
Safe Service Delivery of a Complex Early Pregnancy Problem: Caesarean Scar Pregnancy
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
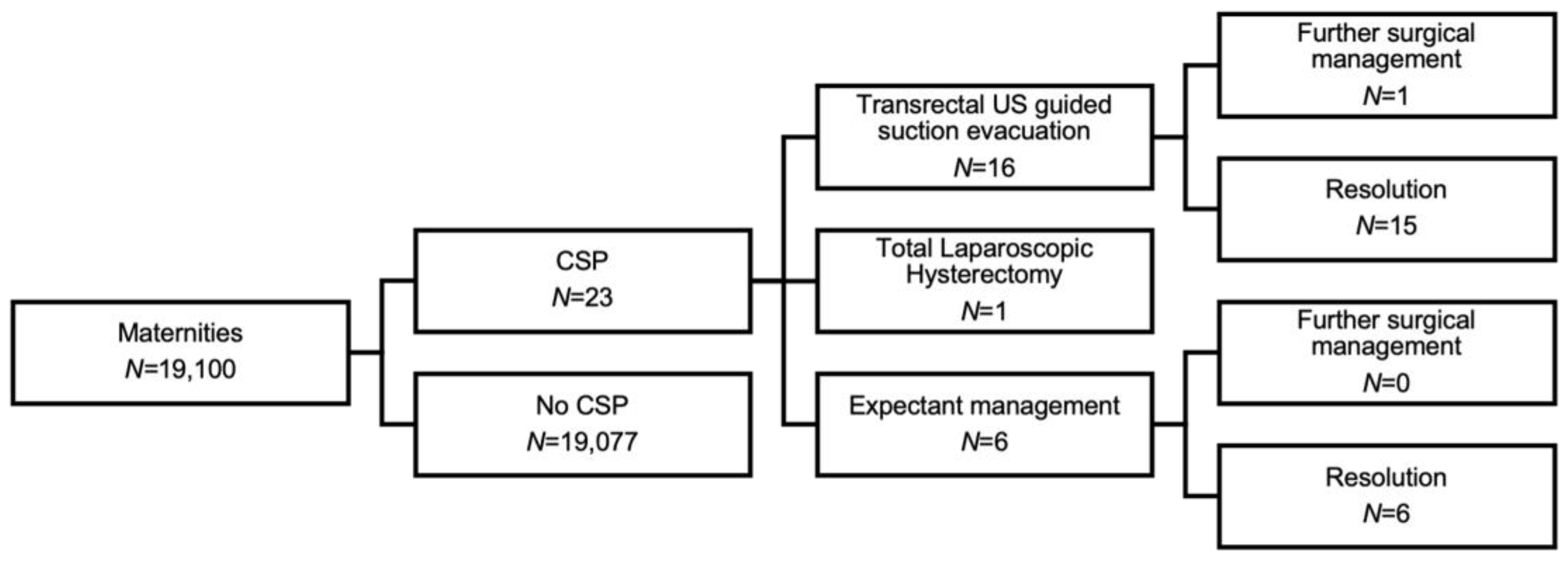
3. Results
3.1. Demographic Features
3.2. Symptoms Leading to Ultrasound Assessment
3.3. Diagnosis
3.4. Counselling
3.5. Management
3.6. Follow Up
3.7. Future Pregnancy
4. Discussion
- Patients in the first trimester of pregnancy with a history of CS and symptoms (bleeding ± pain) or a previous CSP, should be offered a transvaginal ultrasound scan from 6 weeks of pregnancy.
- If there is concern about low implantation close to the CS scar, the case should be reviewed in an early pregnancy multidisciplinary meeting led by a gynaecologist specialising in early pregnancy ultrasound. If suspicion is that of a CSP, the patient should have a detailed ultrasound assessment by a specialist gynaecologist.
- If the diagnosis of CSP is confirmed, the patient should be counselled about her options and given time to consider her wishes. The patient should have access to the clinical team following initial consultation.
- If surgical management is performed, intraoperative transrectal ultrasound guidance is crucial to reduce the risk of retained tissue, bleeding and uterine perforation. Post operative intrauterine haematoma is common and can be difficult to differentiate from retained products of conception. Therefore, objective sonographic evidence of complete uterine evacuation at the time of the procedure improves postoperative investigation and diagnosis.
- Following surgical management, patients should have access to the clinical team due to the risk of ongoing bleeding and infection. A follow-up transvaginal ultrasound should be performed after 6 weeks, with anticipation of resolution of an intrauterine haematoma. At this assessment, the myometrial defect from CS should be assessed. In cases of recurrent CSP and a large myometrial defect, surgical repair of the defect can be discussed.
- If a patient elects for expectant management of a live CSP, antenatal care should be provided in a tertiary centre with expectation of delivery by complex surgery at a preterm gestational age.
- All women should be offered psychological support following their pregnancy loss. Patients are given the email address of a specialist early pregnancy counsellor and directed to pregnancy loss charities.
- All women should be offered contraception if they do not have a desire for future pregnancy, or wish to delay future pregnancy.
- Women should be counselled about lifestyle interventions to reduce the risk to future pregnancy. Themes include folic acid use, diet and exercise with an aim of normalising BMI, and smoking cessation. Smoking is specifically harmful to pregnancy and is known to be associated with miscarriage[13], preterm birth[14], CSP [15], and other placental disorders of pregnancy[16] which underlies widespread international and national recommendation to reduce maternal smoking [17].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Visser, G.H.A.; Ayres-de-Campos, D.; Barnea, E.R.; de Bernis, L.; Di Renzo, G.C.; Vidarte, M.F.E.; Lloyd, I.; Nassar, A.H.; Nicholson, W.; Shah, P.K.; et al. FIGO position paper: How to stop the caesarean section epidemic. Lancet 2018, 392, 1286–1287. [Google Scholar] [CrossRef] [PubMed]
- Sandall, J.; Tribe, R.M.; Avery, L.; Mola, G.; Visser, G.H.A.; Homer, C.S.E.; Gibbons, D.; Kelly, N.M.; Kennedy, H.P.; Kidanto, H.; et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet 2018, 392, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Kwee, A.; Bots, M.L.; Visser, G.H.A.; Bruinse, H.W. Emergency peripartum hysterectomy: A prospective study in The Netherlands. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 124, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Diagnosis and Management of Ectopic Pregnancy. BJOG Int. J. Obstet. Gynaecol. 2016, 123, e15–e55. [CrossRef] [PubMed] [Green Version]
- Jordans, I.P.M.; Verberkt, C.; De Leeuw, R.A.; Bilardo, C.M.; Van Den Bosch, T.; Bourne, T.; Brolmann, H.A.M.; Dueholm, M.; Hehenkamp, W.J.K.; Jastrow, N.; et al. Definition and sonographic reporting system for Cesarean scar pregnancy in early gestation: Modified Delphi method. Ultrasound Obstet. Gynecol. 2022, 59, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Timor-Tritsch, I.E.; Monteagudo, A.; Santos, R.; Tsymbal, T.; Pineda, G.; Arslan, A.A. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am. J. Obstet. Gynecol. 2012, 207, 44.e1–44.e13. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Valentin, L.; Bourne, T.H.; Collins, W.P.; Verrelst, H.; Vergote, I. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: A consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound Obstet. Gynecol. 2000, 16, 500–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soleymani Majd, H.; Collins, S.L.; Addley, S.; Weeks, E.; Chakravarti, S.; Halder, S.; Alazzam, M. The modified radical peripartum cesarean hysterectomy (Soleymani-Alazzam-Collins technique): A systematic, safe procedure for the management of severe placenta accreta spectrum. Am. J. Obstet. Gynecol. 2021, 225, 175.e1–175.e10. [Google Scholar] [CrossRef] [PubMed]
- Jurkovic, D.; Knez, J.; Appiah, A.; Farahani, L.; Mavrelos, D.; Ross, J.A. Surgical treatment of Cesarean scar ectopic pregnancy: Efficacy and safety of ultrasound-guided suction curettage. Ultrasound Obstet. Gynecol. 2016, 47, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jauniaux, E.; Alfirevic, Z.; Bhide, A.G.; Belfort, M.A.; Burton, G.J.; Collins, S.L.; Dornan, S.; Jurkovic, D.; Kayem, G.; Silver, R.; et al. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG Int. J. Obstet. Gynaecol. 2019, 126, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Calì, G.; Timor-Tritsch, I.E.; Palacios-Jaraquemada, J.; Monteaugudo, A.; Buca, D.; Forlani, F.; Familiari, A.; Scambia, G.; Acharya, G.; D’Antonio, F. Outcome of Cesarean scar pregnancy managed expectantly: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2018, 51, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harb, H.; Knight, M.; Bottomley, C.; Overton, C.; Tobias, A.; Gallos, I.; Shehmar, M.; Farquharson, R.; Horne, A.; Latthe, P.; et al. Caesarean scar pregnancy in the UK: A national cohort study. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic review and meta-analysis of miscarriage and maternal exposure to tobacco smoke during pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- Gull, B.; Klerelid, V.; Jormeus, A.; Strandell, A. Potential risk factors for caesarean scar pregnancy: A retrospective case-control study. Hum. Reprod. Open 2021, 2021, hoab019. [Google Scholar] [CrossRef] [PubMed]
- Tobacco and Nicotine Cessation During Pregnancy: ACOG Committee Opinion Summary, Number 807. Obstet. Gynecol. 2020, 135, 1244–1246. [CrossRef] [PubMed]
- England, N. Saving Babies’ Lives Care Bundle Version Two. A Care Bundle for Reducing Perinatal Mortality. 2019. Available online: https://www.england.nhs.uk/wp-content/uploads/2019/03 (accessed on 17 October 2022).
- CSPregistry. Available online: https://csp-registry.com/ (accessed on 17 October 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Type of Pregnancy | Mean Sac Diameter (mm) or RPOC Mean (mm) | Crown Rump Length (mm) | Residual Myometrial Thickness (mm) | Colour Score (1–4) |
|---|---|---|---|---|---|
| 1 | PUV | 10 | NA | UK | UK |
| 2 | PUV | 33.1 | 2.5 | 5.4 | 2 |
| 3 | Live | 18.8 | 6.7 | 3.6 | 4 |
| 4 | Miscarriage | - | 24.7 | 3.2 | 3 |
| 5 | Live | 23.9 | 14.6 | 2.8 | 3 |
| 6 | RPOC (after PUV) | 18 | NA | 1.9 | 2 |
| 7 | PUV | 10.05 | NA | 2.3 | 2 |
| 8 | Live | 14 | 4.99 | 2.5 | 2 |
| 9 | RPOC (after PUV) | 7.7 | NA | 9.5 | 2 |
| 10 | Live | 10..7 | 3.56 | UK | 2 |
| 11 | PUV | 15.6 | NA | 3.6 | 2 |
| 12 | Live | 17.5 | 3.08 | 2.9 | 4 |
| 13 | PUV | 12.6 | NA | 3.3 | 4 |
| 14 | PUV | 22.8 | NA | 2.6 | 4 |
| 15 | Live | 18.4 | 21.46 | 4.3 | 2 |
| 16 | RPOC | 9.7 | NA | UK | 2 |
| 17 | Live | 8.4 | 2.7 | 2.7 | 4 |
| 18 | RPOC | 49.7 | NA | 2.0 | 1 |
| 19 | PUV | 5.2 | NA | UK | UK |
| 20 | Live | 12.9 | 4.7 | 2.7 | 4 |
| 21 | Live | 14 | UK | 5.3 | 4 |
| 22 | RPOC | 28.8 | NA | 1.6 | 4 |
| 23 | Miscarriage | 25.3 | 17.6 | 7.3 | 2 |
| Case | GA at Diagnosis (Days) | Type of Pregnancy | Type of CSP | Management | Blood Loss | Complication | Future Pregnancy |
|---|---|---|---|---|---|---|---|
| 1 | 38 | PUV | 2 | Expectant | NA | Yes | |
| 2 | 33 | PUV | 2 | Surgical | 200 | Yes | |
| 3 | 37 | Live | 1 | Surgical | 600 | Yes | |
| 4 | 48 | Miscarriage | 1 | Surgical | 2000 | Blood transfusion | NA |
| 5 | 54 | Live | 2 | Surgical | 300 | NA | |
| 6 | 43 | PUV | 1 | Expectant | NA | NA | |
| 7 | 39 | PUV | 2 | Expectant | NA | Blood transfusion | Yes |
| 8 | 53 | Live | 2 | Surgical | 50 | Yes | |
| 9 | 51 | PUV | 1 | Expectant | NA | Yes | |
| 10 | NA | Live | 2 | Surgical | 50 | NA | |
| 11 | 77 | PUV | 2 | Surgical | 50 | NA | |
| 12 | 41 | Live | 3 | Surgical | 100 | RPOC requiring hysterectomy | NA |
| 13 | NA | PUV | 1 | Surgical | 50 | Yes | |
| 14 | 17 | PUV | 1 | Surgical | 50 | Yes | |
| 15 | NA | Live | 1 | Surgical | 200 | NA | |
| 16 | 77 | RPOC | 1 | Expectant | NA | NA | |
| 17 | 45 | Live | 1 | Surgical | 100 | NA | |
| 18 | 79 | RPOC | 2 | Surgical | 1100 | NA | |
| 19 | 49 | PUV | 1 | Expectant | NA | NA | |
| 20 | 45 | Live | 1 | Surgical | 1000 | NA | |
| 21 | 52 | Live | 1 | Surgical | 50 | NA | |
| 22 | 60 | RPOC | 3 | Hysterectomy | 500 | NA | |
| 23 | 82 | Miscarriage | 1 | Surgical | 50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fourie, H.; El-Zibdeh, A.; Heppell, V.; Granne, I.; Lim, L.N.; Supramaniam, P.R. Safe Service Delivery of a Complex Early Pregnancy Problem: Caesarean Scar Pregnancy. J. Clin. Med. 2022, 11, 7063. https://doi.org/10.3390/jcm11237063
Fourie H, El-Zibdeh A, Heppell V, Granne I, Lim LN, Supramaniam PR. Safe Service Delivery of a Complex Early Pregnancy Problem: Caesarean Scar Pregnancy. Journal of Clinical Medicine. 2022; 11(23):7063. https://doi.org/10.3390/jcm11237063
Chicago/Turabian StyleFourie, Hanine, Ahmad El-Zibdeh, Victoria Heppell, Ingrid Granne, Lee Nai Lim, and Prasanna Raj Supramaniam. 2022. "Safe Service Delivery of a Complex Early Pregnancy Problem: Caesarean Scar Pregnancy" Journal of Clinical Medicine 11, no. 23: 7063. https://doi.org/10.3390/jcm11237063