


Association between COVID-19 Burden, Population Vaccination Status, and Urologic Oncology Surgery Volume: A National Multicenter Cross-Sectional Study
 , , , , , , , , , , and
, , , , , , , , , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Quantification of COVID-19 Restrictions
2.3. National Vaccination Rates
2.4. “COVID-19 Wave” Definition
2.5. Statistical Analysis
2.6. Institutional Review Board (IRB) Approvals
3. Results
3.1. Patient Characteristics
3.2. Correlations between New COVID-19 Cases in Israel and Monthly Urologic Oncology Surgical Volumes
3.3. Correlations between New COVID-19 Related Hospitalizations in Israel and Monthly Urologic Oncology Surgical Volumes
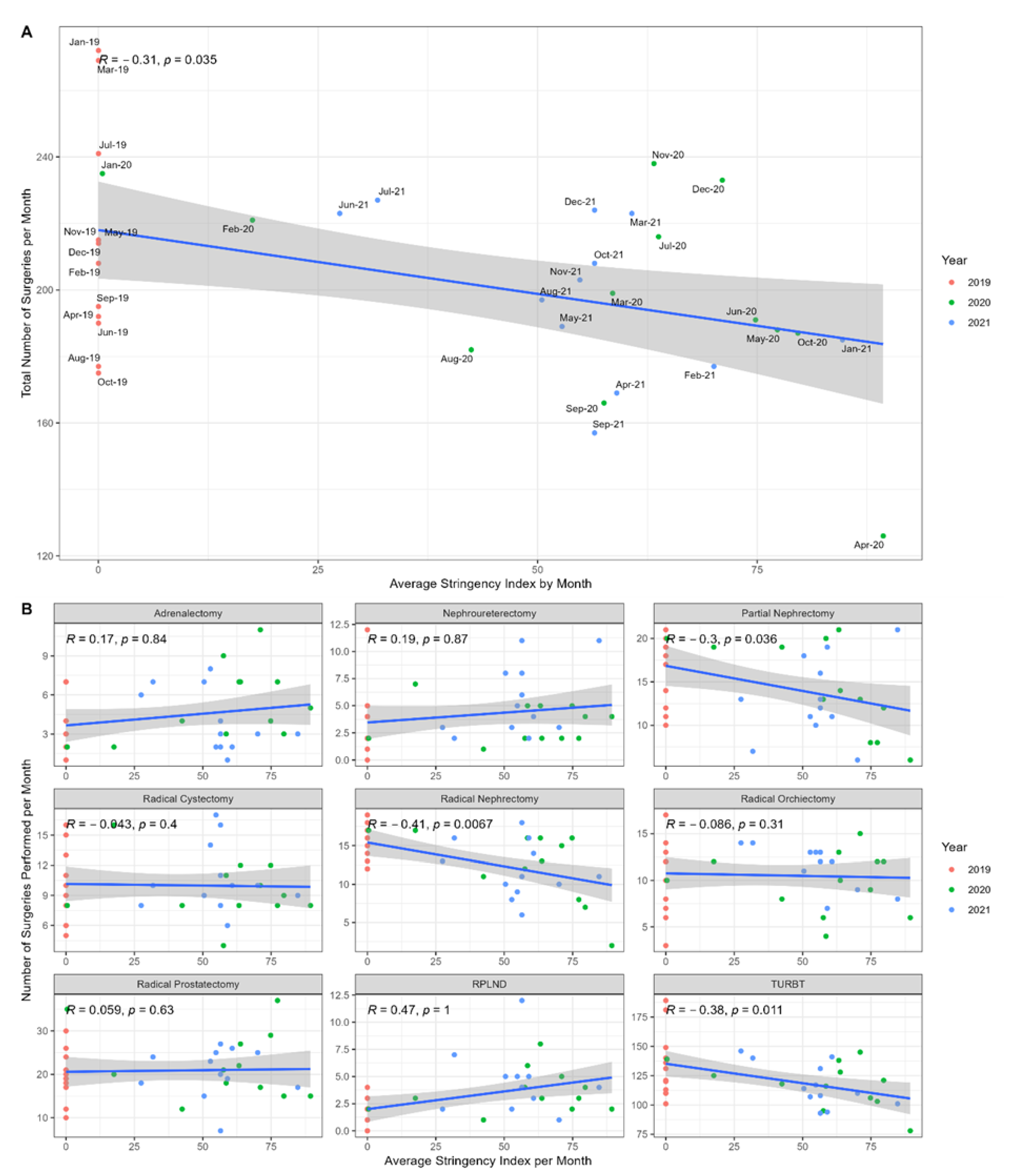
3.4. Correlations between the Average Monthly OSI in Israel and Monthly Urologic Oncology Surgical Volumes
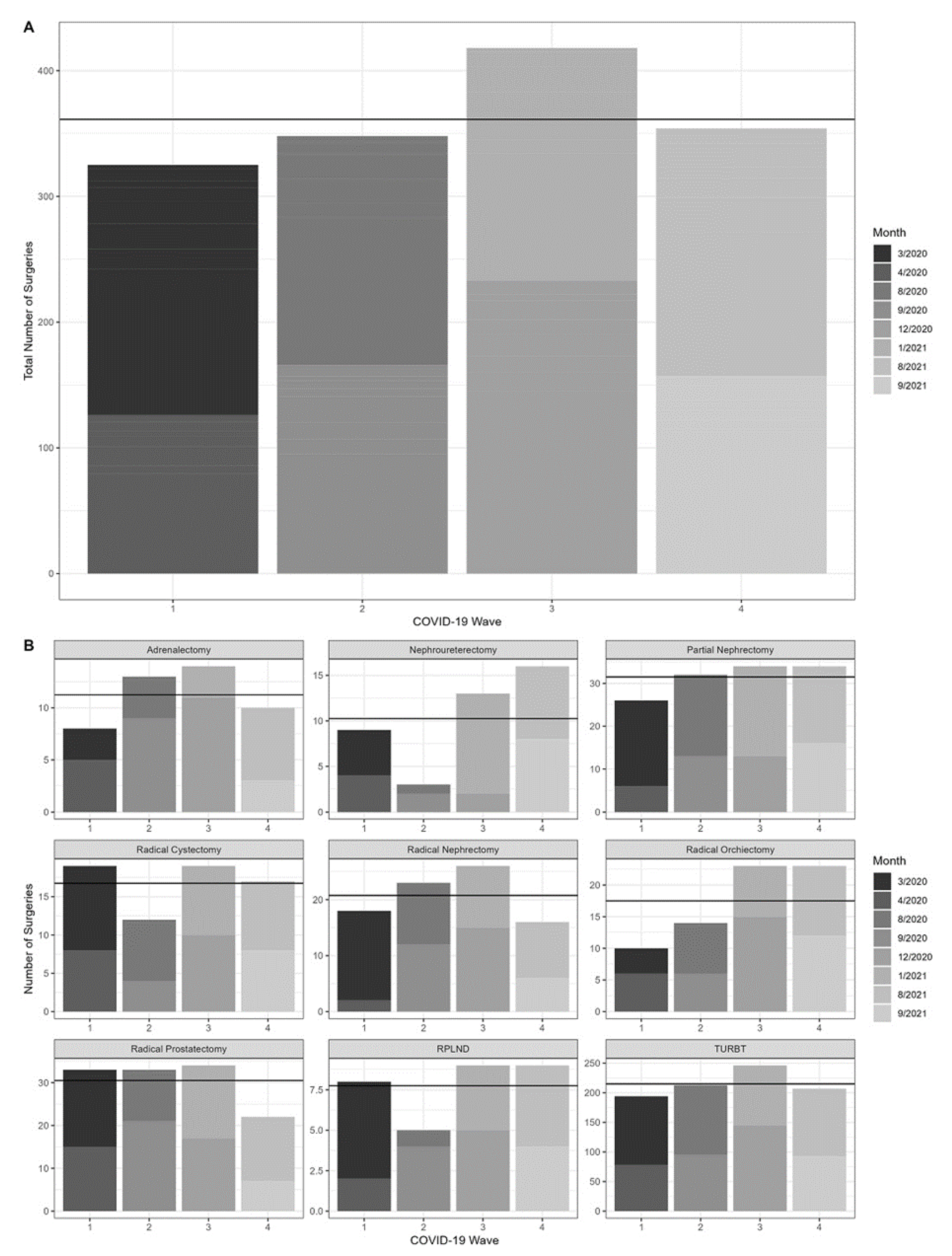
3.5. Changes in Urologic Oncology Surgery Volumes in Relation to COVID-19 Wave Progression
3.6. Correlations between the Cumulative First-Dose Vaccination Rate in Israel and the Monthly Surgical Volumes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iyengar, K.; Mabrouk, A.; Jain, V.K.; Venkatesan, A.; Vaishya, R. Learning opportunities from COVID-19 and future effects on health care system. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 943–946. [Google Scholar] [CrossRef] [PubMed]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Saqib, M.A.N.; Siddiqui, S.; Qasim, M.; Jamil, M.A.; Rafique, I.; Awan, U.A.; Ahmad, H.; Afzal, M.S. Effect of COVID-19 lockdown on patients with chronic diseases. Diabetes Metab Syndr Clin Res Rev. 2020, 14, 1621–1623. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Stöss, C.; Steffani, M.; Pergolini, I.; Hartmann, D.; Radenkovic, D.; Novotny, A.; Friess, H.; Müller, M.W. Impact of the COVID-19 Pandemic on Surgical Oncology in Europe: Results of a European Survey. Dig. Surg. 2021, 38, 259–265. [Google Scholar] [CrossRef]
- Johnson, B.A.; Waddimba, A.C.; Ogola, G.O.; Fleshman, J.W.; Preskitt, J.T. A systematic review and meta-analysis of surgery delays and survival in breast, lung and colon cancers: Implication for surgical triage during the COVID-19 pandemic. Am. J. Surg. 2021, 222, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Jones, M.E.; Broggio, J.; Loveday, C.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; Boyce, S.A.; Ward, P.; et al. Collateral damage: The impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann Oncol. 2020, 31, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, B.; Bex, A.; Dotan, Z.A.; Frydenberg, M.; Klotz, L.; Lotan, Y.; Schulman, C.C.; Tsaur, I.; Ramon, J. Trends in urologic oncology clinical practice and medical education under COVID-19 pandemic: An international survey of senior clinical and academic urologists. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 929.e1–929.e10. [Google Scholar] [CrossRef]
- Stensland, K.D.; Morgan, T.M.; Moinzadeh, A.; Lee, C.T.; Briganti, A.; Catto, J.W.; Canes, D. Considerations in the Triage of Urologic Surgeries During the COVID-19 Pandemic. Eur. Urol. 2020, 77, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; GORRG Group; et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organisation-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur. Urol. 2020, 78, 21–28. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balice, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- OxCGRT. OXCGRT/Covid-Policy-Tracker: Systematic Dataset of COVID-19 Policy, from Oxford University. GitHub. Available online: https://github.com/OxCGRT/covid-policy-tracker (accessed on 22 November 2022).
- Glasbey, J.; Ademuyiwa, A.; Adisa, A.; AlAmeer, E.; Arnaud, A.P.; Ayasra, F.; Minaya-Bravo, A.; Costas-Chavarri, A.; Edwards, J.; Elhadi, M.; et al. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar] [CrossRef]
- Ayala, A.; Villalobos Dintrans, P.; Elorrieta, F.; Castillo, C.; Vargas, C.; Maddaleno, M. Identification of COVID-19 Waves: Considerations for Research and Policy. Int. Env. Res. Public Health 2021, 18, 11058. [Google Scholar] [CrossRef]
- Datadashboard.health.gov.il. 2022. COVID-19 Data Tracker. Available online: https://datadashboard.health.gov.il/COVID-19/general (accessed on 29 July 2022).
- Gribkova, Y.; Davis, C.H.; Greenbaum, A.A.; Lu, S.; Berger, A.C. Effect of the COVID-19 pandemic on surgical oncology practice—Results of an SSO survey. J. Surg. Oncol. 2022, 125, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Guerrieri, R.; Rovati, L.; Dell’Oglio, P.; Galfano, A.; Ragazzoni, L.; Aseni, P. Impact of the COVID-19 Pandemic on Urologic Oncology Surgery: Implications for Moving Forward. J. Clin. Med. 2022, 11, 171. [Google Scholar] [CrossRef]
- Katims, A.B.; Razdan, S.; Eilender, B.M.; Wiklund, P.; Tewari, A.K.; Kyprianou, N.; Badani, K.K.; Mehrazin, R. Urologic oncology practice during COVID-19 pandemic: A systematic review on what can be deferrable vs. nondeferrable. Urol. Oncol. 2020, 38, 783–792. [Google Scholar] [CrossRef]
- Tulchiner, G.; Staudacherm, N.; Fritz, J.; Radmayr, C.; Culig, Z.; Horninger, W.; Pichler, R. The “COVID-19 Pandemic Gap” and Its Influence on Oncologic Outcomes of Bladder Cancer. Cancers 2021, 13, 1754. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Torr, B.; Jones, M.E.; Broggio, J.; Scott, S.; Loveday, C.; Garrett, A.; Gronthoud, F.; Nicol, D.L.; Jhanji, S.; et al. Effect of delays in the 2-week-wait cancer referral pathway during the COVID-19 pandemic on cancer survival in the UK: A modelling study. Lancet Oncol. 2020, 21, 1035–1044. [Google Scholar] [CrossRef]
- Culpan, M.; Keser, F.; Acar, H.C.; Otunctemur, A.; Kucuk, E.V.; Erdem, S.; Ozer, M.; Sen, U.T.; Degirmenci, E.; Ergul, R.; et al. Impact of delay in cystoscopic surveillance on recurrence and progression rates in patients with non-muscle-invasive bladder cancer during the COVID-19 pandemic. Int. J. Clin. Pract. 2021, 75, e14490. [Google Scholar] [CrossRef]
- Mano, R.; Vertosick, E.A.; Hakimi, A.A.; Sternberg, I.A.; Sjoberg, D.D.; Bernstein, M.; Dalbagni, G.; Coleman, J.A.; Russo, P. The effect of delaying nephrectomy on oncologic outcomes in patients with renal tumors greater than 4cm. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 239.e1–239.e8. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.M.A.; Bryan, R.T.; Dunn, J.A.; Begum, G.; Bathers, S.; Group on behalf of the WMUR. Delay and survival in bladder cancer. BJU Int. 2002, 89, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Gore, J.L.; Lai, J.; Setodji, C.M.; Litwin, M.S.; Saigal, C.S. Mortality increases when radical cystectomy is delayed more than 12 weeks. Cancer 2009, 115, 988–996. [Google Scholar] [CrossRef] [Green Version]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Rossman, H.; Shilo, S.; Meir, T.; Gorfine, M.; Shalit, U.; Segal, E. COVID-19 dynamics after a national immunization program in Israel. Nat. Med. 2021, 27, 1055–1061. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns—United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- Cantor, J.; Sood, N.; Bravata, D.M.; Pera, M.; Whaley, C. The impact of the COVID-19 pandemic and policy response on health care utilization: Evidence from county-level medical claims and cellphone data. J. Health Econ. 2022, 82, 102581. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amir, I.; Golan, S.; Frumer, M.; Sternberg, I.A.; Gildor, O.S.; Hoffman, A.; Shashar, R.; Mano, R.; Savin, Z.; Haifler, M.; et al. Association between COVID-19 Burden, Population Vaccination Status, and Urologic Oncology Surgery Volume: A National Multicenter Cross-Sectional Study. J. Clin. Med. 2022, 11, 7071. https://doi.org/10.3390/jcm11237071
Amir I, Golan S, Frumer M, Sternberg IA, Gildor OS, Hoffman A, Shashar R, Mano R, Savin Z, Haifler M, et al. Association between COVID-19 Burden, Population Vaccination Status, and Urologic Oncology Surgery Volume: A National Multicenter Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(23):7071. https://doi.org/10.3390/jcm11237071
Chicago/Turabian StyleAmir, Ido, Shay Golan, Michael Frumer, Itay A. Sternberg, Omri Schwarztuch Gildor, Azik Hoffman, Reut Shashar, Roy Mano, Ziv Savin, Miki Haifler, and et al. 2022. "Association between COVID-19 Burden, Population Vaccination Status, and Urologic Oncology Surgery Volume: A National Multicenter Cross-Sectional Study" Journal of Clinical Medicine 11, no. 23: 7071. https://doi.org/10.3390/jcm11237071