
Reversible Bronchial Obstruction in Primary Ciliary Dyskinesia
 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lucas, J.S.; Davis, S.D.; Omran, H.; Shoemark, A. Primary ciliary dyskinesia in the genomics age. Lancet Respir. Med. 2020, 8, 202–216. [Google Scholar] [CrossRef]
- Lucas, J.S.; Barbato, A.; Collins, S.A.; Goutaki, M.; Behan, L.; Caudri, D.; Dell, S.; Eber, E.; Escudier, E.; Hirst, R.A.; et al. European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur. Respir. J. 2017, 49, 1601090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piatti, G.; De Santi, M.M.; Farolfi, A.; Zuccotti, G.V.; D’Auria, E.; Patria, M.F.; Torretta, S.; Consonni, D.; Ambrosetti, U. Exacerbations and Pseudomonas aeruginosa colonization are associated with altered lung structure and function in primary ciliary dyskinesia. BMC Pediatr. 2020, 20, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousquet, J.; Jeffery, P.K.; Busse, W.W.; Johnson, M.; Vignola, A.M. Asthma from Bronchoconstriction to Airways Inflammation and Remodeling. Am. J. Respir. Crit. Care Med. 2000, 161, 1720–1745. [Google Scholar] [CrossRef] [Green Version]
- Koh, Y.Y.; Park, Y.; Jeong, J.H.; Kim, C.K.; Min, Y.G.; Chi, J.G. The effect of regular salbutamol on lung function and bronchial responsiveness in patients with primary ciliary dyskinesia. Chest 2000, 117, 427–433. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.A.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.E.; Coates, A.; Van Der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [Green Version]
- Phillips, G.E.; Thomas, S.; Heather, S.; Bush, A. Airway response of children with primary ciliary dyskinesia to exercise and β2-agonist challenge. Eur. Respir. J. 1998, 11, 1389–1391. [Google Scholar] [CrossRef] [Green Version]
- Levine, H.; Cohen-Cymberknoh, M.; Klein, N.; Hoshen, M.; Mussaffi, H.; Stafler, P.; Breuer, O.; Kerem, E.; Blau, H. Reversible airway obstruction in cystic fibrosis: Common, but not associated with characteristics of asthma. J. Cyst. Fibros. 2016, 15, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Galodé, F.; Ladipo, O.; Andrieux, A.; Feghali, H.; Bui, S.; Fayon, M. Prevalence and Determinants of Wheezing and Bronchodilatation in Children with Cystic Fibrosis: A Retrospective Cohort Study. Front. Pediatr. 2022, 10, 856840. [Google Scholar] [CrossRef]
- Eggleston, P.A.; Rosenstein, B.J.; Stackhouse, C.M.; Alexander, M.F. Airway Hyperreactivity in Cystic Fibrosis. Chest 1988, 94, 360–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Haren, E.H.; Lammers, J.W.; Festen, J.; Van Herwaarden, C.L. Bronchial vagal tone and responsiveness to histamine, exercise and bronchodilators in adult patients with cystic fibrosis. Eur. Respir. J. 1992, 5, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Katoch, C.S.; Vardhan, V.; Chopra, M.; Singh, S.; Ahuja, N. Functional impairment in bronchiectasis: Spirometry parameters versus St. George’s Respiratory Questionnaire scores: Any co-relation? Lung India 2021, 38, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Gao, Y.H.; Xu, G.; Li, H.M.; Yuan, J.J.; Zheng, J.P.; Chen, R.C.; Zhong, N.S. Bronchodilator response in adults with bronchiectasis: Correlation with clinical parameters and prognostic implications. J. Thorac. Dis. 2016, 8, 14–23. [Google Scholar] [CrossRef] [PubMed]
- King, P.T.; Daviskas, E. Pathogenesis and diagnosis of bronchiectasis. Breathe 2010, 6, 342–351. [Google Scholar] [CrossRef]
- Bulcun, E.; Arslan, M.; Ekici, A.; Ekici, M. Quality of life and bronchial hyper-responsiveness in subjects with bronchiectasis: Validation of the seattle obstructive lung disease questionnaire in bronchiectasis. Respir. Care 2015, 60, 1616–1623. [Google Scholar] [CrossRef] [Green Version]
- Sevgili, S.; Hasanoğlu, H.C.; Karalezli, A.; Er, M. Bronchial reversibility in the patients with bronchiectasis. Tuberk. Toraks 2009, 57, 38–47. [Google Scholar]
- Frohock, J.I.; Wijkstrom-Frei, C.; Salathe, M. Effects of albuterol enantiomers on ciliary beat frequency in ovine tracheal epithelial cells. J. Appl. Physiol. 2002, 92, 2396–2402. [Google Scholar] [CrossRef] [Green Version]
- Strippoli, M.P.; Frischer, T.; Barbato, A.; Snijders, D.; Maurer, E.; Lucas, J.S.; Eber, E.; Karadag, B.; Pohunek, P.; Zivkovic, Z.; et al. Management of primary ciliary dyskinesia in European children: Recommendations and clinical practice. Eur. Respir. J. 2012, 39, 1482–1491. [Google Scholar] [CrossRef] [Green Version]
- Dehlink, E.; Richardson, C.; Marsh, G.; Lee, K.; Jamalzadeh, A.; Bush, A.; Hogg, C.; Carr, S.B. Are inhaled corticosteroids prescribed rationally in primary ciliary dyskinesia? Eur. Respir. J. 2018, 51, 1702221. [Google Scholar] [CrossRef]
- Kobbernagel, H.E.; Buchvald, F.F.; Haarman, E.G.; Casaulta, C.; Collins, S.A.; Hogg, C.; Kuehni, C.E.; Lucas, J.S.; Moser, C.E.; Quittner, A.L.; et al. Efficacy and safety of azithromycin maintenance therapy in primary ciliary dyskinesia (BESTCILIA): A multicentre, double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir. Med. 2020, 8, 493–505. [Google Scholar] [CrossRef]
- Kanoh, S.; Rubin, B.K. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin. Microbiol. Rev. 2010, 23, 590–615. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total n = 46 (100%) | Without Airway Reversibility n = 20 (43.5%) | With Airway Reversibility n = 26 (56.5%) | p-Value | |
|---|---|---|---|---|
| Sex (female) | 20 (43.5%) | 7 (35.0%) | 13 (50.0%) | 0.309 |
| Ethnicity (n = 29/46, 63%) | ||||
| Jewish | 13 (44.8%) | 7 (58.3%) | 6 (35.3%) | |
| Arabic | 15 (51.7%) | 5 (41.7%) | 10 (58.8%) | 0.379 |
| Other | 1 (3.4%) | 0 | 1 (5.9%) | |
| Consanguineous (n = 28/46, 61%) | 14 (50.0%) | 6 (50.0%) | 8 (50.0%) | 1.000 |
| Height (cm) (mean (SD)) | 149 (19.6) | 146.7 (22.0) | 151.5 (16.3) | 0.24 |
| Weight (kg) (mean (SD)) | 44.6 (18.3) | 42.9 (20.2) | 46.6 (16.0) | 0.345 |
| BMI (kg/m2) (mean (SD)) | 19.1 (3.9) | 18.6 (3.9) | 19.7 (3.8) | 0.899 |
| Total n = 46 (100%) | Without Airway Reversibility n = 20 (43.5%) | With Airway Reversibility n = 26 (56.5%) | p-Value | |
|---|---|---|---|---|
| Spirometry: | ||||
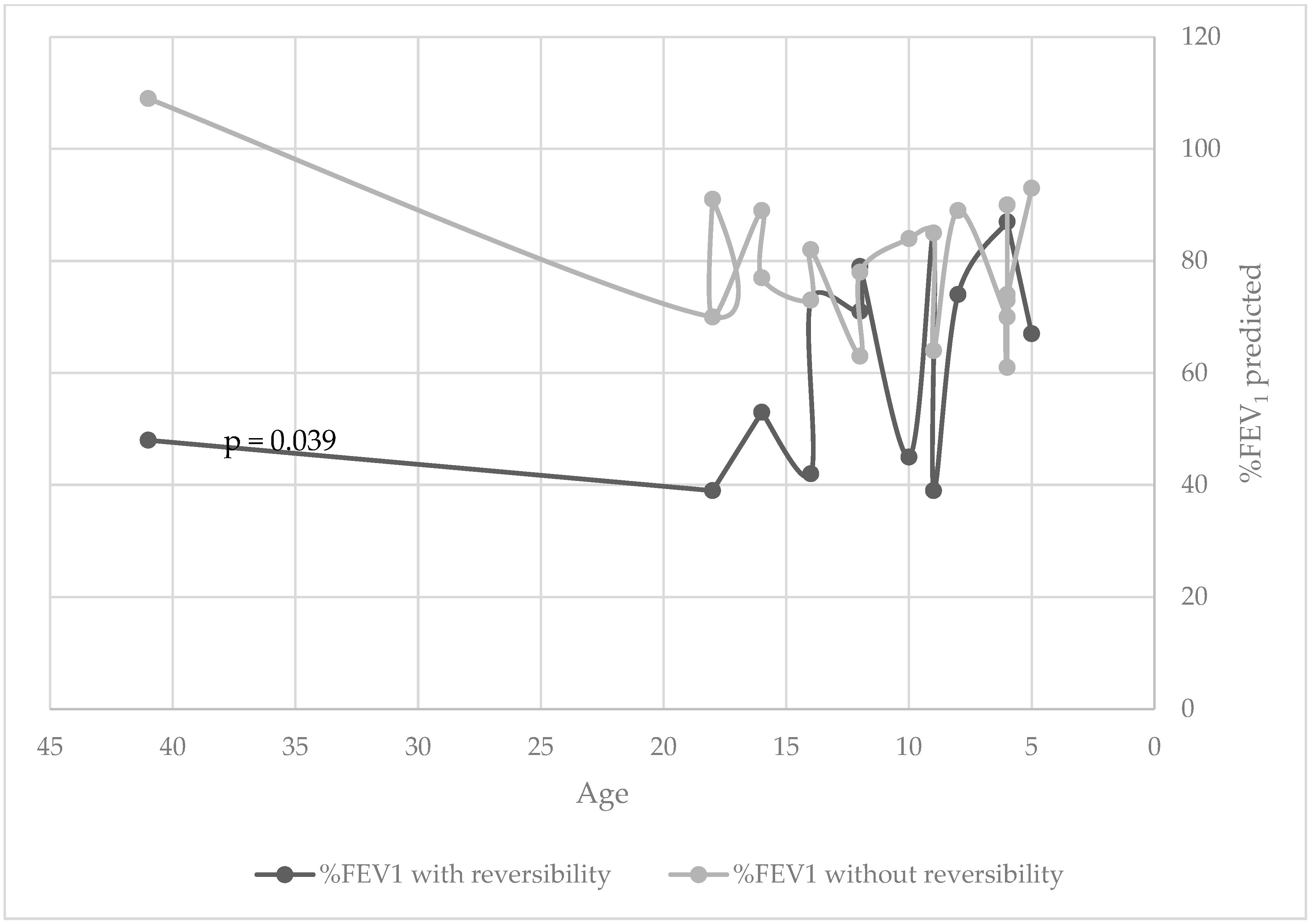
| %FEV1 predicted (median, range) | 72 (32–109) | 77 (61–109) | 60 (32–92) | 0.07 |
| Reversibility in %FEV1 (median, range) | 11.5 (0–27) | 5 (0–8) | 16 (10–27) | <0.001 |
| Age (years) (median, range) | 12 (5–48) | At best-recorded spirometry 11 (5–48) | At best reversibility 13.5 (5–41) | 0.301 |
| Asthma/Atopy: | ||||
| Familial asthma | 6 (13.0%) | 2 (10.0%) | 4 (15.4%) | 0.591 |
| Atopy/allergy | 4 (8.7%) | 2 (10.0%) | 2 (7.7%) | 0.783 |
| Eosinophils ≥ 5% | 28 (62.2%) | 14 (70.0%) | 14 (56.0%) | 0.336 |
| IgE ≥ 100 IU | 9 (20.0%) | 5 (25.0%) | 4 (16.0%) | 0.453 |
| Neonatal/Childhood characteristics: | ||||
| Neonatal tachypnea or pneumonia (n = 25/46, 54%) | 19 (76.0%) | 11 (91.7%) | 8 (61.5%) | 0.078 |
| Recurrent wheezing (n = 22/46, 48%) | 15 (68.2%) | 4 (40.0%) | 11 (91.7%) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levine, H.; Bar-On, O.; Nir, V.; West, N.; Dizitzer, Y.; Mussaffi, H.; Prais, D. Reversible Bronchial Obstruction in Primary Ciliary Dyskinesia. J. Clin. Med. 2022, 11, 6791. https://doi.org/10.3390/jcm11226791
Levine H, Bar-On O, Nir V, West N, Dizitzer Y, Mussaffi H, Prais D. Reversible Bronchial Obstruction in Primary Ciliary Dyskinesia. Journal of Clinical Medicine. 2022; 11(22):6791. https://doi.org/10.3390/jcm11226791
Chicago/Turabian StyleLevine, Hagit, Ophir Bar-On, Vered Nir, Nicole West, Yotam Dizitzer, Huda Mussaffi, and Dario Prais. 2022. "Reversible Bronchial Obstruction in Primary Ciliary Dyskinesia" Journal of Clinical Medicine 11, no. 22: 6791. https://doi.org/10.3390/jcm11226791