
Characteristics of Sleep Disturbance in Patients with Long COVID: A Retrospective Observational Study in Japan
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Inclusion of Patients
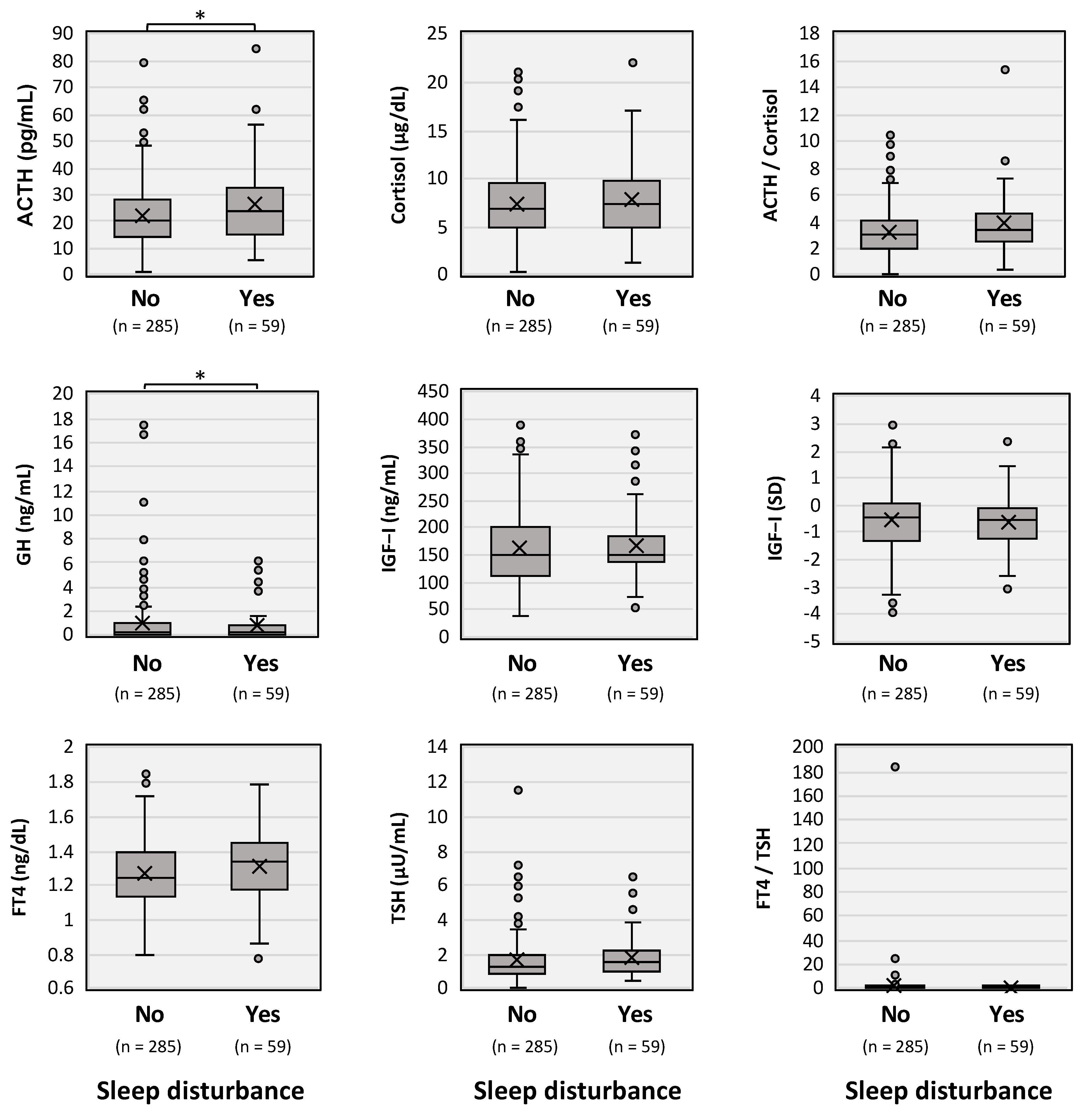
2.2. Endocrine Examination
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Carfi, A.; Bernabei, R.; Landi, F.; The Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Olde Hartman, T.C.; Rosmalen, J.G.M.; Lifelines Corona Research, I. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef]
- Almas, T.; Malik, J.; Alsubai, A.K.; Jawad Zaidi, S.M.; Iqbal, R.; Khan, K.; Ali, M.; Ishaq, U.; Alsufyani, M.; Hadeed, S.; et al. Post-acute COVID-19 syndrome and its prolonged effects: An updated systematic review. Ann. Med. Surg. 2022, 80, 103995. [Google Scholar] [CrossRef] [PubMed]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, Z.; Nami, M.; Leite, J.P.; Delbem, A.C.B.; Hyppolito, M.A.; Ghodratitoostani, I. Conceptual Framework for Insomnia: A Cognitive Model in Practice. Front. Neurosci. 2021, 15, 628836. [Google Scholar] [CrossRef] [PubMed]
- Huynh, G.; Nguyen, H.V.; Vo, L.Y.; Le, N.T.; Nguyen, H.T.N. Assessment of Insomnia and Associated Factors among Patients Who Have Recovered from COVID-19 in Vietnam. Patient Prefer. Adherence 2022, 16, 1637–1647. [Google Scholar] [CrossRef]
- Otsuka, Y.; Tokumasu, K.; Nakano, Y.; Honda, H.; Sakurada, Y.; Sunada, N.; Omura, D.; Hasegawa, K.; Hagiya, H.; Obika, M.; et al. Clinical Characteristics of Japanese Patients Who Visited a COVID-19 Aftercare Clinic for Post-Acute Sequelae of COVID-19/Long COVID. Cureus 2021, 13, e18568. [Google Scholar] [CrossRef]
- Sakurada, Y.; Sunada, N.; Honda, H.; Tokumasu, K.; Otsuka, Y.; Nakano, Y.; Hanayama, Y.; Furukawa, M.; Hagiya, H.; Otsuka, F. Serial Changes of Long COVID Symptoms and Clinical Utility of Serum Antibody Titers for Evaluation of Long COVID. J. Clin. Med. 2022, 11, 1309. [Google Scholar] [CrossRef]
- Nakano, Y.; Otsuka, Y.; Honda, H.; Sunada, N.; Tokumasu, K.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Ochi, K.; Hagiya, H.; et al. Transitional changes of fatigue-related symptoms due to long COVID: A single-center retrospective observational study in Japan. Medicina 2022, 58, 1393. [Google Scholar] [CrossRef] [PubMed]
- Sunada, N.; Honda, H.; Nakano, Y.; Yamamoto, K.; Tokumasu, K.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Otsuka, Y.; Obika, M.; et al. Hormonal trends in patients suffering from long COVID symptoms. Endocr. J. 2022, 69, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Otsuka, Y.; Sunada, N.; Tokumasu, K.; Nakano, Y.; Honda, H.; Sakurada, Y.; Hagiya, H.; Hanayama, Y.; Otsuka, F. Detection of Male Hypogonadism in Patients with Post COVID-19 Condition. J. Clin. Med. 2022, 11, 1955. [Google Scholar] [CrossRef] [PubMed]
- Soejima, Y.; Otsuka, Y.; Tokumasu, K.; Nakano, Y.; Harada, K.; Nakamoto, K.; Sunada, N.; Sakurada, Y.; Hasegawa, K.; Hagiya, H.; et al. Late-Onset Hypogonadism in a Male Patient with Long COVID Diagnosed by Exclusion of ME/CFS. Medicina 2022, 58, 536. [Google Scholar] [CrossRef]
- Kato, Y. Case Management of COVID-19 (Secondary Version). JMA J. 2021, 4, 191–197. [Google Scholar] [CrossRef]
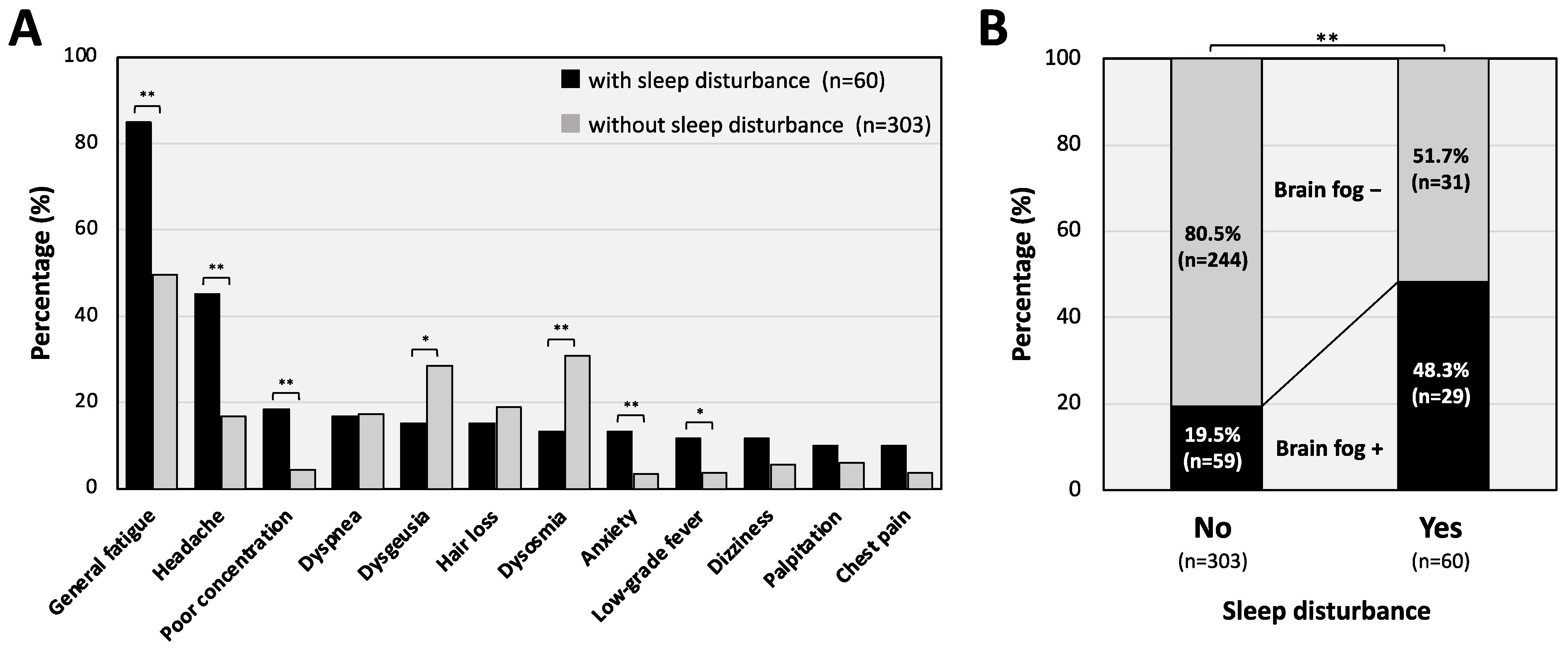
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID syndrome-associated brain fog. J. Med. Virol. 2022, 94, 979–984. [Google Scholar] [CrossRef]
- Isojima, T.; Shimatsu, A.; Yokoya, S.; Chihara, K.; Tanaka, T.; Hizuka, N.; Teramoto, A.; Tatsumi, K.I.; Tachibana, K.; Katsumata, N.; et al. Standardized centile curves and reference intervals of serum insulin-like growth factor-I (IGF-I) levels in a normal Japanese population using the LMS method. Endocr. J. 2012, 59, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Jahrami, H.; BaHammam, A.S.; Bragazzi, N.L.; Saif, Z.; Faris, M.; Vitiello, M.V. Sleep problems during the COVID-19 pandemic by population: A systematic review and meta-analysis. J. Clin. Sleep Med. 2021, 17, 299–313. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, C.A.; Rizvydeen, M.; Conroy, D.A.; O’Brien, L.M.; Gupta, G.; Somers, E.C.; Sharma, P.; Golob, J.L.; Troost, J.P.; Burgess, H.J. The prevalence and impact of pre-existing sleep disorder diagnoses and objective sleep parameters in patients hospitalized for COVID-19. J. Clin. Sleep Med. 2021, 17, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, L.B.; Foster, C.; Rawlinson, W.; Tedla, N.; Bull, R.A. Evolution of the SARS-CoV-2 omicron variants BA.1 to BA.5: Implications for immune escape and transmission. Rev. Med. Virol. 2022, 32, e2381. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef]
- Taquet, M.; Sillett, R.; Zhu, L.; Mendel, J.; Camplisson, I.; Dercon, Q.; Harrison, P.J. Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: An analysis of 2-year retrospective cohort studies including 1 284 437 patients. Lancet Psychiatry 2022, 9, 815–827. [Google Scholar] [CrossRef]
- Winkelman, J.W. Clinical practice. Insomnia Disorder. N. Engl. J. Med. 2015, 373, 1437–1444. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D.; Clinical Guidelines Committee of the American College of Physicians. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Clemente, I.; Sinatti, G.; Cirella, A.; Santini, S.J.; Balsano, C. Alteration of Inflammatory Parameters and Psychological Post-Traumatic Syndrome in Long-COVID Patients. Int. J. Environ. Res. Public Health 2022, 19, 7103. [Google Scholar] [CrossRef]
- Morin, C.M.; Bjorvatn, B.; Chung, F.; Holzinger, B.; Partinen, M.; Penzel, T.; Ivers, H.; Wing, Y.K.; Chan, N.Y.; Merikanto, I.; et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: An international collaborative study. Sleep Med. 2021, 87, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Tokumasu, K.; Honda, H.; Sunada, N.; Sakurada, Y.; Matsuda, Y.; Yamamoto, K.; Nakano, Y.; Hasegawa, T.; Yamamoto, Y.; Otsuka, Y.; et al. Clinical Characteristics of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Diagnosed in Patients with Long COVID. Medicina 2022, 58, 850. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Gubbi, S.; Koch, C.A. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J. Clin. Transl. Endocrinol. 2022, 27, 100284. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Cholevas, C.; Polyzoidis, K.; Politis, A. Long-COVID syndrome-associated brain fog and chemofog: Luteolin to the rescue. Biofactors 2021, 47, 232–241. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sleep Disturbance | p Value | |||
|---|---|---|---|---|
| Sleep disturbance, n (%) | No: 303 (83.5%) | Yes: 60 (16.5%) | ||
| Age, median (IQR) | 40 (26.5–50) | 38 (22.75–49.5) | 0.504 | |
| Gender, n (%) | Male 131 (43.2%) Female 172 (56.8%) | Male 33 (55%) Female 27 (45%) | 0.126 | |
| BMI, median (IQR) | 22.9 (20.4–26.0) | 23.5 (20.4–26.8) | 0.948 | |
| Smoking habit, n (%) | 145 (47.9%) | 26 (43.3%) | 0.617 | |
| Alcohol-drinking habit, n (%) | 109 (36.0%) | 26 (43.3%) | 0.352 | |
| Days after onset to first visit, median (IQR) | 88 (55.5–131.5) | 71.5 (50.75–102.75) | 0.0698 | |
| COVID-19-related clinical background | ||||
| Admission, n (%) | 80 (26.4%) | 13 (21.7%) | 0.545 | |
| Steroid and/or O2 therapy, n (%) | 43 (14.2%) | 9 (15%) | 1.00 | |
| Severity, n (%) | Mild | 236 (77.9%) | 52 (86.7%) | 0.174 |
| Moderate/Severe | 67 (22.1%) | 8 (13.3%) | ||
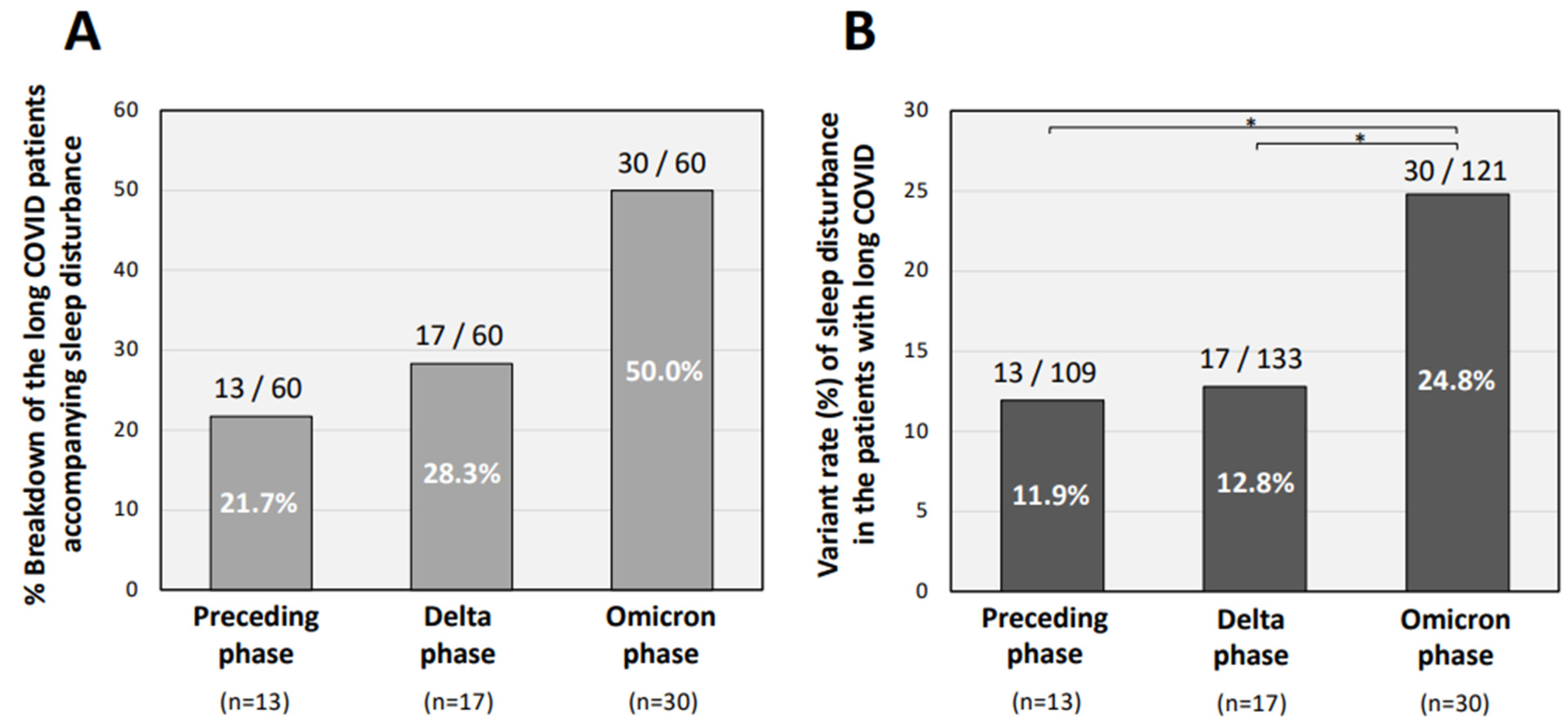
| Infected periods, n (%) | Preceding | 96 (31.7%) | 13 (21.7%) | 0.164 |
| Delta-dominant | 116 (38.3%) | 17 (28.3%) | 0.189 | |
| Omicron-dominant | 91 (30.0%) | 30 (50.0%) | ** <0.01 | |
| Vaccinations, n (%) | None | 136 (44.9%) | 25 (41.7%) | 0.752 |
| 2 doses or more | 138 (45.5%) | 30 (50.0%) | 0.572 | |
| Unknown | 5 (1.65%) | 1 (1.67%) | 1.00 | |
| Odds Ratio (95% Confidence Interval) | p Value | |
|---|---|---|
| Gender (male) | 1.58 (0.87–2.86) | 0.13 |
| Smoking habit | 0.70 (0.38–1.30) | 0.26 |
| Alcohol-drinking habit | 1.52 (0.83–2.80) | 0.17 |
| Severity (moderate and severe) | 0.41 (0.14–1.17) | 0.09 |
| Infected periods (Omicron phase) | 1.76 (0.62–4.97) | 0.29 |
| Vaccination (2 doses or more) | 0.90 (0.57–1.41) | 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sunada, N.; Nakano, Y.; Otsuka, Y.; Tokumasu, K.; Honda, H.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Omura, D.; Ochi, K.; et al. Characteristics of Sleep Disturbance in Patients with Long COVID: A Retrospective Observational Study in Japan. J. Clin. Med. 2022, 11, 7332. https://doi.org/10.3390/jcm11247332
Sunada N, Nakano Y, Otsuka Y, Tokumasu K, Honda H, Sakurada Y, Matsuda Y, Hasegawa T, Omura D, Ochi K, et al. Characteristics of Sleep Disturbance in Patients with Long COVID: A Retrospective Observational Study in Japan. Journal of Clinical Medicine. 2022; 11(24):7332. https://doi.org/10.3390/jcm11247332
Chicago/Turabian StyleSunada, Naruhiko, Yasuhiro Nakano, Yuki Otsuka, Kazuki Tokumasu, Hiroyuki Honda, Yasue Sakurada, Yui Matsuda, Toru Hasegawa, Daisuke Omura, Kanako Ochi, and et al. 2022. "Characteristics of Sleep Disturbance in Patients with Long COVID: A Retrospective Observational Study in Japan" Journal of Clinical Medicine 11, no. 24: 7332. https://doi.org/10.3390/jcm11247332