
Surgical Strategies to Dissect around the Superior Mesenteric Artery in Robotic Pancreatoduodenectomy
 ,
,
Abstract
:1. Introduction
2. Methods
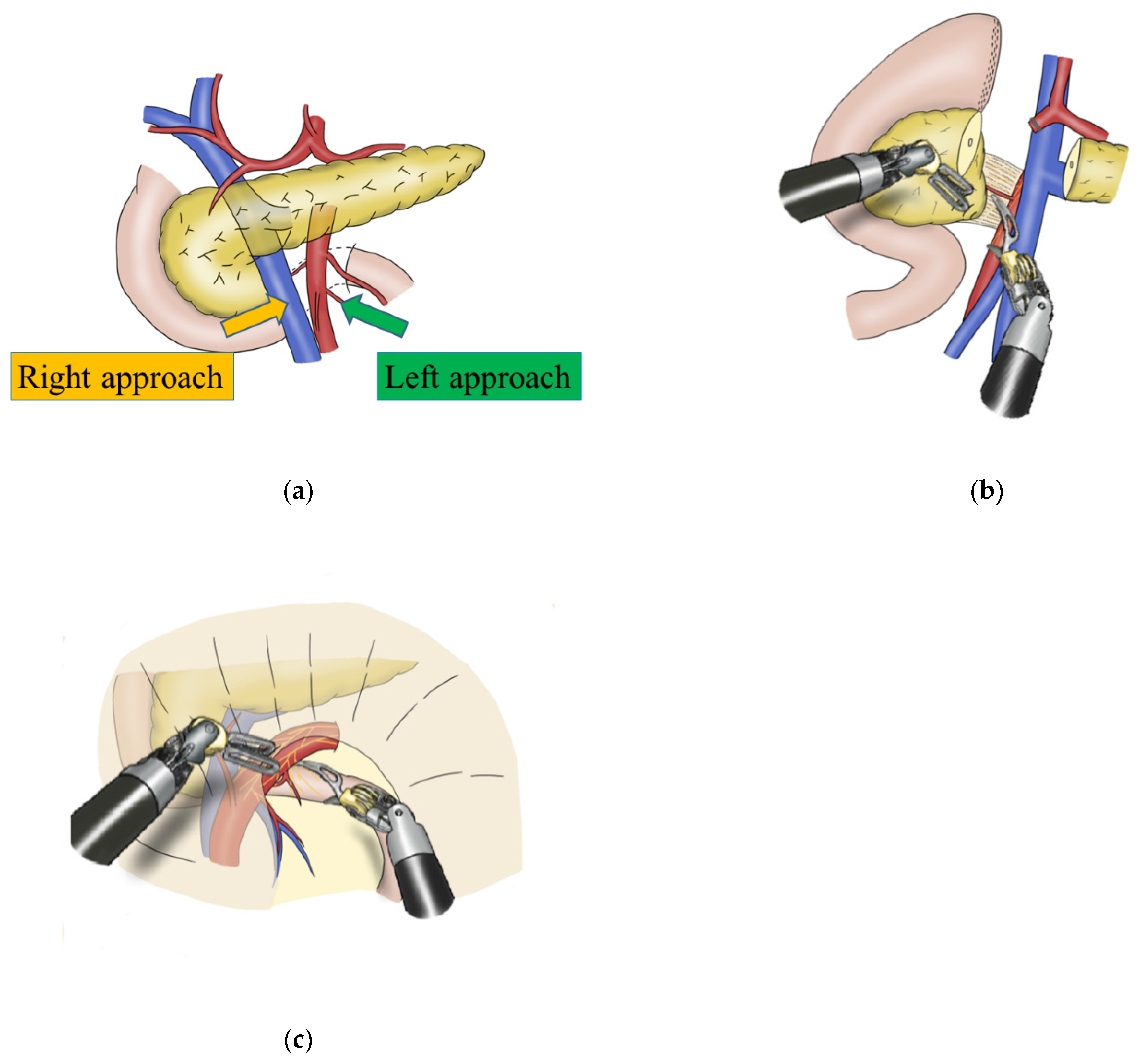
2.1. Surgical Approaches to the SMA in RPD
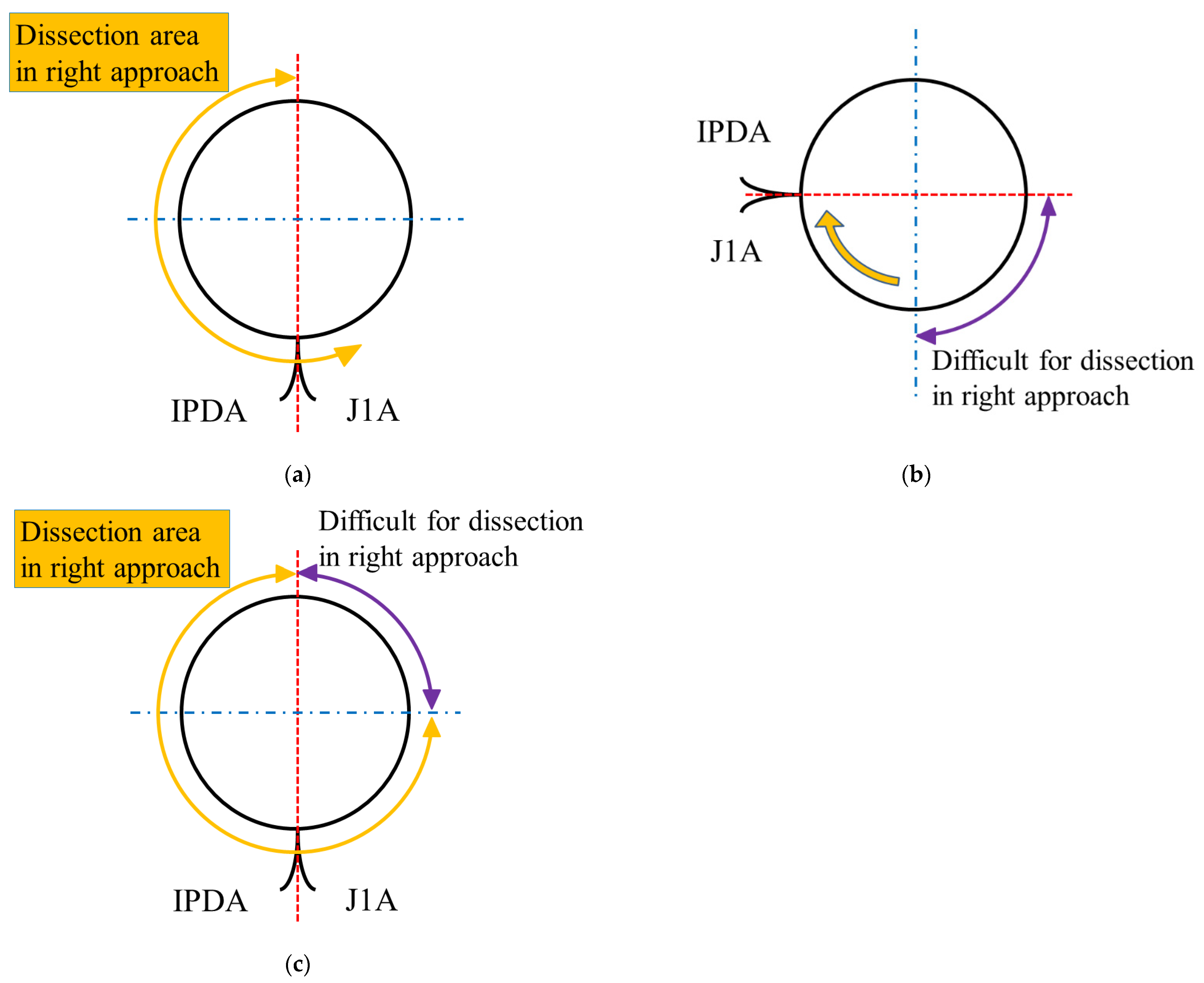
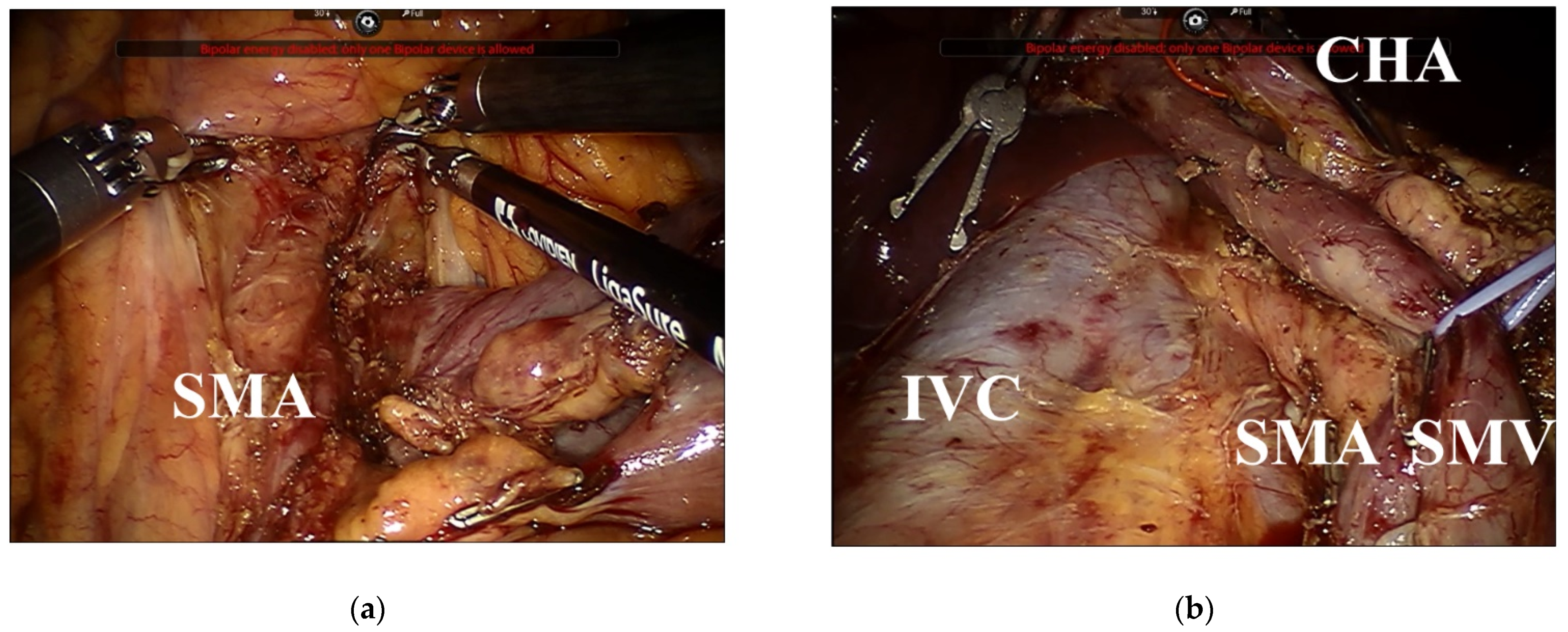
2.2. Dissection around the SMA Using the Right Approach
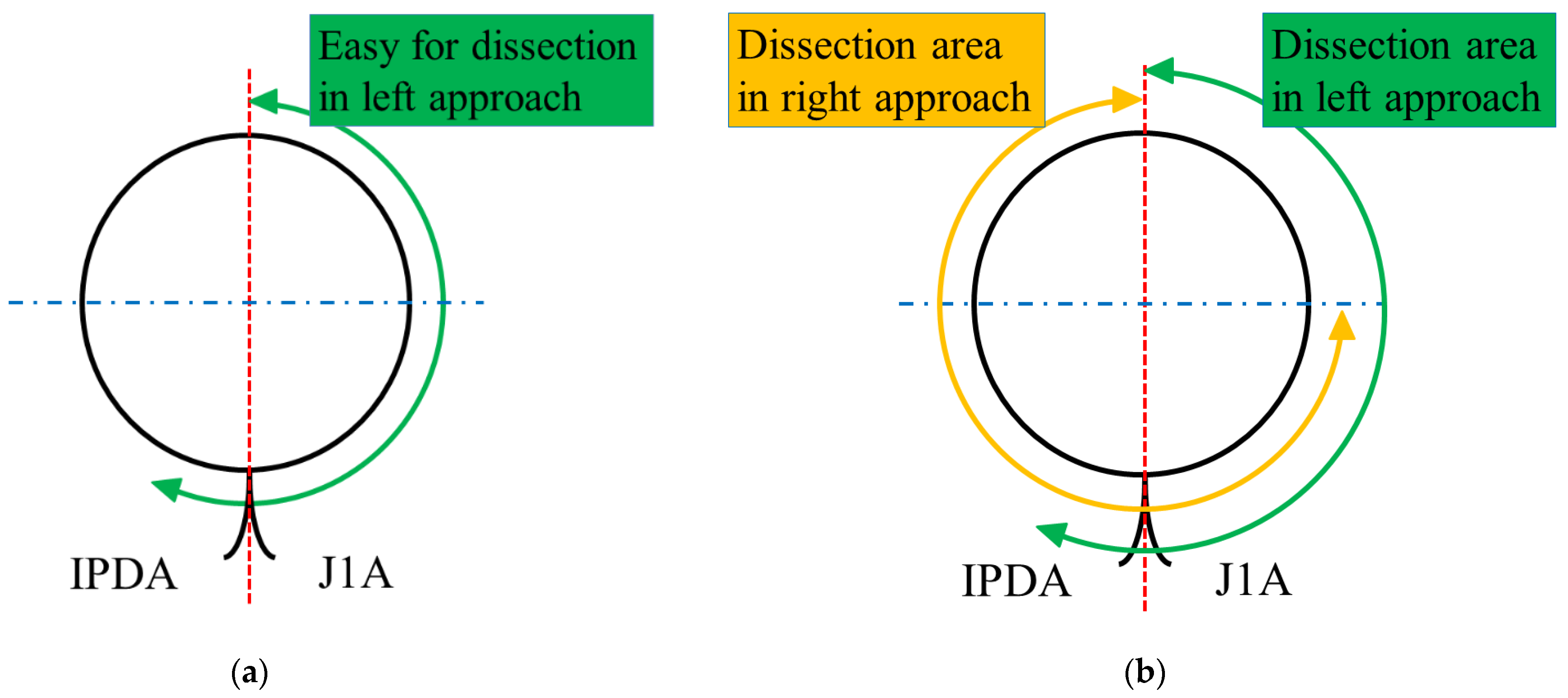
2.3. Dissection around the SMA Using a Combination of the Left and Right Approaches
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanjay, P.; Takaori, K.; Govil, S.; Shrikhande, S.V.; Windsor, J.A. ‘Artery-first’ approaches to pancreatoduodenectomy. Br. J. Surg. 2012, 99, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Yu, Z.; Ma, Z.; Deng, H.; Ren, W.; Shi, W.; Jiao, Z. Superior mesenteric artery first approach can improve the clinical outcomes of pancreaticoduodenectomy: A meta-analysis. Int. J. Surg. 2020, 73, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Asbun, H.J.; Moekotte, A.L.; Vissers, F.L.; Kunzler, F.; Cipriani, F.; Alseidi, A.; D’Angelica, M.I.; Balduzzi, A.; Bassi, C.; Björnsson, B.; et al. The Miami International Evidence-based Guidelines on Minimally Invasive Pancreas Resection. Ann. Surg. 2020, 271, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bhandare, M.S.; Parray, A.; Chaudhari, V.A.; Shrikhande, S.V. Minimally invasive surgery for pancreatic cancer-are we there yet?—A narrative review. Chin. Clin. Oncol. 2022, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Watanabe, Y.; Kozono, S.; Boggi, U.; Palanivelu, C.; Liu, R.; Wang, S.E.; He, J.; Nishino, H.; Ohtsuka, T.; et al. Surgical approaches to the superior mesenteric artery during minimally invasive pancreaticoduodenectomy: A systematic review. J. Hepatobiliary Pancreat. Sci. 2022, 29, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Min, S.K.; You, Y.; Choi, D.W.; Han, I.W.; Shin, S.H.; Yoon, S.; Jung, J.H.; Yoon, S.J.; Heo, J.S. Prognosis of pancreatic head cancer with different patterns of lymph node metastasis. J. Hepatobiliary Pancreat. Sci. 2022, 29, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Kumano, K.; Umeda, Y.; Yoshida, R.; Fuji, T.; Yasui, K.; Yagi, T.; Fujiwara, T. Surgical Strategies to Approaching the Splenic Artery in Robotic Distal Pancreatectomy. Anticancer Res 2022, 42, 4471–4476. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Umeda, Y.; Yoshida, R.; Yagi, T.; Fujiwara, T.; Zureikat, A.H.; Hogg, M.E.; Koerkamp, B.G. Surgical training model and safe implementation of robotic pancreatoduodenectomy in Japan: A technical note. World J. Surg. Oncol. 2021, 19, 55. [Google Scholar] [CrossRef] [PubMed]
- Zwart, M.J.W.; Nota, C.L.M.; de Rooij, T.; van Hilst, J.; Te Riele, W.W.; van Santvoort, H.C.; Hagendoorn, J.; Rinkes, I.; van Dam, J.L.; Latenstein, A.E.J.; et al. Outcomes of a Multicenter Training Program in Robotic Pancreatoduodenectomy (LAELAPS-3). Ann. Surg. 2021, 276, e886–e895. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Hosokawa, Y.; Sahara, Y.; Takishita, C.; Hijikata, Y.; Osakabe, H.; Nakajima, T.; Shirota, T.; Katsumata, K.; Nakamura, M.; et al. Approaching the superior mesenteric artery from the right side using the proximal-dorsal jejunal vein preisolation method during laparoscopic pancreaticoduodenectomy. Surg. Endosc. 2018, 32, 4044–4051. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Saiura, A.; Oba, A.; Kawakatsu, S.; Ono, Y.; Sato, T.; Mise, Y.; Ishizawa, T.; Takahashi, Y.; Ito, H. Optimal Extent of Superior Mesenteric Artery Dissection during Pancreaticoduodenectomy for Pancreatic Cancer: Balancing Surgical and Oncological Safety. J. Gastrointest. Surg. 2019, 23, 1373–1383. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indications | Advantages | Disadvantages | |
| Right approach | First option. | Commonly used in MIPD. Adequate working space. LN dissection mostly at the right side of the SMA. No need to lift the transverse colon. | Often difficult in patients with obesity. Difficult in patients with adhesions around the ligament of Treitz. Difficult to dissect at the left side of the SMA. |
| Left approach | LN dissection mostly at the left side of the SMA. Easy dissection around the ligament of Treitz, especially in patients with obesity. | Inadequate working space. Difficult to dissect at the right side of the SMA and uncinate process. Need to lift the transverse colon. | |
| Left and right approach | Second option. Considered for patients with obesity, adhesions, and malignant diseases requiring LN dissection around the SMA. | Circumferential LN dissection around the SMA. Easy dissection around the ligament of Treitz. | Need to lift the transverse colon during the left approach. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takagi, K.; Umeda, Y.; Yoshida, R.; Fuji, T.; Yasui, K.; Kimura, J.; Hata, N.; Mishima, K.; Yagi, T.; Fujiwara, T. Surgical Strategies to Dissect around the Superior Mesenteric Artery in Robotic Pancreatoduodenectomy. J. Clin. Med. 2022, 11, 7112. https://doi.org/10.3390/jcm11237112
Takagi K, Umeda Y, Yoshida R, Fuji T, Yasui K, Kimura J, Hata N, Mishima K, Yagi T, Fujiwara T. Surgical Strategies to Dissect around the Superior Mesenteric Artery in Robotic Pancreatoduodenectomy. Journal of Clinical Medicine. 2022; 11(23):7112. https://doi.org/10.3390/jcm11237112
Chicago/Turabian StyleTakagi, Kosei, Yuzo Umeda, Ryuichi Yoshida, Tomokazu Fuji, Kazuya Yasui, Jiro Kimura, Nanako Hata, Kento Mishima, Takahito Yagi, and Toshiyoshi Fujiwara. 2022. "Surgical Strategies to Dissect around the Superior Mesenteric Artery in Robotic Pancreatoduodenectomy" Journal of Clinical Medicine 11, no. 23: 7112. https://doi.org/10.3390/jcm11237112