
Iris Racemose Hemangioma Assessment with Swept Source Optical Coherence Tomography Angiography: A Feasibility Study and Stand-Alone Comparison

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
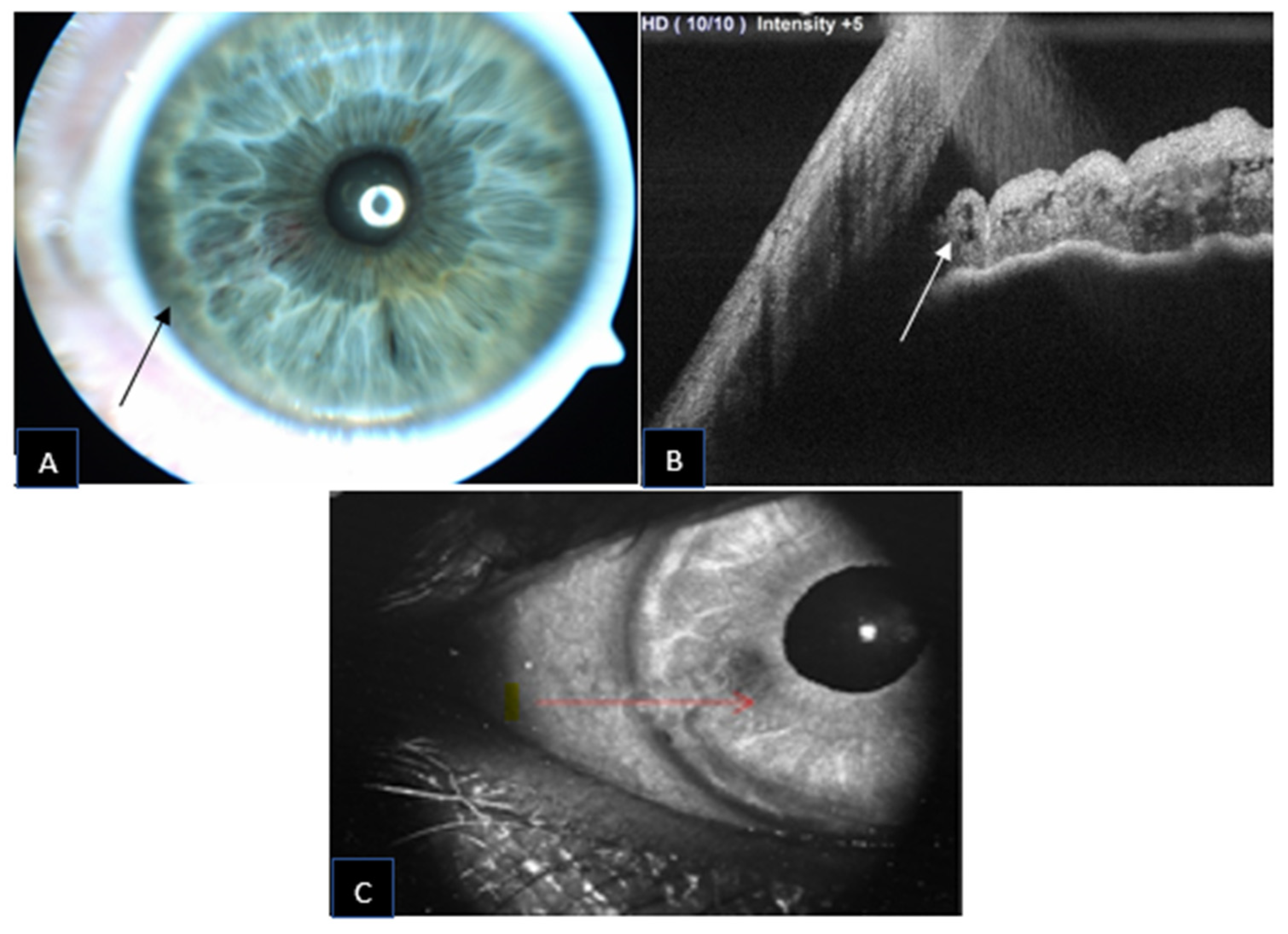
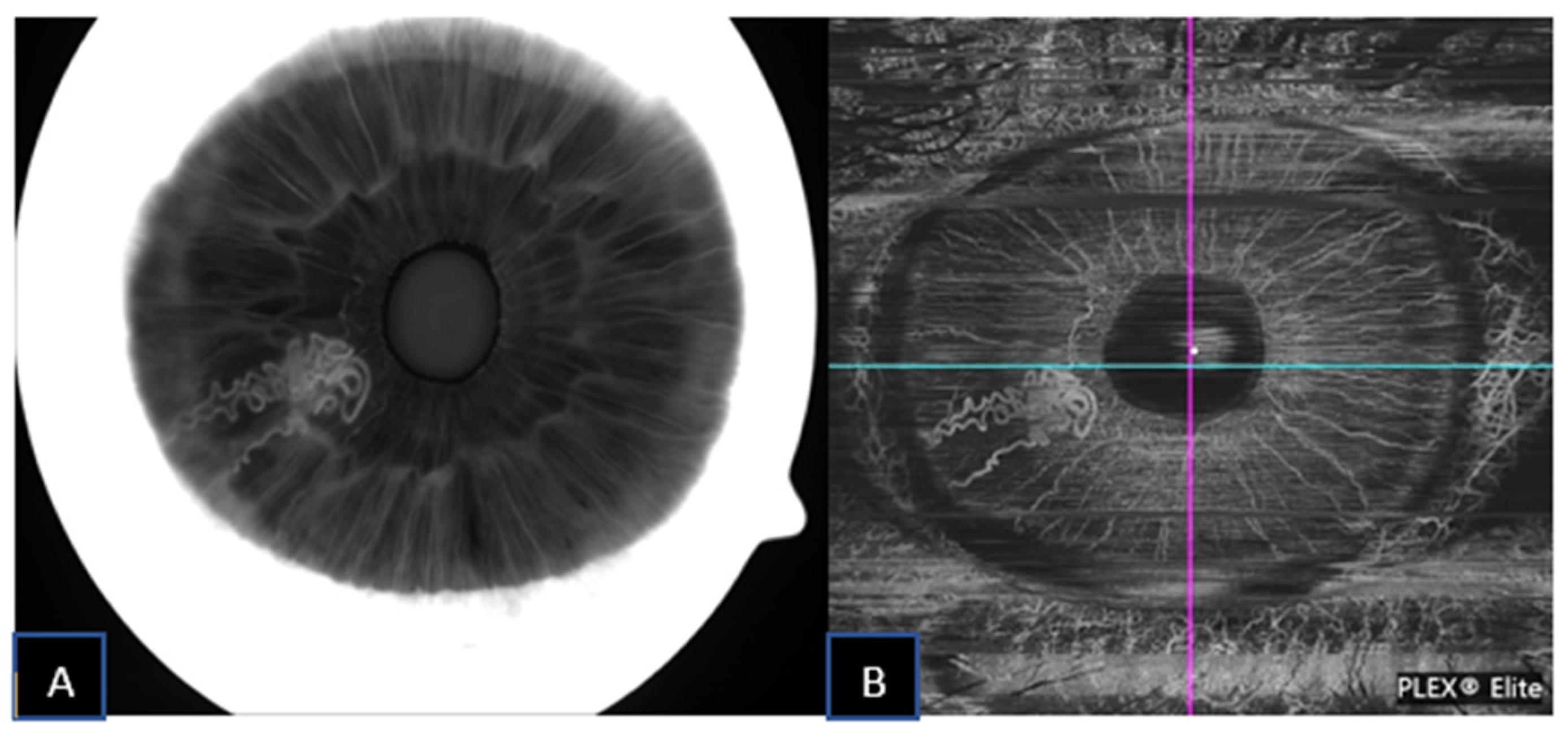
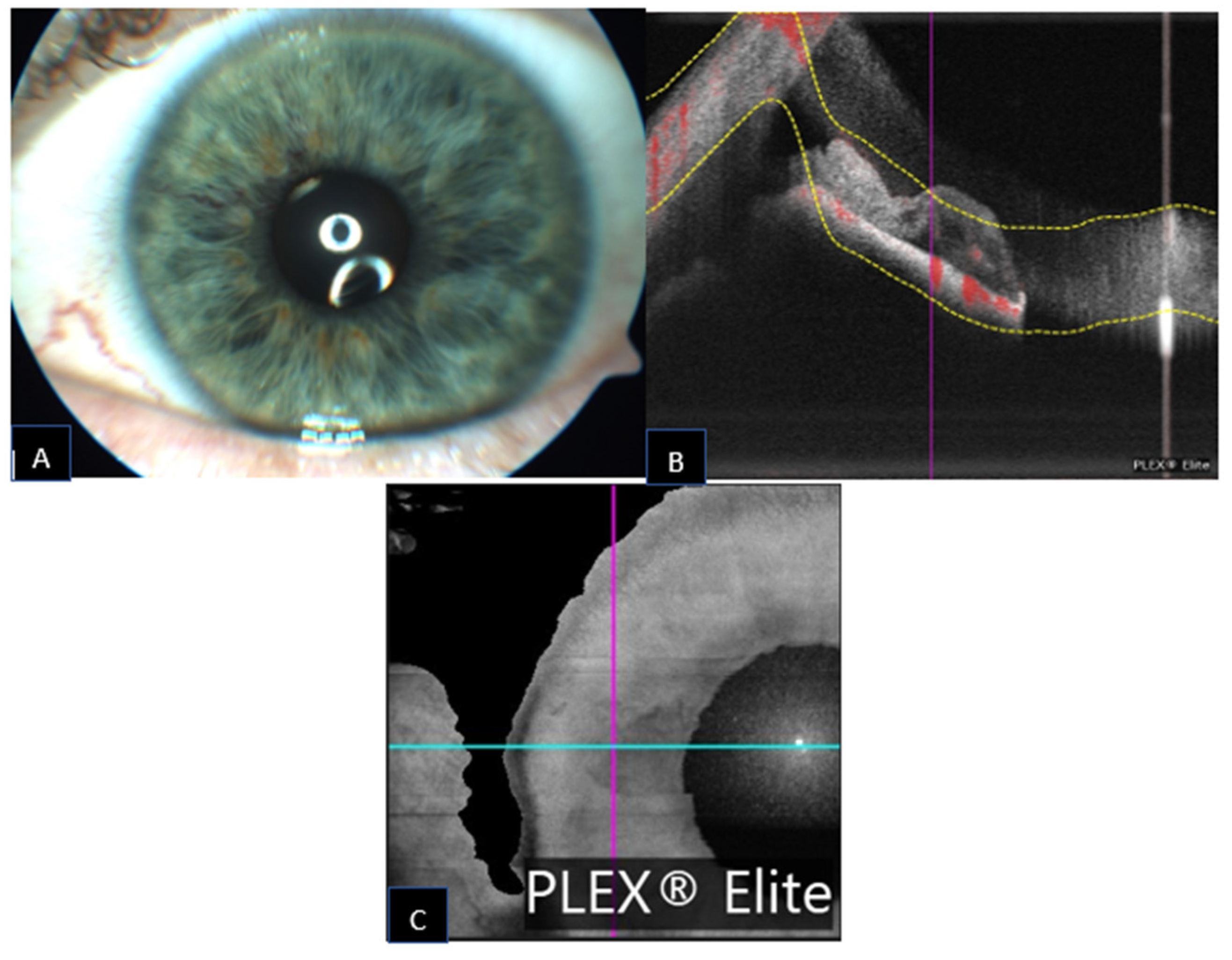
3.1. Patient 1
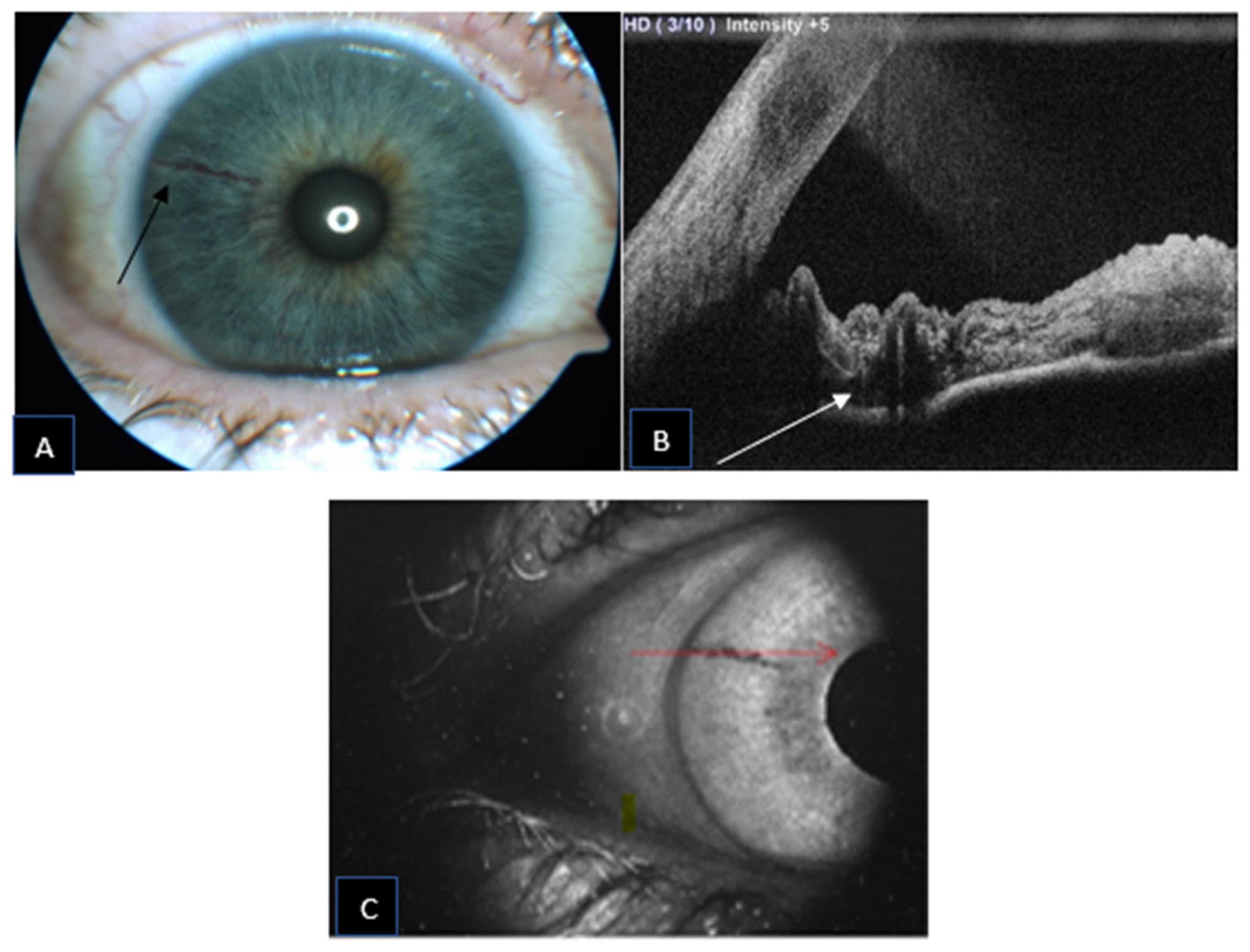
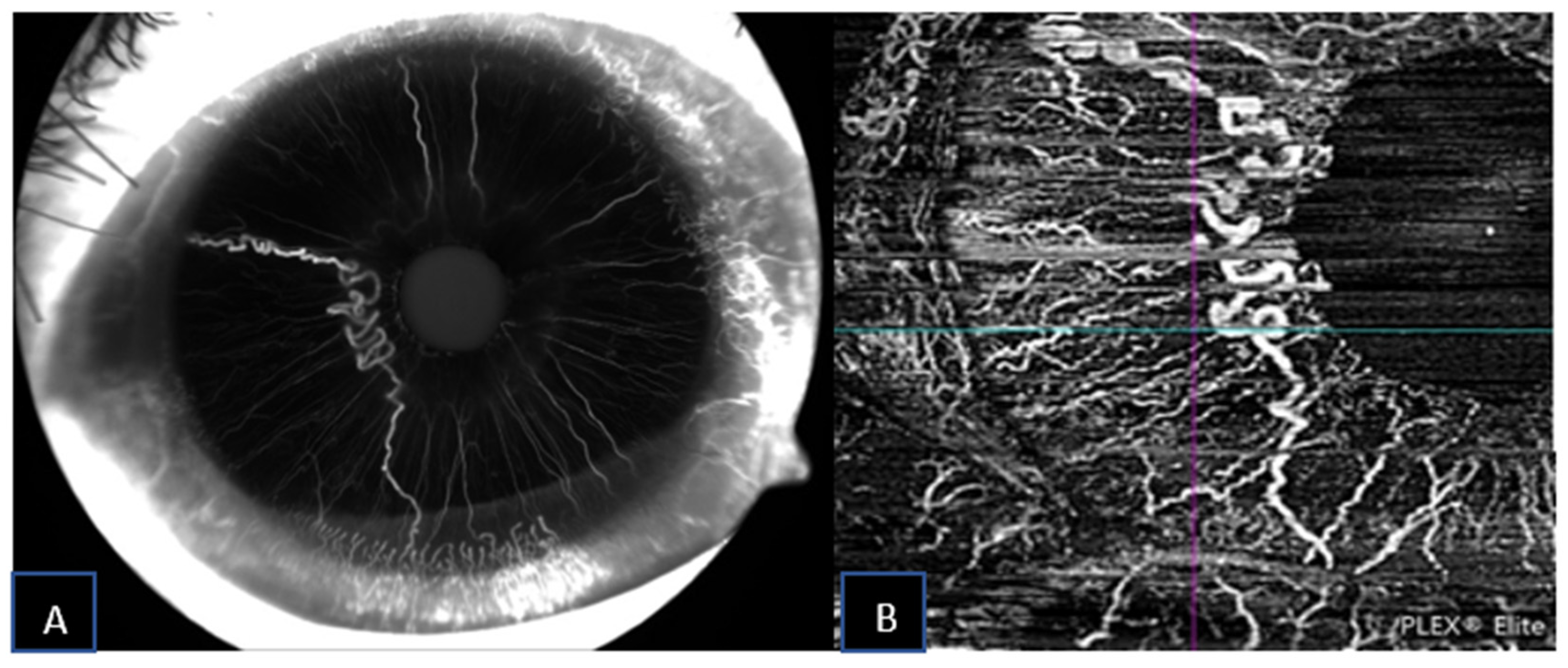
3.2. Patient 2
3.3. Patient 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prost, M. Arteriovenous Communication of the Iris. Br. J. Ophthalmol. 1986, 70, 856–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, J.A.; Streicher, T.F.E.; Spirkova, J.H.J.; Stubna, M.; Shields, C.L. Arteriovenous Malformation of the Iris in 14 Cases. Arch. Ophthalmol. 2006, 124, 370–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iris Arteriovenous Malformation—EyeWiki. Available online: https://eyewiki.aao.org/Iris_Arteriovenous_Malformation (accessed on 24 September 2022).
- Allegrini, D.; Montesano, G.; Pece, A. Optical Coherence Tomography Angiography in a Normal Iris. Ophthalmic Surg. Lasers Imaging Retin. 2016, 47, 1138–1139. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.L.; Sioufi, K.; Ferenczy, S.; Say, E.A.T.; Shields, C.L. Optical Coherence Tomography Angiography Features of Iris Racemose Hemangioma in 4 Cases. JAMA Ophthalmol. 2017, 135, 1106–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, P.J.; Durbin, M.K.; Roisman, L.; Zheng, F.; Miller, A.; Robbins, G.; Schaal, K.B.; Gregori, G. ZEISS AngioplexTM Spectral Domain Optical Coherence Tomography Angiography: Technical Aspects. Dev. Ophthalmol. 2016, 56, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Shiozaki, D.; Sakimoto, S.; Shiraki, A.; Wakabayashi, T.; Fukushima, Y.; Oie, Y.; Usui, S.; Sato, S.; Sakaguchi, H.; Nishida, K. Observation of Treated Iris Neovascularization by Swept-Source-Based En-Face Anterior-Segment Optical Coherence Tomography Angiography. Sci. Rep. 2019, 9, 10262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, M.; Cai, Y.; Tan, A.C.S. Swept Source Optical Coherence Tomography Angiography for Contact Lens-Related Corneal Vascularization. J. Ophthalmol. 2016, 2016, e9685297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skalet, A.H.; Li, Y.; Lu, C.D.; Jia, Y.; Lee, B.; Husvogt, L.; Maier, A.; Fujimoto, J.G.; Thomas, C.R.; Huang, D. Optical Coherence Tomography Angiography Characteristics of Iris Melanocytic Tumors. Ophthalmology 2017, 124, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, A.S.; Welch, R.J.; Sioufi, K.; Say, E.A.T.; Shields, J.A.; Shields, C.L. Optical Coherence Tomography Angiography of Iris Microhemangiomatosis. Am. J. Ophthalmol. Case Rep. 2017, 6, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.L.; Sioufi, K.; Shields, C.L. Optical Coherence Tomography Angiography of Conjunctival Racemose Hemangioma. Ophthalmology 2017, 124, 449. [Google Scholar] [CrossRef] [PubMed]
- Zett, C.; Stina, D.M.R.; Kato, R.T.; Novais, E.A.; Allemann, N. Comparison of Anterior Segment Optical Coherence Tomography Angiography and Fluorescein Angiography for Iris Vasculature Analysis. Graefe Arch. Clin. Exp. Ophthalmol. 2018, 256, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ang, M.; Devarajan, K.; Tan, A.C.; Ke, M.; Tan, B.; Teo, K.; Sng, C.C.A.; Ting, D.S.; Schmetterer, L. Anterior Segment Optical Coherence Tomography Angiography for Iris Vasculature in Pigmented Eyes. Br. J. Ophthalmol. 2021, 105, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Fujimoto, M.; Ikeda, H.O. Anterior Segment Optical Coherence Tomography Angiography of Iris Neovascularization After Intravitreal Ranibizumab and Panretinal Photocoagulation. JAMA Ophthalmol. 2020, 138, e190318. [Google Scholar] [CrossRef] [PubMed]
- Roberts, P.K.; Goldstein, D.A.; Fawzi, A.A. Anterior Segment Optical Coherence Tomography Angiography for Identification of Iris Vasculature and Staging of Iris Neovascularization: A Pilot Study. Curr. Eye Res. 2017, 42, 1136–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, J.A.; Bianciotto, C.; Kligman, B.E.; Shields, C.L. Vascular Tumors of the Iris in 45 Patients: The 2009 Helen Keller Lecture. Arch. Ophthalmol. 2010, 128, 1107–1113. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Age | 59 | 69 | 60 |
| Ethnicity | Caucasian | Caucasian | Caucasian |
| Sex | Male | Female | Male |
| Referral diagnosis | Pigmented iris lesion | Pigmented iris lesion | Pigmented iris lesion |
| Involved eye | Right eye | Right eye | Left eye |
| BCVA | 20/20 | 20/32 | 20/20 |
| Iris color | Blue | Blue | Blue |
| Clock hour | 7–8 | 6–10 | 10–12 |
| Concomitant iris or ciliary body mass | no | no | no |
| Visibility UBM | Indistinct | Indistinct | Indistinct |
| Visibility at the slit lamp | Red lesion | Red indistinct lesion | Red indistinct lesion |
| Visibility at AS-OCT | Cystic lesions | Cystic lesions | Cystic lesions |
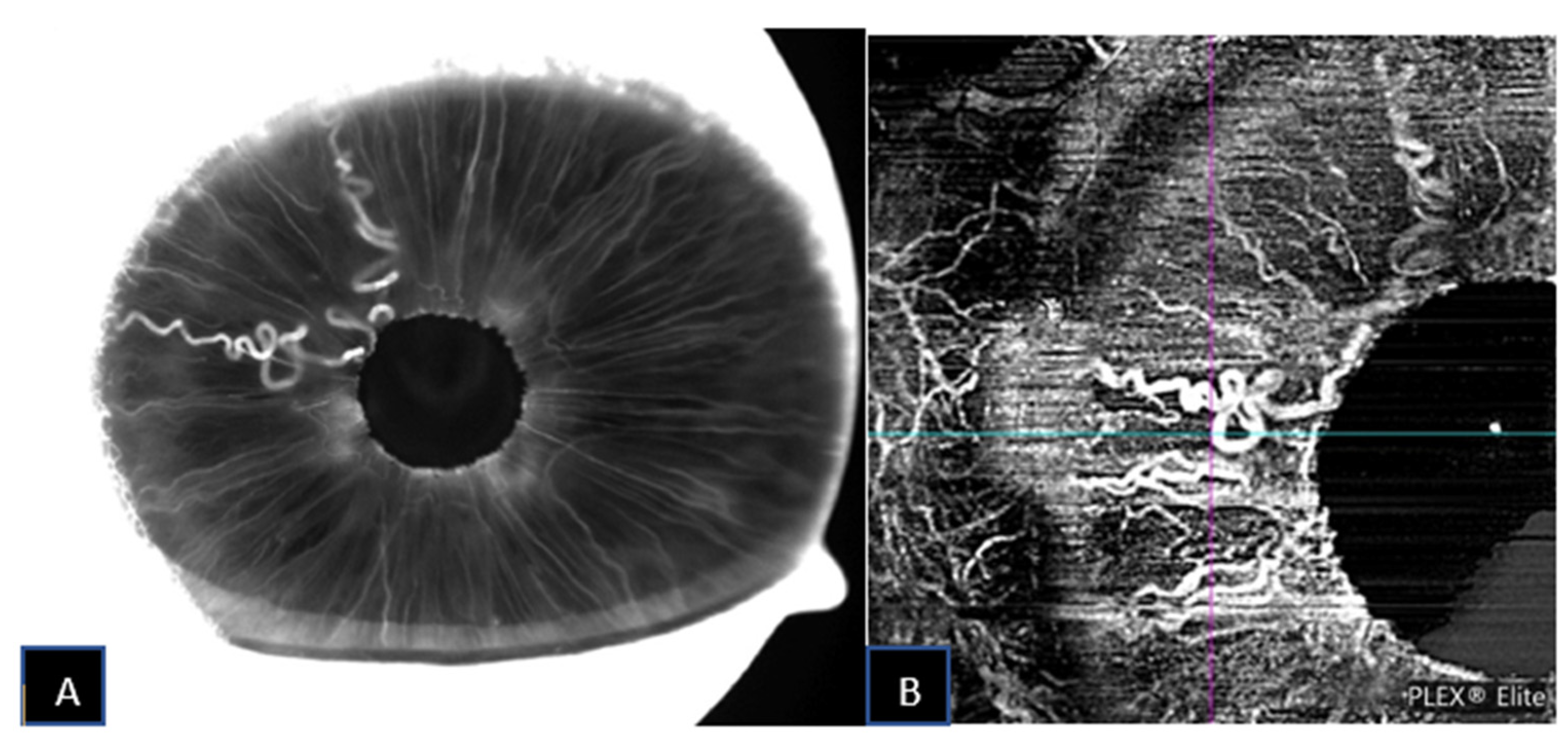
| Visibility at SS-OCTA | Well defined vascular network | Well defined vascular network | Well defined vascular network |
| Visibility at IVFA | Well defined vascular network without leakage | Well defined vascular network without leakage | Well defined vascular network without leakage |
| Vascular course | Convoluted | Convoluted at the pupil margin | Convoluted at the pupil margin |
| Hemangioma type characterization | Complex | Complex | Complex |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Confalonieri, F.; Ngo, H.B.; Petersen, H.H.; Eide, N.A.; Petrovski, G. Iris Racemose Hemangioma Assessment with Swept Source Optical Coherence Tomography Angiography: A Feasibility Study and Stand-Alone Comparison. J. Clin. Med. 2022, 11, 6575. https://doi.org/10.3390/jcm11216575
Confalonieri F, Ngo HB, Petersen HH, Eide NA, Petrovski G. Iris Racemose Hemangioma Assessment with Swept Source Optical Coherence Tomography Angiography: A Feasibility Study and Stand-Alone Comparison. Journal of Clinical Medicine. 2022; 11(21):6575. https://doi.org/10.3390/jcm11216575
Chicago/Turabian StyleConfalonieri, Filippo, Huy Bao Ngo, Helga Halldorsdottir Petersen, Nils Andreas Eide, and Goran Petrovski. 2022. "Iris Racemose Hemangioma Assessment with Swept Source Optical Coherence Tomography Angiography: A Feasibility Study and Stand-Alone Comparison" Journal of Clinical Medicine 11, no. 21: 6575. https://doi.org/10.3390/jcm11216575