
Treatment of Cesarean Scar Ectopic Pregnancy in China with Uterine Artery Embolization—A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Literature Search Results
3.2. Characteristic of Included Studies
3.3. Quality Assessment
3.4. Analysis of the Outcomes
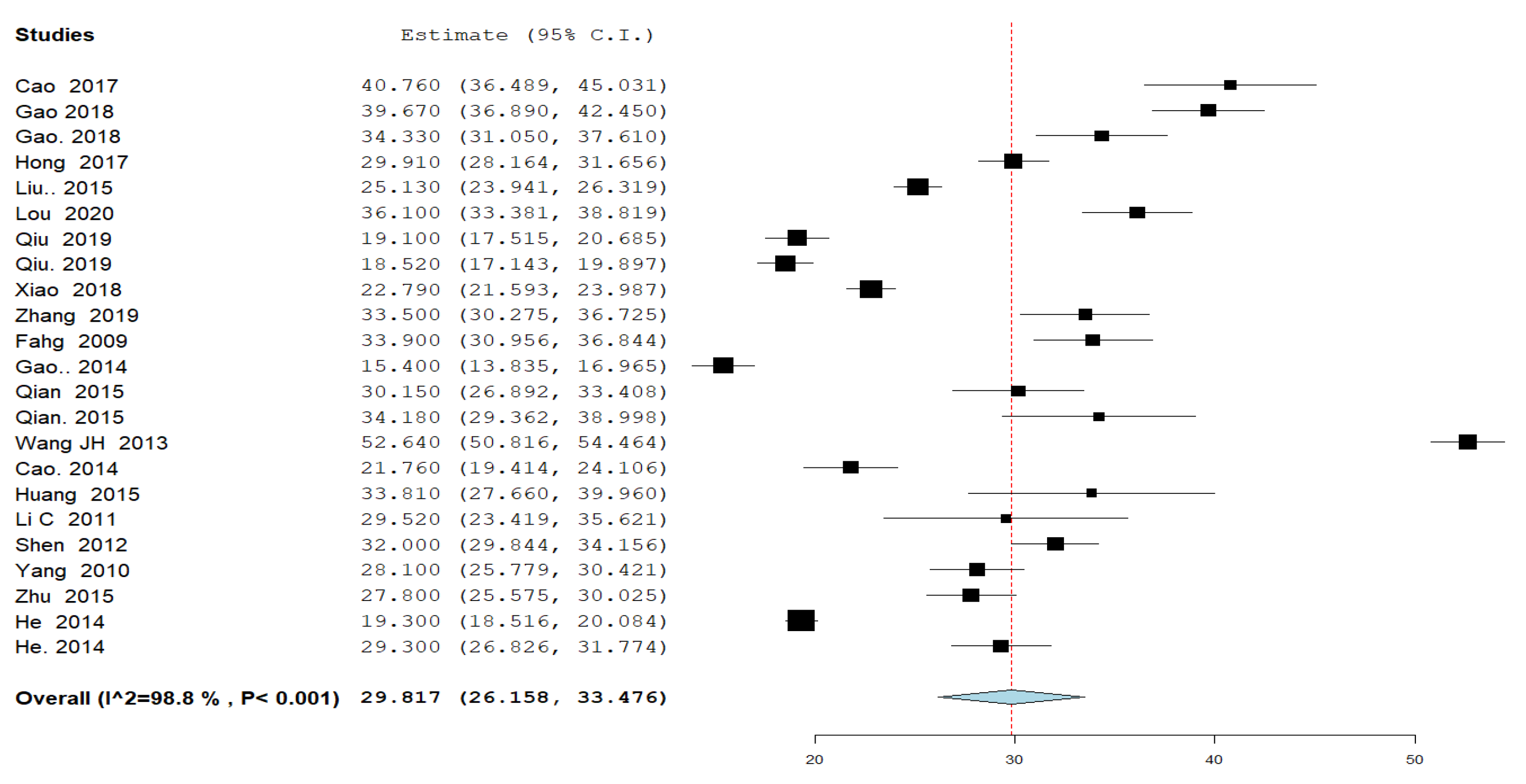
3.4.1. Time for Serum β-Human Chorionic Gonadotropin (β-hCG) Normalization (Figure 1)

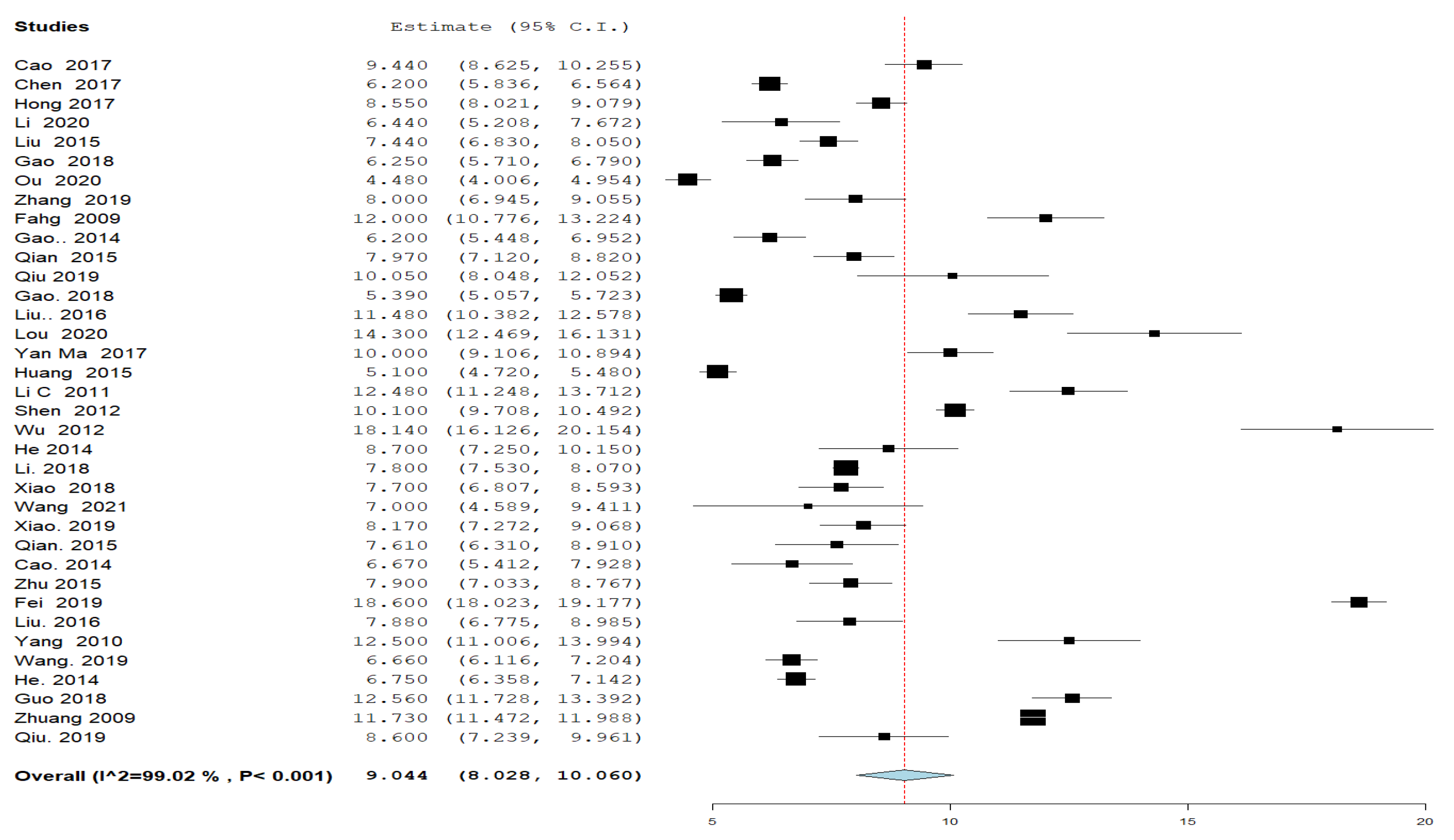
3.4.2. Hospital Stay (Figure 2)

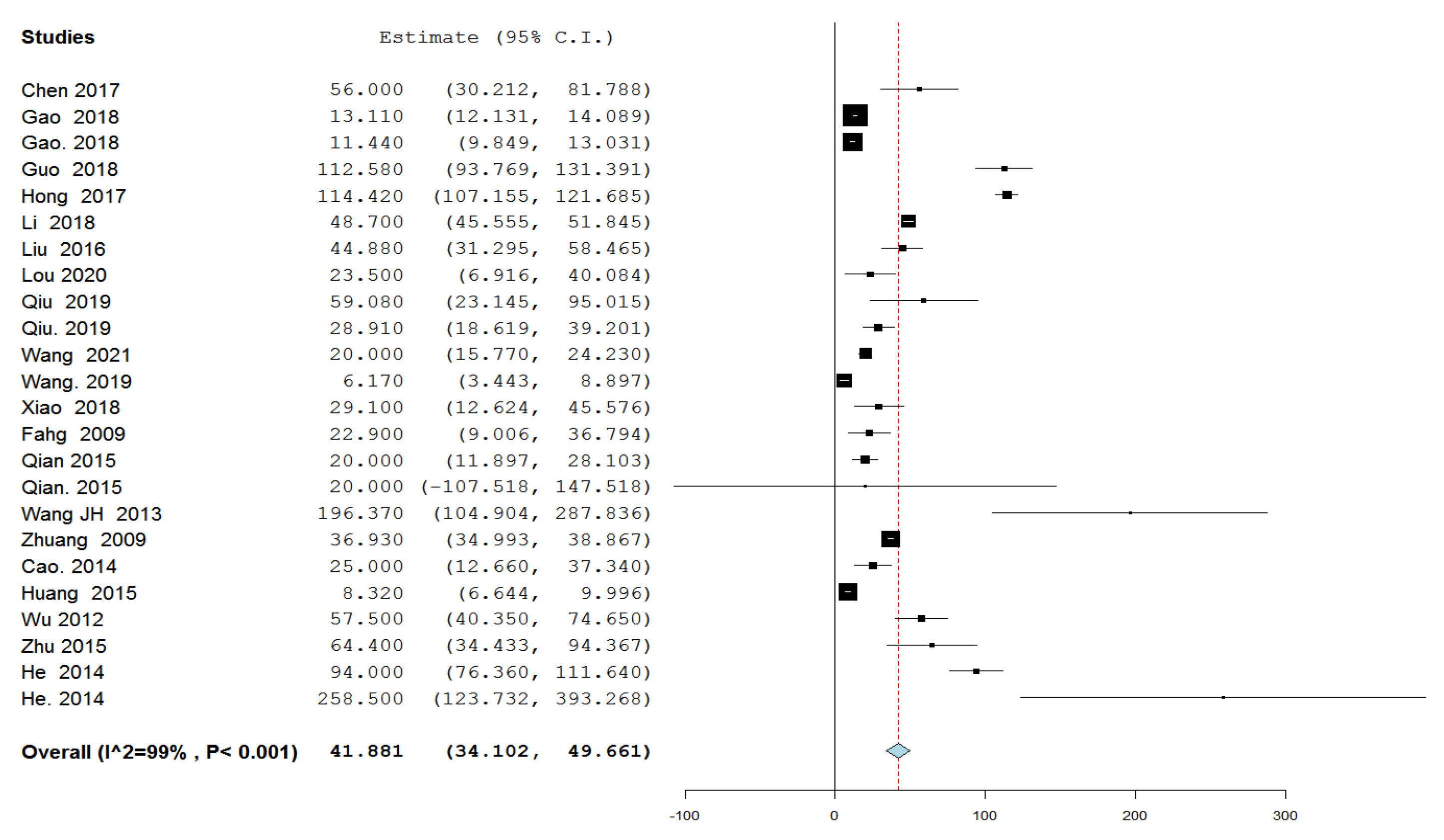
3.4.3. Amount of Intraprocedural Blood Loss (Figure 3)

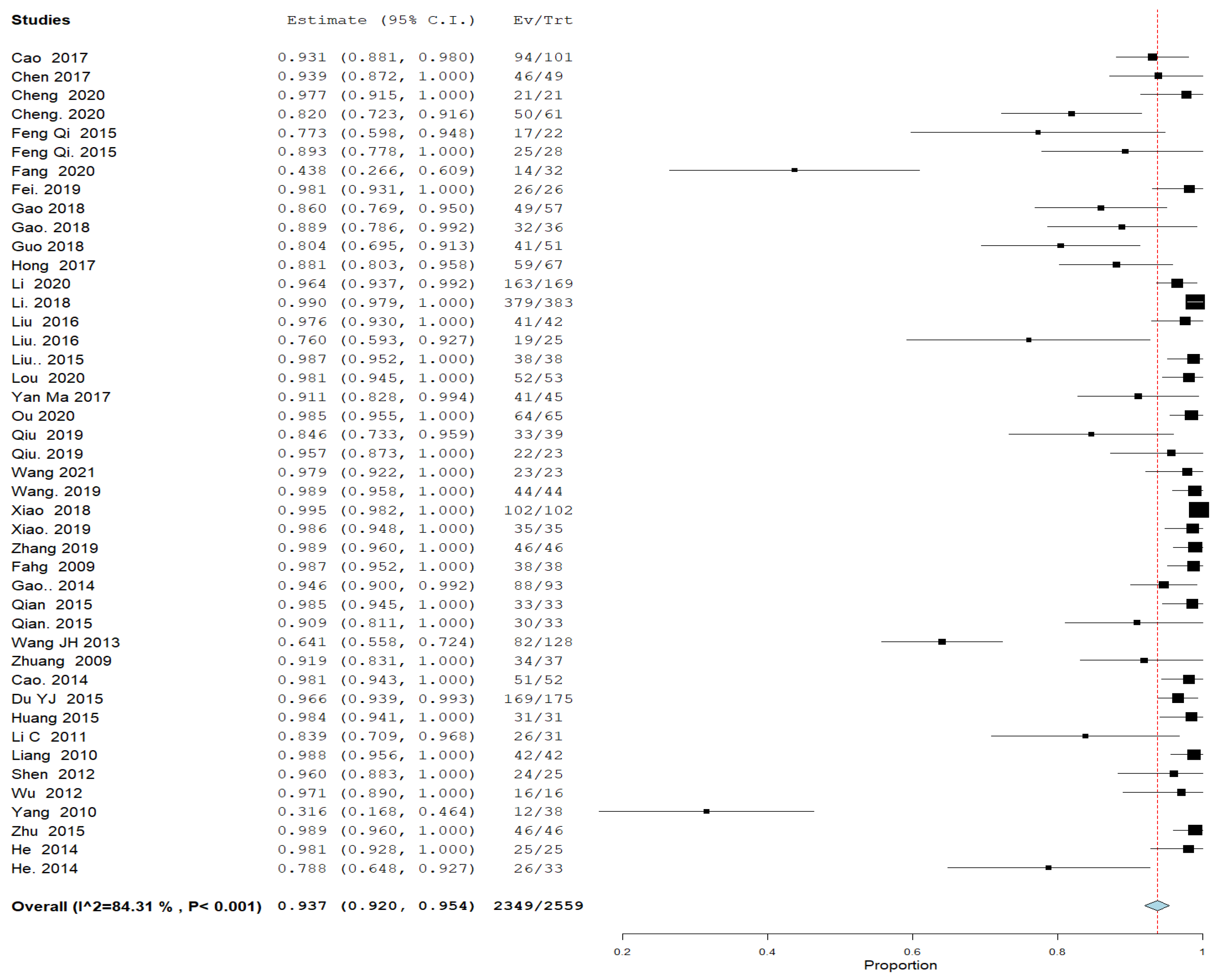
3.4.4. Success Rate (Figure 4)

3.4.5. Severe Complication Rate (Figure 5)

4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Commitment to Diversity
References
- Della-Giustina, D.; Denny, M. Ectopic pregnancy. Emerg. Med. Clin. N. Am. 2003, 21, 565–584. [Google Scholar] [CrossRef] [PubMed]
- Mettler, L.; Sodhi, B.; Schollmeyer, T.; Mangeshikar, P. Ectopic pregnancy treatment by laparoscopy, a short glimpse. Minim. Invasive Ther. Allied Technol. 2006, 15, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Jurkovic, D.; Hillaby, K.; Woelfer, B.; Lawrence, A.; Salim, R.; Elson, C.J. First-trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2003, 21, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Mi, J.; Liu, F. Rate of caesarean section is alarming in China. Lancet (Lond. Engl.) 2014, 383, 1463–1464. [Google Scholar] [CrossRef]
- Lavender, T.; Hofmeyr, G.J.; Neilson, J.P.; Kingdon, C.; Gyte, G.M.L. Caesarean section for non-medical reasons at term. Cochrane Database Syst. Rev. 2012, 2012, CD004660. [Google Scholar] [CrossRef] [Green Version]
- Maymon, R.; Svirsky, R.; Smorgick, N.; Mendlovic, S.; Halperin, R.; Gilad, K.; Tobvin, Y. Fertility performance and obstetric outcomes among women with previous cesarean scar pregnancy. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2011, 30, 1179–1184. [Google Scholar] [CrossRef]
- Seow, K.M.; Huang, L.W.; Lin, Y.H.; Lin, M.Y.-S.; Tsai, Y.L.; Hwang, J.L. Cesarean scar pregnancy: Issues in management. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2004, 23, 247–253. [Google Scholar] [CrossRef]
- Arslan, M.; Pata, O.; Dilek, T.U.K.; Aktas, A.; Aban, M.; Dilek, S. Treatment of viable cesarean scar ectopic pregnancy with suction curettage. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2005, 89, 163–166. [Google Scholar] [CrossRef]
- Hois, E.L.; Hibbeln, J.F.; Alonzo, M.J.; Chen, M.E.; Freimanis, M.G. Ectopic pregnancy in a cesarean section scar treated with intramuscular methotrexate and bilateral uterine artery embolization. J. Clin. Ultrasound JCU 2008, 36, 123–127. [Google Scholar] [CrossRef]
- Rotas, M.A.; Haberman, S.; Levgur, M. Cesarean scar ectopic pregnancies: Etiology, diagnosis, and management. Obstet. Gynecol. 2006, 107, 1373–1381. [Google Scholar] [CrossRef]
- Li, C.; Li, C.; Feng, D.; Jia, C.; Liu, B.; Zhan, X. Transcatheter arterial chemoembolization versus systemic methotrexate for the management of cesarean scar pregnancy. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2011, 113, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Jiang, Z.-B.; Huang, M.-S.; Guan, S.-H.; Zhu, K.-S.; Qian, J.-S.; Zhou, B.; Li, M.-A.; Shan, H. Uterine artery embolization combined with methotrexate in the treatment of cesarean scar pregnancy: Results of a case series and review of the literature. J. Vasc. Interv. Radiol. JVIR 2012, 23, 1582–1588. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, X.; Zhu, J.; Di, W. Caesarean scar pregnancy: Comparative efficacy and safety of treatment by uterine artery chemoembolization and systemic methotrexate injection. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 161, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Hou, Y.-Y.; Sun, F.; Xia, W.; Yang, Y.; Tian, T.; Chen, Q.-F.; Li, X.-C. A retrospective comparative study evaluating the efficacy of adding intra-arterial methotrexate infusion to uterine artery embolisation followed by curettage for cesarean scar pregnancy. Arch. Gynecol. Obstet. 2018, 297, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Yu, J.; Zhang, Q.; Song, X. Clinical Efficacy and Safety of Uterine Artery Embolization (UAE) versus Laparoscopic Cesarean Scar Pregnancy Debridement Surgery (LCSPDS) in Treatment of Cesarean Scar Pregnancy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 4659–4666. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, R.; Qian, H.; Lv, H. Pituitrin local injection versus uterine artery embolization in the management of cesarean scar pregnancy: A retrospective cohort study. J. Obstet. Gynaecol. Res. 2021, 47, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0. 1. The Cochrane Collaboration. 2008. Available online: http://www.cochrane-handbook.org (accessed on 3 March 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- NIH National Heart, Lung, and Blood Institute. Study Quality Assessment Tools: Quality Assessment Tool for Observational Cohort, Cross-Sectional and Case Series Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 3 March 2021).
- Cao, G.-S.; Liu, R.-Q.; Liu, Y.-Y.; Liu, J.-W.; Li, L.-P.; Zhang, Q.; Cao, H.-C.; Li, T.-X. Menstruation recovery in scar pregnancy patients undergoing UAE and curettage and its influencing factors. Medicine 2018, 97, e9584. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Zhu, L.; Jin, L.; Gao, J.; Chen, C. Uterine artery embolization in cesarean scar pregnancy: Safe and effective intervention. Chin. Med. J. 2014, 127, 2322–2326. [Google Scholar]
- Chen, H.; Zhou, J.; Wang, H.; Tan, W.; Yao, M.; Wang, X. The Treatment of Cesarean Scar Pregnancy with Uterine Artery Embolization and Curettage as Compared to Transvaginal Hysterotomy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 44–49. [Google Scholar] [CrossRef]
- Cheng, Q.; Tian, Q.; Chang, K.-K.; Yi, X.-F. Comparison of the efficacy and safety of different surgical strategies for patients with type II cesarean scar pregnancy. Reprod. Dev. Med. 2020, 4, 89–96. [Google Scholar] [CrossRef]
- Du, Y.J.; Zhang, X.H.; Wang, L.Q. Risk Factors for Haemorrhage during Suction Curettage after Uterine Artery Embolization for Treating Caesarean Scar Pregnancy: A Case-Control Study. Gynecol. Obstet. Investig. 2015, 80, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Fahg, A.-H.; Chen, Q.-F.; Qian, Z.-X.; Li, Q.-Y.; Meng, Y. Correlation Questions Clinical Discussion of Uterine Artery Embolization in Induced Abortion Patients with Management of Cesarean Scar Pregnancy. J. Reprod. Contracept. 2009, 20, 153–160. [Google Scholar] [CrossRef]
- Fang, S.; Zhang, P.; Zhu, Y.; Wang, F.; He, L. A Retrospective Analysis of the Treatment of Cesarean Scar Pregnancy by High-Intensity Focused Ultrasound, Uterine Artery Embolization and Surgery. Front. Surg. 2020, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Fei, H.; Jiang, X.; Li, T.; Pan, Y.; Guo, H.; Xu, X.; Shu, S. Comparison Of Three Different Treatment Methods For Cesarean Scar Pregnancy. Ther. Clin. Risk Manag. 2019, 15, 1377–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.; Huang, Z.; Gao, J.; Mai, H.; Zhang, Y.; Wang, X. Uterine artery embolization followed by dilation and curettage within 24 hours compared with systemic methotrexate for cesarean scar pregnancy. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2014, 127, 147–151. [Google Scholar] [CrossRef]
- He, Y.; Wu, X.; Zhu, Q.; Wu, X.; Feng, L.; Wu, X.; Zhao, A.; Di, W. Combined laparoscopy and hysteroscopy vs. uterine curettage in the uterine artery embolization-based management of cesarean scar pregnancy: A retrospective cohort study. BMC Women’s Health 2014, 14, 116. [Google Scholar]
- Hong, Y.; Guo, Q.; Pu, Y.; Lu, D.; Hu, M. Outcome of high-intensity focused ultrasound and uterine artery embolization in the treatment and management of cesarean scar pregnancy: A retrospective study. Medicine 2017, 96, e7687. [Google Scholar] [CrossRef]
- Huang, Y.; Li, Y.; Xi, R.; Chen, Z.; Ying, D.; Li, Z.; Yang, Y. An application of uterine artery chemoembolization in treating cesarean scar pregnancy. Int. J. Clin. Exp. Med. 2015, 8, 2570–2577. [Google Scholar] [PubMed]
- Li, X.; Niu, H.; Li, J.; Zhang, L.; Qu, Q. Clinical assessment of uterine artery embolization combined with curettage when treating patients with cesarean scar pregnancy: A retrospective study of 169 cases. J. Obstet. Gynaecol. Res. 2020, 46, 1110–1116. [Google Scholar] [CrossRef]
- Li, Y.; Lu, L.; Wang, W.; Sun, J.; Zhang, X.; Huang, X. Retrospective study of patients with cesarean scar pregnancies treated by uterine artery chemoembolization and curettage. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2018, 143, 172–177. [Google Scholar] [CrossRef]
- Liang, F.; He, J. Methotrexate-based bilateral uterine arterial chemoembolization for treatment of cesarean scar pregnancy. Acta Obstet. Et Gynecol. Scand. 2010, 89, 1592–1594. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Wu, J.; Cao, J.; Xue, Y.; Dai, C.; Xu, J.; Jia, X. Comparison of three treatment strategies for cesarean scar pregnancy. Arch. Gynecol. Obstet. 2017, 296, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Shen, L.; Wang, Q.; Wang, W.; Sun, Z. Uterine artery embolization combined with curettage vs. methotrexate plus curettage for cesarean scar pregnancy. Arch. Gynecol. Obstet. 2016, 294, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Lou, T.; Gao, Y.; Feng, Y.; Lu, J.; Zhang, Z.; Bai, H. Reproductive outcomes of cesarean scar pregnancies pretreated with methotrexate and uterine artery embolization prior to curettage. Taiwan. J. Obstet. Gynecol. 2020, 59, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Shao, M.; Shao, X. Analysis of risk factors for intraoperative hemorrhage of cesarean scar pregnancy. Medicine 2017, 96, e7327. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.; Peng, P.; Li, C.; Teng, L.; Liu, X. Assessment of the necessity of uterine artery embolization during suction and curettage for caesarean scar pregnancy: A prospective cohort study. BMC Pregnancy Childbirth 2020, 20, 378. [Google Scholar] [CrossRef] [PubMed]
- Pyra, K.; Szmygin, M.; Bérczi, V.; Tsitskari, M.; Sojka, M.; Pietras, G. Clinical outcome and analysis of procedural failure during uterine artery chemoembolization as a treatment of caesarean scar pregnancy. Videosurgery Other Miniinvasive Tech. 2021, 16, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Qi, F.; Zhou, W.; Wang, M.-F.; Chai, Z.-Y.; Zheng, L.-Z. Uterine artery embolization with and without local methotrexate infusion for the treatment of cesarean scar pregnancy. Taiwan. J. Obstet. Gynecol. 2015, 54, 376–380. [Google Scholar] [CrossRef] [Green Version]
- Qian, Z.-D.; Huang, L.-L.; Zhu, X.-M. Curettage or operative hysteroscopy in the treatment of cesarean scar pregnancy. Arch. Gynecol. Obstet. 2015, 292, 1055–1061. [Google Scholar] [CrossRef]
- Qiu, J.; Fu, Y.; Xu, J.; Huang, X.; Yao, G.; Lu, W. Analysis on clinical effects of dilation and curettage guided by ultrasonography versus hysteroscopy after uterine artery embolization in the treatment of cesarean scar pregnancy. Ther. Clin. Risk Manag. 2019, 15, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, L.; Tan, A.; Zhu, H.; Guo, C.; Liu, D.; Huang, W. Bilateral uterine artery chemoembolization with methotrexate for cesarean scar pregnancy. Am. J. Obstet. Gynecol. 2012, 207, 386.e1–386.e6. [Google Scholar] [CrossRef] [PubMed]
- Stępniak, A.; Paszkowski, T.; Jargiełło, T.; Czuczwar, P. Effectiveness, complications and reproductive outcome of selective chemoembolization with methotrexate followed by suction curettage for caesarean scar pregnancy—A prospective observational study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 241, 56–59. [Google Scholar] [CrossRef]
- Tumenjargal, A.; Tokue, H.; Kishi, H.; Hirasawa, H.; Taketomi-Takahashi, A.; Tsushima, Y. Uterine Artery Embolization Combined with Dilation and Curettage for the Treatment of Cesarean Scar Pregnancy: Efficacy and Future Fertility. Cardiovasc. Interv. Radiol. 2018, 41, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-H.; Qian, Z.-D.; Zhuang, Y.-L.; Du, Y.-J.; Zhu, L.-H.; Huang, L.-L. Risk factors for intraoperative hemorrhage at evacuation of a cesarean scar pregnancy following uterine artery embolization. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2013, 123, 240–243. [Google Scholar] [CrossRef]
- Xiao, F.-Y.; Xue, X.-H.; Lu, X. Comparison of Five Treatment Strategies for Cesarean Scar Pregnancy. Reprod. Dev. Med. 2018, 2, 88–94. [Google Scholar] [CrossRef]
- Xiao, Z.; Cheng, D.; Chen, J.; Yang, J.; Xu, W.; Xie, Q. The effects of methotrexate and uterine arterial embolization in patients with cesarean scar pregnancy: A retrospective case-control study. Medicine 2019, 98, e14913. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Luo, F.; Xia, Y.; Mei, L.; Xie, L.; Liu, H. Clinical analysis of 211 cases of cesarean scar pregnancy. Clin. Exp. Obstet. Gynecol. 2019, 46, 948–952. [Google Scholar] [CrossRef]
- Yang, X.Y.; Yu, H.; Li, K.M.; Chu, Y.X.; Zheng, A. Uterine artery embolisation combined with local methotrexate for treatment of caesarean scar pregnancy. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 990–996. [Google Scholar] [CrossRef]
- Zhang, S.; Zhou, T.; Li, M.; Sheng, C.; Shou, J. Dilation and curettage following local sclerotherapy for cesarean scar pregnancy. Int. J. Clin. Exp. Med. 2019, 12, 730–734. [Google Scholar]
- Zhu, X.; Deng, X.; Xiao, S.; Wan, Y.; Xue, M. A comparison of high-intensity focused ultrasound and uterine artery embolisation for the management of caesarean scar pregnancy. Int. J. Hyperth. Off. J. Eur. Soc. Hyperthermic Oncol. North Am. Hyperth. Group 2016, 32, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Huang, L. Uterine artery embolization compared with methotrexate for the management of pregnancy implanted within a cesarean scar. Am. J. Obstet. Gynecol. 2009, 201, 152.e1–152.e3. [Google Scholar] [CrossRef] [PubMed]
- Qiao, B.; Zhang, Z.; Li, Y. Uterine Artery Embolization Versus Methotrexate for Cesarean Scar Pregnancy in a Chinese Population: A Meta-analysis. J. Minim. Invasive Gynecol. 2016, 23, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Kazeminia, M.; Shohaimi, S.; Nankali, A.A.-D.; Mohammadi, M. Evaluation of treatment of previous cesarean scar pregnancy with methotrexate: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. RBE 2020, 18, 108. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Chen, S.; Li, C.; Zhang, X.; Duan, H.; Sooranna, S. Curettage after uterine artery embolization combined with methotrexate treatment for caesarean scar pregnancy. Exp. Ther. Med. 2016, 12, 1469–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, W.; Hu, D.; Li, Z.; Wang, L.; Yang, W.; Hu, S. Bilateral uterine artery chemoembolization combined with dilation and curettage for treatment of cesarean scar pregnancy: A method for preserving the uterus. J. Obstet. Gynaecol. Res. 2013, 39, 1153–1158. [Google Scholar] [CrossRef]
- Birch Petersen, K.; Hoffmann, E.; Rifbjerg Larsen, C.; Svarre Nielsen, H. Cesarean scar pregnancy: A systematic review of treatment studies. Fertil. Steril. 2016, 105, 958–967. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Year of Publication | Study Design | Inclusion Period | Primary Treatment Modality | Number of Cases | Age | Gestational Age (Days) | Success Rate (%) | Treatment Failure Causes | Severe Complications Rate (%) | Conclusion | Methodological Quality | Country of Origin |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cao 2017 [20] | 2017 | Retrospective cohort Study | 2012–2016 | UAE + curettage | 101 | 32.98 (4.96) | – | 93.07% | Treatment failure (n = 7) [underwent curettage again] | 2.97% | Reduced menstrual blood volume can occur in scar pregnancy patients who received uterine artery embolization combined with curettage. | Fair | China |
| Chen 2017 [22] | 2017 | Retrospective cohort Study | 2014–2016 | UAE + curettage | 49 | 33.7 (4.8) | – | 93.90% | Treatment failure (n = 3) [underwent transvaginal hysterotomy] | 4.08% | UAE combined with uterine curettage is less advantageous than transvaginal hysterotomy. | Fair | China |
| Cheng 2020 [23] | 2020 | Retrospective cohort Study | 2010–2015 | UAE + hysteroscopy | 21 | 33.9 (1) | 49 (45.5–65.5) | 100% | – | 0% | Compared with D&C ± UAE, LAOH ± UAE showed a higher success rate for CSP–II patients. | Fair | China |
| UAE + D&C | 61 | 33.5 (0.6) | 52 (42–58) | 82% | Treatment failure (n = 3) [laparoscopic surgery or laparotomy] | 4.90% | |||||||
| Qi 2015 [41] | 2015 | Case series | 2009–2013 | UAE + MTX + D&C | 22 | 31.68 (4.58) | 59.86 (17.67) | 77.30% | Treatment failure (n = 8) additional intra–amniotic MTX injection or systemic MTX + D&C (n = 2), hysterotomy (n = 1). severe vaginal bleeding during curettage (n = 4) [hysterotomy] gelatin sponge separated and embolized the right leg (n = 1) [a second UAE.] | 0% | UAE with or without local MTX infusion might be an effective treatment for CSP. | Good | China |
| UAE + curettage | 28 | 31.68 (4.58) | 54.33 (17.51) | 89.30% | 0% | ||||||||
| Fang 2020 [26] | 2020 | Case series | 2010–2016 | UAE + curettage | 32 | – | 68.05 (23.29) | 43.75% | Treatment failure (n = 18) Massive vaginal bleeding (n = 5) [received blood transfusions and laparoscopy or laparotomy] large gestational sac (n = 13) [underwent surgery] | 27.78% | CSP patients with short gestational age and small gestational sac can be treated with surgery, UAE, and HIFU and achieve safe and effective therapeutic effects. | Good | China |
| Fei 2019 [27] | 2019 | Retrospective cohort Study | 2008–2017 | UAE + MTX | 26 | 31.4 (4.4) | – | 100% | – | 0% | There is no universal agreement on the optimal treatment modality for CSP. | Fair | China |
| Gao 2018 [14] | 2018 | Retrospective cohort study | 2010–2015 | UAE + curettage | 57 | 33.46 (4.47) | 54.25 (11.6) | 86% | Treatment failure (n = 5) [underwent a repeat curettage or intrauterine packing with a water balloon] | 0% | Adding intra–arterial MTX to UAE and curettage significantly promoted postoperative recovery, though success rate and bleeding events were not significantly affected. | Fair | China |
| UAE + MTX +D&C | 36 | 32.18 (5.65) | 55.58 (9.82) | 88.90% | Treatment failure (n = 2) [underwent a repeat curettage and intrauterine packing with a water balloon] | 0% | |||||||
| Guo 2018 [15] | 2018 | Retrospective cohort Study | 2012–2017 | UAE | 51 | 32.21 (5.68) | 54.82 (9.27) | 80.40% | Treatment failure (n = 10) laparotomy hysterectomy (n = 5) LCSPDS operation (n = 3) scar lesion removal by abdominal incision (n = 2) | 9.8% (5/51) | UAE and LCSPDS each have their advantages and disadvantages in treating CSP. Thus, appropriate individualized surgical programs based on specific patient circumstances are needed to avoid indiscriminately performing complete uterine cavity curettage. | Fair | China |
| Hong 2017 [30] | 2017 | Retrospective cohort Study | 2014–2016 | UAE + curettage | 67 | 31.74 (3.69) | – | 88.06% | _ | 0% | UAE combined with suction curettage under hysteroscopy is safe and effective in the management of CSP. | Fair | China |
| Li 2020 [32] | 2020 | Retrospective cohort Study | 2013–2017 | UAE + curettage | 169 | 33.58 (4.88) | – | 96% | Treatment failure (n = 6) repeated curettage (n = 2) resection of gestational tissues (n = 2) hemostatic drugs (n = 2) | 0% | UAE combined with curettage treatment in CSP patients demonstrates a favorable success rate, which can also reduce MBV and proceeding pregnancy rate. | Fair | China |
| Li 2018 [33] | 2018 | Retrospective cohort Study | 2006–2016 | UACE + curettage + MTX | 383 | 32.3 (4.9) | – | 99% | Treatment failure (n = 4) massive blood loss of (n = 1) [systemic methotrexate] residual tissues (n = 3)[underwent hysteroscopic or transabdominal resection] | 0.26% | UACE combined with curettage was found to be an effective fertility–sparing treatment for CSP. Further, the approach did not seem to harm future reproductive ability. | Poor | China |
| Liu 2016 [36] | 2016 | Retrospective cohort Study | 2014–2016 | UAE + MTX + D&C | 42 | 32.43 (4.2) | – | 97.50% | Treatment failure (n = 1) [needed additional treatment.] | 0.00% | The combination of UAE, local MTX injection, and D&C for CSP patients is the optimal treatment strategy. | Fair | China |
| UAE + MTX | 25 | 32.44 (6.16) | – | 76% | Treatment failure (n = 6) [required additional systemic MTX or D&C] | 0% | |||||||
| Liu 2015 [35] | 2015 | Retrospective cohort Study | 2005–2013 | UAE + curettage | 38 | 33.42 (5.29) | 55.42 (14.28) | 100% | – | 0% | UAE combined with curettage appears to be superior to MTX plus curettage for treatment of CSP with high serum b–hCG level. | Fair | China |
| Lou 2020 [37] | 2020 | Retrospective cohort Study | 2013–2015 | UAE + MTX + D&C | 53 | 33 (3.6) | 47 (8.4) | 97.90% | Treatment failure (n = 1) [emergency UAE + Curettage] | 0% | Pretreatment with MTX and UAE prior to curettage is safe and effective for the management of CSP. | Fair | China |
| Ma 2017 [38] | 2017 | Retrospective cohort Study | 2012–2016 | UAE + MTX + D&C | 45 | 33 (6) | – | 91.10% | Treatment failure (n = 4) systemic and local MTX therapy + curettage (n = 1) [supplementary MTX therapy] (n = 2) abdominal CSP mass resection (n = 1) | 0% | All treatments have high success rates and no significant effects on intraoperative bleeding. | Fair | China |
| Ou 2020 [39] | 2020 | Prospective cohort study | 2016–2018 | UAE + curettage | 65 | 34 (4.4) | 52.29 (10.32) | 98.46% | Treatment failure (n = 1) [repeat curettage] | 0% | Suction and curettage alone is a more suitable option than UAE followed by suction and curettage. | Fair | China |
| Qiu 2019 [43] | 2019 | Retrospective cohort Study | 2013–2018 | UAE + curettage | 39 | 32.1 (5.02) | _ | 84.60% | Treatment failure (n = 6) Massive vaginal bleeding (n = 3) [hysteroscopy or iodoform gauze packing.] unsatisfactory decrease in serum β–HCG level (n = 3) [received intramuscular injection of MTX] retained products of conception (n = 3) [underwent hysteroscopy] | 0% | D&C guided by ultrasonography after UAE treatment showed good clinical efficacy. | Fair | China |
| UAE + hysteroscopy | 23 | 32.48 (4.73) | _ | 95.70% | Treatment failure (n = 1) Massive vaginal bleeding received [iodoform gauze packing] | 0% | Hysteroscopy after UAE treatment showed good clinical efficacy. | ||||||
| Wang 2021 [16] | 2021 | Retrospective cohort study | 2017–2019 | UAE+ D&C + Hysteroscopy | 23 | 29.2 (3.6) | _ | 100% | _ | 8.70% | UAE pretreatment method seems to be effective, economical, and with few side effects in the management of CSP. | Fair | China |
| Wang 2019 [50] | 2019 | Retrospective cohort study | 2016–2018 | UAE + MTX + hysteroscopy | 44 | 31.84 (2.47) | _ | 100% | _ | 0% | UAE can effectively reduce intraoperative blood loss but increases the risk of postoperative complications, length of hospital stay, medical costs. | Fair | China |
| Xiao 2018 [48] | 2018 | Retrospective cohort study | 2011–2014 | UACE + curettage + MTX | 102 | 33.1 (4.6) | 51.19 (11.13) | 100% | _ | 0% | UACE combined with D&C is a useful measure for most Type 2 CSP cases in the first trimester. For Type 2 CSP cases in the second trimester, UACE before laparotomy could be a reasonable choice. | Fair | China |
| Xiao 2019 [49] | 2019 | Retrospective case–control study | 2014–2017 | UAE + D&C + hysteroscopy | 35 | 32.67 (6.96) | 52.5 (13.91) | 100% | _ | 0% | combination of UAE and surgery should be selected carefully because of its potential fertility complication. | Fair | China |
| Zhang 2019 [52] | 2019 | Retrospective cohort study | _ | UAE + curettage | 46 | 32.5 (4.7) | 48.7 (9.8) | 100% | _ | 0% | Compared to UAE, lauromacrogol–based sclerotherapy is a safe, effective, and economic approach in the pretreatment for uterine scar pregnancy. | Fair | China |
| Fahg 2009 [25] | 2009 | Prospective cohort study | 2004–2088 | UAE + curettage | 38 | 32.5 (4.8) | 53.35 (7.72) | 100% | _ | 0% | UAE followed by curettage is recommended to medical facilities where UAE is available. | Fair | China |
| Gao 2014 [28] | 2014 | Prospective cohort study | 2009–2012 | UAE + curettage | 93 | 33.4 (4.5) | 49.84 (7.72) | 94.62% | Treatment failure (n = 5) [needed additional interventions] | 0% | UAE combined with D&C within 24 hours was an effective and safe uterine preservation treatment for CSP. | Fair | China |
| Qian 2015 [42] | 2015 | RCT | 2008–2013 | UAE + curettage | 33 | 30.79 (4.29) | 51.33 (7.57) | 100% | _ | 0% | UAE plus curettage was successful in terminating a gestational sac type of CSP. | High | China |
| UAE + D&C + hysteroscopy | 33 | 32 (4.15) | 52 (11.14) | 90.91% | Treatment failure (n = 3) hemorrhage during surgery (n = 1) [Emergency hysterectomy] additional MTX therapy (n = 2) | 3.03% | |||||||
| Wang 2013 [47] | 2013 | Retrospective cohort study | 2007–2012 | UAE + curettage | 128 | 32.28 (4.76) | 48.64 (7.98) | 88.28% | Treatment failure (n = 15) Emergency hysterectomy (n = 5) | 11.72% | For CSP masses with a GA of 8 weeks or more and a diameter of 6 cm or more, the outcome of surgical evacuation after UAE tends to be unsatisfactory. | Fair | China |
| Zhuang 2009 [54] | 2009 | RCT | 2003–2007 | UAE + curettage | 37 | 32.23 (.65) | 51.24 (1.4) | 91.89% | Treatment failure (n = 3) Iodoform meche (n = 1) Readmitted due to bleeding (n = 2) | 0% | UAE followed by suction curettage seems to have more advantages than systemic MTX treatment and maybe a priority option. | Moderate | China |
| Cao 2014 [21] | 2014 | Retrospective cohort study | 2007–2012 | UAE + D&C + hysteroscopy | 52 | 33.3 (4.5) | 49.13 (14.74) | 98.08% | Treatment failure (n = 1) [Resection of the lower uterine segment] | 0% | UAE combined with D&C is a safe and efficient treatment for CSP. | Fair | China |
| Du 2015 [24] | 2015 | Retrospective cohort study | 2006–2012 | UAE + MTX + D&C | 175 | 32.44 (4.6) | 54.05 (14.04) | 96.57% | Treatment failure (n = 6) tamponade with iodoform gauze packs or an inflated balloon catheter (n = 3) emergency local CSP resection via laparotomy (n = 1) Emergency hysterectomy (n = 2) | 3.43% | Increased gestational age increases the risk of bleeding in CSP treated by UAE+MTX+D&C. | Fair | China |
| Huang 2015 [31] | 2015 | Retrospective cohort study | 2009–2014 | UAE + MTX + D&C | 31 | 32.42 (5.94) | 42.12 (6.32) | 100% | _ | 0% | UAE combined with MTX is a safe and efficient treatment of CSP. | Fair | China |
| Li 2011 [11] | 2011 | RCT | 2002–2009 | UAE + MTX + D&C | 31 | 34.15 (5.41) | 70.89 (35.94) | 83.87% | Treatment failure (n = 5) tamponade with iodoform gauze (n = 2) re–embolization (n = 3) | 0% | Arterial chemoembolization with MTX was more effective than systemic MTX treatment for termination of CSP. | Low | China |
| Liang 2010 [34] | 2010 | Retrospective cohort study | 2005–2009 | UAE + MTX + D&C | 42 | 31.3 (3.6) | 5–10.5 weeks | 100% | _ | 0% | The use of UAE for the treatment of CSP is tolerated well and has few complications. | Poor | China |
| Shen 2012 [44] | 2012 | Retrospective cohort study | 2008–2010 | UAE + MTX + D&C | 25 | 32.7 (6) | 55.45 (2.11) | 96.00% | Treatment failure (n = 1) [Hysterectomy] | 4.00% | UAE and MTX appears to be a safe and effective treatment for CSP and causes less morbidity than current approaches. | Fair | China |
| Wu 2012 [13] | 2012 | Retrospective cohort study | 2000–2010 | UAE + MTX + D&C | 16 | 33.09 (4.33) | 48.18 (11.68) | 100% | _ | 0% | UAE combined with intraarterial MTX infusion could be an effective and safe treatment for CSP. | Fair | China |
| Yang 2010 [51] | 2010 | Retrospective cohort study | 2003–2008 | UAE + MTX | 38 | 31.5 (7.25) | 47.73 (11.1) | 31.58% | Treatment failure (n = 26) Re–embolization (n = 2) Additional D&C (n = 24) | 7.89% | UAE combined with local MTX benefits women wishing to preserve fertility and is suitable for use as the primary treatment for CSP. | Fair | China |
| Zhu 2015 [53] | 2015 | Retrospective cohort study | 2014 | UAE + D&C + hysteroscopy | 46 | 31.4 (5.1) | 60.6 (16.4) | 100% | _ | 2.17% | UAE combined with suction curettage under hysteroscopic guidance is safe and effective in treating patients with CSP. | Fair | China |
| He 2014 [29] | 2014 | Retrospective cohort study | 2005–2010 | UAE + MTX + hysteroscopy | 25 | _ | _ | 100% | _ | 0% | Combination of laparoscopy and hysteroscopy is much safer and more effective than uterine curettage as a supplementary measure following the UAE management of CSP. | Fair | China |
| UAE + MTX + D&C | 33 | 78.79% | Treatment failure (n = 7) [underwent multiple curettages] | 6.10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchand, G.J.; Masoud, A.T.; Coriell, C.; Ulibarri, H.; Parise, J.; Arroyo, A.; Goetz, S.; Moir, C.; Moberly, A.; Govindan, M. Treatment of Cesarean Scar Ectopic Pregnancy in China with Uterine Artery Embolization—A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7393. https://doi.org/10.3390/jcm11247393
Marchand GJ, Masoud AT, Coriell C, Ulibarri H, Parise J, Arroyo A, Goetz S, Moir C, Moberly A, Govindan M. Treatment of Cesarean Scar Ectopic Pregnancy in China with Uterine Artery Embolization—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(24):7393. https://doi.org/10.3390/jcm11247393
Chicago/Turabian StyleMarchand, Greg J., Ahmed Taher Masoud, Catherine Coriell, Hollie Ulibarri, Julia Parise, Amanda Arroyo, Sydnee Goetz, Carmen Moir, Atley Moberly, and Malini Govindan. 2022. "Treatment of Cesarean Scar Ectopic Pregnancy in China with Uterine Artery Embolization—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 24: 7393. https://doi.org/10.3390/jcm11247393