakaji, S.; Ishibashi, Y. Nocturnal knee pain increases with the severity of knee osteoarthritis, disturbing patient sleep quality. Arthritis Care Res. 2014, 66, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Khazzam, M.S.; Mulligan, E.P.; Brunette-Christiansen, M.; Shirley, Z. Sleep Quality in Patients with Rotator Cuff Disease. J. Am. Acad. Orthop. Surg. 2018, 26, 215–222. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Categories | All | Patients without Postoperative Improvement in Sleep Medication | Patients with Postoperative Improvement in Sleep Medication | Proportions of Patients without Improvement | Standardized Mean Difference |
|---|---|---|---|---|---|---|
| Number of patients | 3183 | 776 | 2407 | 24.4% | ||
| Age | Mean ± SD | 66.7 ± 10.7 | 67.2 ± 10.5 | 66.5 ± 10.8 | 0.065 | |
| 20–49 | 213 (7) | 50 (6) | 163 (7) | 23.5% | ||
| 50–69 | 1525 (48) | 366 (47) | 1159 (48) | 24.0% | ||
| 70+ | 1445 (45) | 360 (46) | 1085 (45) | 24.9% | ||
| Sex | Men | 1308 (41) | 307 (40) | 1001 (42) | 23.5% | 0.046 |
| Women | 1875 (59) | 469 (60) | 1406 (58) | 25.0% | ||
| Region | Urban | 2714 (85) | 660 (85) | 2054 (85) | 24.3% | 0.012 |
| Rural | 469 (15) | 116 (15) | 353 (15) | 24.7% | ||
| Hospital | Tertiary | 640 (20) | 153 (20) | 487 (20) | 23.9% | 0.062 |
| General | 660 (21) | 172 (22) | 488 (20) | 26.1% | ||
| Others | 1883 (59) | 451 (58) | 1432 (59) | 24.0% | ||
| Spinal regions | Cervical | 461 (14) | 96 (12) | 365 (15) | 20.8% | 0.134 |
| Thoracic | 35 (1) | 7 (1) | 28 (1) | 20.0% | ||
| Lumbar | 2687 (84) | 673 (87) | 2014 (84) | 25.0% | ||
| Charlson comorbidity index score | Mean ± SD | 1.61 ± 1.46 | 1.75 ± 1.52 | 1.56 ± 1.44 | 0.136 | |
| 0–2 | 2427 (76) | 572 (74) | 1855 (77) | 23.6% | ||
| 3–5 | 696 (22) | 185 (24) | 511 (21) | 26.6% | ||
| ≥6 | 60 (2) | 19 (2) | 41 (2) | 31.7% |
| Variables | Categories | All | Patients without Postoperative Improvement in Sleep Medication | Patients with Postoperative Improvement in Sleep Medication | Proportions of Patients without Improvement | Standardized Mean Difference |
|---|---|---|---|---|---|---|
| General comorbidities | Myocardial infarction | 40 (1) | 7 (1) | 33 (1) | 17.5% | 0.233 |
| Congestive heart failure | 159 (5) | 45 (6) | 114 (5) | 28.3% | 0.118 | |
| Cerebrovascular disease | 441 (14) | 113 (15) | 328 (14) | 25.6% | 0.043 | |
| Peripheral vascular disease | 531 (17) | 140 (18) | 391 (16) | 26.4% | 0.070 | |
| Chronic pulmonary disease | 1059 (33) | 285 (37) | 774 (32) | 26.9% | 0.112 | |
| Rheumatologic disease | 161 (5) | 42 (5) | 119 (5) | 26.1% | 0.053 | |
| Peptic ulcer disease | 745 (23) | 205 (26) | 540 (22) | 27.5% | 0.119 | |
| Liver disease | ||||||
| Mild | 273 (9) | 70 (9) | 203 (8) | 25.6% | 0.041 | |
| Moderate to severe | 5 (0) | 1 (0) | 4 (0) | 20.0% | 0.140 | |
| Diabetes | ||||||
| Uncomplicated | 828 (26) | 206 (27) | 622 (26) | 24.9% | 0.020 | |
| Complicated | 245 (8) | 70 (9) | 175 (7) | 28.6% | 0.129 | |
| Hemiplegia or paraplegia | 26 (1) | 1 (0) | 25 (1) | 3.8% | 1.156 | |
| Renal disease | 105 (3) | 34 (4) | 71 (3) | 32.4% | 0.226 | |
| End-stage renal disease | 16 (1) | 6 (1) | 10 (0) | 37.5% | 0.344 | |
| Osteoporosis | 609 (19) | 144 (19) | 465 (19) | 23.6% | 0.027 | |
| Concurrent neuropsychiatric disorders | Depressive disorder | 1560 (49) | 423 (55) | 1137 (47) | 27.1% | 0.161 |
| Dementia | 106 (3) | 29 (4) | 77 (3) | 27.4% | 0.089 | |
| Parkinson disease | 51 (2) | 13 (2) | 38 (2) | 25.5% | 0.033 | |
| Migraine | 202 (6) | 67 (9) | 135 (6) | 33.2% | 0.256 | |
| Tension-type headache | 180 (6) | 59 (8) | 121 (5) | 32.8% | 0.243 | |
| Other-type headache | 246 (8) | 76 (10) | 170 (7) | 30.9% | 0.197 | |
| Concurrent osteoarthritis of extremities | Shoulder | 349 (11) | 90 (12) | 259 (11) | 25.8% | 0.047 |
| Elbow | 78 (2) | 18 (2) | 60 (2) | 23.1% | 0.041 | |
| Wrist | 94 (3) | 27 (3) | 67 (3) | 28.7% | 0.127 | |
| Hip | 299 (9) | 80 (10) | 219 (9) | 26.8% | 0.076 | |
| Knee | 991 (31) | 258 (33) | 733 (30) | 26.0% | 0.071 | |
| Ankle | 189 (6) | 53 (7) | 136 (6) | 28.0% | 0.111 |
| Variables | Categories | Univariable | Model 2 (Fully Adjusted) | Model 3 (Bootstrap Validation after Fully Adjusted) | |||
|---|---|---|---|---|---|---|---|
| Odds Ratio (95% Confidence Interval) | p-Value | Adjusted Odds Ratio (95% Confidence Interval) | p-Value | Adjusted Odds Ratio (95% Confidence Interval) | Bias (%) | ||
| Charlson comorbidity index score | 1.09 [1.03–1.15] | 0.002 | 1.07 [0.93–1.22] | 0.364 | 1.07 [0.95–1.20] | −6.7 | |
| 3–5 vs. 0–2 | 1.17 [1.77–2.02] | 0.102 | 0.83 [0.59–1.17] | 0.284 | 0.82 [0.62–1.09] | 4.7 | |
| ≥6 vs. 0–2 | 1.50 [0.87–2.61] | 0.148 | 0.81 [0.35–1.89] | 0.624 | 0.81 [0.39–1.61] | 2.4 | |
| Comorbidities | Myocardial infarction | 0.66 [0.29–1.49] | 0.312 | 0.64 [0.28–1.47] | 0.291 | 0.58 [0.23–1.28] | 22.5 |
| Congestive heart failure | 1.24 [0.87–1.77] | 0.238 | 1.12 [0.75–1.62] | 0.607 | 1.11 [0.81–1.53] | −10.3 | |
| Chronic pulmonary disease | 1.23 [1.03–1.45] | 0.019 | 1.13 [0.92–1.39] | 0.259 | 1.12 [0.94–1.35] | −3.8 | |
| Peptic ulcer disease | 1.24 [1.03–1.50] | 0.023 | 1.15 [0.92–1.43] | 0.233 | 1.15 [0.96–1.38] | 1.5 | |
| Liver disease, moderate to severe | 0.78 [0.09–6.95] | 0.820 | 0.56 [0.06–5.38] | 0.615 | 0.01 [0.00–2.25] | 678.3 | |
| Diabetes, complicated | 1.27 [0.95–1.69] | 0.112 | 1.16 [0.78–1.72] | 0.478 | 1.16 [0.80–1.66] | −2.3 | |
| Renal disease | 1.51 [0.99–2.29] | 0.054 | 1.29 [0.77–2.16] | 0.338 | 1.30 [0.80–2.04] | 2.2 | |
| End-stage renal disease | 1.87 [0.68–5.16] | 0.227 | 1.37 [0.45–4.16] | 0.578 | 1.36 [0.48–3.74] | −3.4 | |
| Comorbidities associated with neuropsychiatric disorders | Depressive disorder | 1.34 [1.14–1.57] | <0.001 | 1.25 [1.06–1.48] | 0.008 | 1.25 [1.10–1.44] | 1.4 |
| Migraine | 1.59 [1.17–2.16] | 0.003 | 1.42 [1.04–1.94] | 0.028 | 1.42 [1.03–1.88] | −0.6 | |
| Tension-type headache | 1.56 [1.13–2.15] | <0.001 | 1.28 [0.68–2.44] | 0.445 | 1.36 [0.81–2.39] | 23.1 | |
| Other-type headache | 1.43 [1.08–1.90] | 0.014 | 1.04 [0.59–1.84] | 0.889 | 0.98 [0.56–1.63] | −139.0 | |
| Surgical regions | Cervical vs. lumbar | 0.79 [0.62–1.00] | 0.052 | 0.82 [0.64–1.04] | 0.100 | 0.81 [0.63–0.99] | 8.9 |
| Thoracic vs. lumbar | 0.75 [0.33–1.72] | 0.495 | 0.77 [0.33–1.78] | 0.539 | 0.72 [0.29–1.39] | 26.9 | |
| Concurrent osteoarthritis | Wrist | 1.26 [0.80–1.98] | 0.320 | 1.21 [0.76–1.92] | 0.426 | 1.21 [0.78–1.79] | 0.3 |
| Ankle | 1.22 [0.88–1.70] | 0.227 | 1.22 [0.87–1.71] | 0.244 | 1.22 [0.91–1.64] | 1.2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kim, J.H.; Kim, T.-H. Changes in Sleep Problems in Patients Who Underwent Surgical Treatment for Degenerative Spinal Disease with a Concurrent Sleep Disorder: A Nationwide Cohort Study in 3183 Patients during a Two-Year Perioperative Period. J. Clin. Med. 2022, 11, 7402. https://doi.org/10.3390/jcm11247402
Kim J, Kim JH, Kim T-H. Changes in Sleep Problems in Patients Who Underwent Surgical Treatment for Degenerative Spinal Disease with a Concurrent Sleep Disorder: A Nationwide Cohort Study in 3183 Patients during a Two-Year Perioperative Period. Journal of Clinical Medicine. 2022; 11(24):7402. https://doi.org/10.3390/jcm11247402
Chicago/Turabian StyleKim, Jihye, Jang Hyun Kim, and Tae-Hwan Kim. 2022. "Changes in Sleep Problems in Patients Who Underwent Surgical Treatment for Degenerative Spinal Disease with a Concurrent Sleep Disorder: A Nationwide Cohort Study in 3183 Patients during a Two-Year Perioperative Period" Journal of Clinical Medicine 11, no. 24: 7402. https://doi.org/10.3390/jcm11247402