
Dual Anti-Glomerular Basement Membrane and Anti-Neutrophil Cytoplasmic Antibodies—Positive Rapidly Progressive Glomerulonephritis with Rheumatoid Arthritis and Sjogren’s Syndrome: A Case Report and Literature Review
 ,
, {kind=link}
Abstract
:1. Introduction
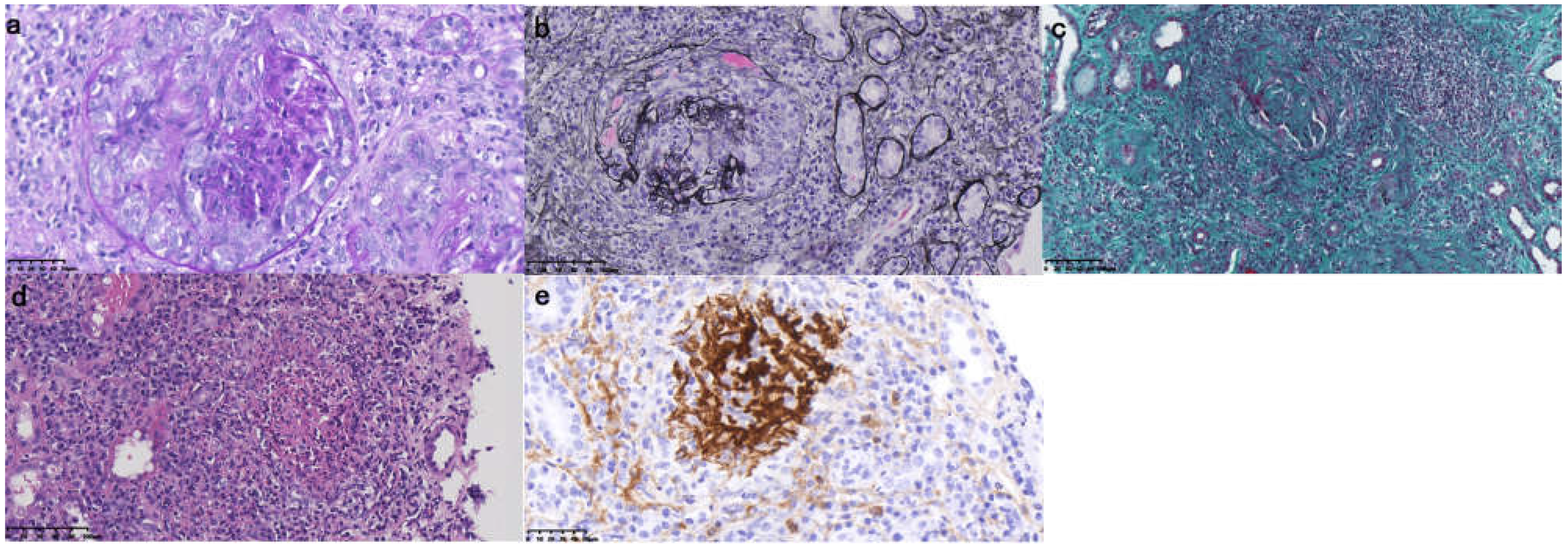
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Icardi, A.; Araghi, P.; Ciabattoni, M.; Romano, U.; Lazzarini, P.; Bianchi, G. Kidney involvement in rheumatoid arthritis. Reumatismo 2003, 55, 76–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.J.; Wu, H.S.; Chu, T.S. Anti-neutrophil Cytoplasmic Antibody-associated Pauci-immune Crescentic Glomerulonephritis Complicating Sjogren’s Syndrome. J. Formos. Med. Assoc. 2011, 110, 473–477. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, D.J.; Short, C.D.; Brenchley, P.E.C.; Lawler, W.; Ballardie, F.W. Sequential development of systemic vasculitis with anti-neutrophil cytoplasmic antibodies complicating anti-glomerular basement membrane disease. Clin. Nephrol. 1989, 32, 251. [Google Scholar] [PubMed]
- Rutgers, A.; Slot, M.; Paassen, P.V.; Vriesman, P.V.B.; Heeringa, P.; Tervaert, J.W.C. Coexistence of Anti-Glomerular Basement Membrane Antibodies and Myeloperoxidase-ANCAs in Crescentic Glomerulonephritis. Am. J. Kidney Dis. 2005, 46, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Mcadoo, S.P.; Tanna, A.; Hrušková, Z.; Holm, L.; Weiner, M.; Arulkumaran, N.; Kang, A.; Satrapová, V.; Levy, J.; Ohlsson, S.; et al. Patients double-seropositive for ANCA and anti-GBM antibodies have varied renal survival, frequency of relapse, and outcomes compared to single-seropositive patients. Kidney Int. 2017, 92, 693–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yang, R.; Cui, Z.; Chen, M.; Zhao, M.-H.; Wang, H.-Y. Characteristics and outcome of Chinese patients with both antineutrophil cytoplasmic antibody and anti-glomerular basement membrane antibodies. Nephron Clin. Pract. 2007, 107, c56–c62. [Google Scholar] [CrossRef] [PubMed]
- Balderia, P.G.; Andeen, N.; Jefferson, J.A. Characteristics and Outcomes of Patients with Anti-Glomerular Basement Membrane Antibody Disease and Anti-Neutrophil Cytoplasmic Antibodies. Curr. Rheumatol. Rev. 2019, 15, 224–228. [Google Scholar] [CrossRef] [PubMed]
- François, H.; Mariette, X. Renal involvement in Sjögren’s syndrome. Nephrol. Ther. 2020, 16, 440–452. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, M.; Luppi, F.; Sambataro, G.; Villegas, D.C.; Cerri, S.; Tomietto, P.; Cassone, G.; Bocchino, M.; Atienza-Mateo, B.; Cameli, P.; et al. Interstitial Lung Disease and Anti-Myeloperoxidase Antibodies: Not a Simple Association. J. Clin. Med. 2021, 10, 2548. [Google Scholar] [CrossRef] [PubMed]
- Kurita, N.; Mise, N.; Fujii, A.; Mori, M.; Sai, K.; Nishi, T.; Suzuki, T.; Tagawa, H.; Sugimoto, Y. Myeloperoxidase-antineutrophil cytoplasmic antibody-associated crescentic glomerulonephritis with rheumatoid arthritis: A comparison of patients without rheumatoid arthritis. Clin. Exp. Nephrol. 2010, 14, 325. [Google Scholar] [CrossRef] [PubMed]
- Spoerl, D.; Pers, Y.M.; Jorgensen, C. Anti-neutrophil cytoplasmic antibodies in rheumatoid arthritis: Two case reports and review of the literature. Allergy Asthma Clin. Immunol. Off. J. Can. Soc. Allergy Clin. Immunol. 2012, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustila, A.; Paimela, L.; Leirisalo-Repo, M.; Huhtala, H.; Miettinen, A. Antineutrophil cytoplasmic antibodies in patients with early rheumatoid arthritis: An early marker of progressive erosive disease. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2000, 43, 1371–1377. [Google Scholar] [CrossRef]
- Mustila, A.; Korpel, M.; Mustonen, J.; Helin, H.; Huhtala, H.; Soppi, E.; Pasternack, A.; Miettinen, A. Perinuclear antineutrophil cytoplasmic antibody in rheumatoid arthritis. A marker of severe disease with associated nephropathy. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1997, 40, 710–717. [Google Scholar] [CrossRef]
- Draibe, J.; Salama, A.D. Association of ANCA associated vasculitis and rheumatoid arthritis: A lesser recognized overlap syndrome. SpringerPlus 2015, 4, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos-Casals, M.; Nardi, N.; Brito-Zerón, P.; Aguiló, S.; Gil, V.; Delgado, G.; Bové, A.; Font, J. Atypical Autoantibodies in Patients with Primary Sjogren Syndrome: Clinical Characteristics and Follow-Up of 82 Cases. Semin. Arthritis Rheum. 2006, 35, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Choi, H.; Kim, M.K.; Jung, S.M.; Song, J.J.; Park, Y.-B.; Lee, S.-W. Can antineutrophil cytoplasmic antibody positivity at diagnosis predict the poor outcomes of Sjogren’s syndrome? Rheumatol. Int. 2019, 40, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Guellec, D.; Gall, C.L.; Groh, M.; Hachulla, E.; Karrase, A.; Charles, P.; Dunogué, B.; Abad, S.; Alvarez, F.; Gérard, F.; et al. ANCA-associated vasculitis in patients with primary Sjogren’s syndrome: Detailed analysis of 7 new cases and systematic literature review. Autoimmun. Rev. 2015, 14, 742–750. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, T.; Zhi, H.; Liu, Y.; Zhang, S.; Song, Z.; Li, Y. Dual Anti-Glomerular Basement Membrane and Anti-Neutrophil Cytoplasmic Antibodies—Positive Rapidly Progressive Glomerulonephritis with Rheumatoid Arthritis and Sjogren’s Syndrome: A Case Report and Literature Review. J. Clin. Med. 2022, 11, 6793. https://doi.org/10.3390/jcm11226793
Cheng T, Zhi H, Liu Y, Zhang S, Song Z, Li Y. Dual Anti-Glomerular Basement Membrane and Anti-Neutrophil Cytoplasmic Antibodies—Positive Rapidly Progressive Glomerulonephritis with Rheumatoid Arthritis and Sjogren’s Syndrome: A Case Report and Literature Review. Journal of Clinical Medicine. 2022; 11(22):6793. https://doi.org/10.3390/jcm11226793
Chicago/Turabian StyleCheng, Ting, Huiwen Zhi, Yunxiao Liu, Shengxiao Zhang, Ziyi Song, and Yafeng Li. 2022. "Dual Anti-Glomerular Basement Membrane and Anti-Neutrophil Cytoplasmic Antibodies—Positive Rapidly Progressive Glomerulonephritis with Rheumatoid Arthritis and Sjogren’s Syndrome: A Case Report and Literature Review" Journal of Clinical Medicine 11, no. 22: 6793. https://doi.org/10.3390/jcm11226793