
Increased Surgical Experience in Microendoscopic Spinal Surgery Can Reduce Development of Postoperative Spinal Epidural Hematoma and Improve the Clinical Outcomes
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Surgical Criteria
2.3. Perioperative Clinical Care
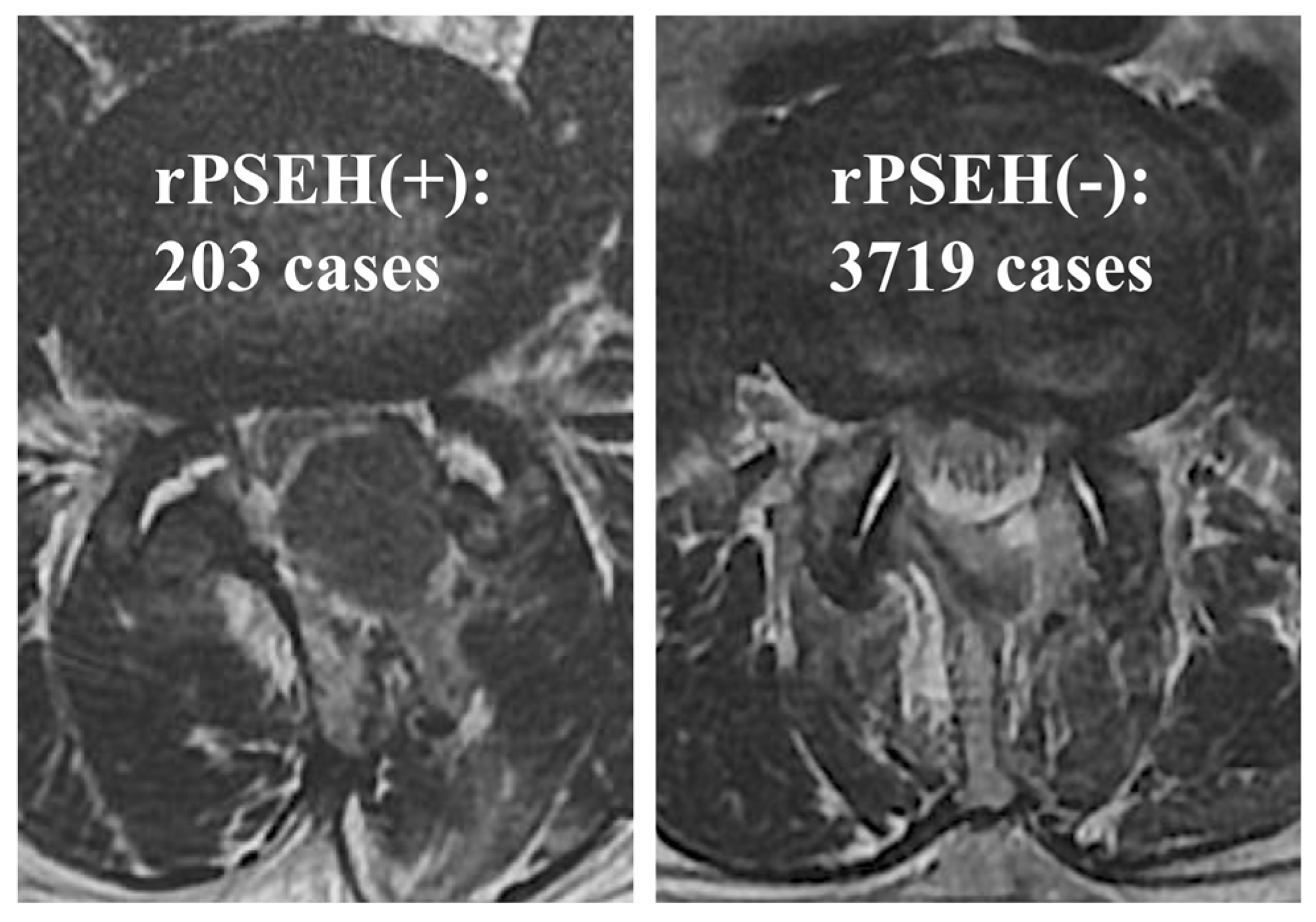
2.4. Definition of rPSEH
2.5. Preoperative Data
2.6. Surgical Data
2.7. Clinical Score
2.8. Statistical Analyses
3. Results
3.1. Incidence Rate of rPSEH
3.2. Risk Factors of rPSEH
3.3. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schroeder, G.D.; Kurd, M.F.; Kepler, C.K.; Arnold, P.M.; Vaccaro, A.R. Postoperative Epidural Hematomas in the Lumbar Spine. J. Spinal Disord. Tech. 2015, 28, 313–318. [Google Scholar] [CrossRef]
- Fujita, N.; Michikawa, T.; Yagi, M.; Suzuki, S.; Tsuji, O.; Nagoshi, N.; Okada, E.; Tsuji, T.; Nakamura, M.; Matsumoto, M.; et al. Impact of lumbar hypolordosis on the incidence of symptomatic postoperative spinal epidural hematoma after decompression surgery for lumbar spinal canal stenosis. Eur. Spine J. 2018, 28, 87–93. [Google Scholar] [CrossRef]
- Ikuta, K.; Tono, O.; Tanaka, T.; Arima, J.; Nakano, S.; Sasaki, K.; Oga, M. Evaluation of postoperative spinal epidural hematoma after microendoscopic posterior decompression for lumbar spinal stenosis: A clinical and magnetic resonance imaging study. J. Neurosurg. Spine 2006, 5, 404–409. [Google Scholar] [CrossRef]
- Sokolowski, M.J.; Garvey, T.A.; Perl, J., II; Sokolowski, M.S.; Akesen, B.; Mehbod, A.A.; Mullaney, K.J.; Dykes, D.C.; Transfeldt, E.E. Postoperative lumbar epidural hematoma: Does size really matter? Spine 2008, 33, 114–119. [Google Scholar] [CrossRef]
- Kao, F.-C.; Tsai, T.-T.; Chen, L.-H.; Lai, P.-L.; Fu, T.-S.; Niu, C.-C.; Ho, N.Y.-J.; Chen, W.-J.; Chang, C.-J. Symptomatic epidural hematoma after lumbar decompression surgery. Eur. Spine J. 2014, 24, 348–357. [Google Scholar] [CrossRef]
- Yamada, K.; Abe, Y.; Satoh, S.; Yanagibashi, Y.; Hyakumachi, T.; Masuda, T. Large increase in blood pressure after extubation and high body mass index elevate the risk of spinal epidural hematoma after spinal surgery. Spine 2015, 40, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Manabe, H.; Izumi, B.; Harada, T.; Nakanishi, K.; Tanaka, N.; Adachi, N. The impact of hypertension on the occurrence of postoperative spinal epidural hematoma following single level microscopic posterior lumbar decompression surgery in a single institute. Eur. Spine J. 2017, 26, 2606–2615. [Google Scholar] [CrossRef] [PubMed]
- Foley, K.T.; Smith, M.M. Microendoscopic discectomy. Tech. Neurosurg. 1997, 3, 301–307. [Google Scholar]
- Ikuta, K.; Arima, J.; Tanaka, T.; Oga, M.; Nakano, S.; Sasaki, K.; Goshi, K.; Yo, M.; Fukagawa, S. Short-term results of microendoscopic posterior decompression for lumbar spinal stenosis. J. Neurosurg. Spine 2005, 2, 624–633. [Google Scholar] [CrossRef] [Green Version]
- Minamide, A.; Yoshida, M.; Yamada, H.; Nakagawa, Y.; Kawai, M.; Maio, K.; Hashizume, H.; Iwasaki, H.; Tsutsui, S. Endoscope-assisted spinal decompression surgery for lumbar spinal stenosis. J. Neurosurg. Spine 2013, 19, 664–671. [Google Scholar] [CrossRef] [Green Version]
- Pao, J.L.; Chen, W.C.; Chen, P.Q. Clinical outcomes of microendoscopic decompressive laminotomy for degenerative lumbar spinal stenosis. Eur. Spine J. 2009, 18, 672–678. [Google Scholar] [CrossRef]
- Minamide, A.; Yoshida, M.; Yamada, H.; Nakagawa, Y.; Hashizume, H.; Iwasaki, H.; Tsutsui, S. Clinical outcomes after microendoscopic laminotomy for lumbar spinal stenosis: A 5-year follow-up study. Eur. Spine J. 2014, 24, 396–403. [Google Scholar] [CrossRef]
- Nomura, K.; Yoshida, M. Assessment of the Learning Curve for Microendoscopic Decompression Surgery for Lumbar Spinal Canal Stenosis through an Analysis of 480 Cases Involving a Single Surgeon. Glob. Spine J. 2017, 7, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marappan, K.; Jothi, R.; Paul Raj, S. Microendoscopic discectomy (MED) for lumbar disc herniation: Comparison of learning curve of the surgery and outcome with other established case studies. J. Spine Surg. 2018, 4, 630–637. [Google Scholar] [CrossRef]
- Minamide, A.; Yoshida, M.; Simpson, A.K.; Nakagawa, Y.; Iwasaki, H.; Tsutsui, S.; Takami, M.; Hashizume, H.; Yukawa, Y.; Yamada, H. Minimally invasive spinal decompression for degenerative lumbar spondylolisthesis and stenosis maintains stability and may avoid the need for fusion. Bone Jt. J. 2018, 100, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Kobayashi, N.; Saiki, K.; Kitagawa, T.; Tamai, K.; Saotome, K. Association of the Japanese Orthopaedic Association score with the Oswestry Disability Index, Roland-Morris Disability Questionnaire, and Short-Form 36. Spine 2003, 28, 1601–1607. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Couper, J.; Davies, J.B.; O’Brien, J.P. The Oswestry low back pain disability questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, E.P.; Lampley, A.J.; Chen, A.; Adams, S.B.; Nettles, D.L.; Richard, M.J. Inflammatory cytokines and matrix metalloproteinases in the synovial fluid after intra-articular elbow fracture. J. Shoulder Elb. Surg. 2020, 29, 736–742. [Google Scholar] [CrossRef]
- Masaki, M.; Aoyama, T.; Murakami, T.; Yanase, K.; Ji, X.; Tateuchi, H.; Ichihashi, N. Association of low back pain with muscle stiffness and muscle mass of the lumbar back muscles, and sagittal spinal alignment in young and middle-aged medical workers. Clin. Biomech. 2017, 49, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Ko, S.; Chae, S. Correlations Between the SF-36, the Oswestry-Disability Index and Rolland-Morris Disbility Questionnaire in Patients Undergoing Lumbar Decompression According to Types of Spine Origin Pain. Clin. Spine Surg. 2017, 30, E804–E808. [Google Scholar] [CrossRef] [PubMed]
- Awad, J.N.; Kebaish, K.M.; Donigan, J.; Cohen, D.B.; Kostuik, J.P. Analysis of the risk factors for the development of post-operative spinal epidural haematoma. J. Bone Jt. Surg. Br. Vol. 2005, 87, 1248–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kou, J.; Fischgrund, J.; Biddinger, A.; Herkowitz, H. Risk factors for spinal epidural hematoma after spinal surgery. Spine 2002, 27, 1670–1673. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, S.; Takahashi, S.; Tamai, K.; Hori, Y.; Hirakawa, Y.; Hoshino, M.; Suzuki, A.; Nakamura, H. Prevention of Nerve Root Thermal Injury Caused by Bipolar Cauterization Near the Nerve Roots. Spine 2019, 44, E321–E328. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| rPSEH Group (n = 203) | Control Group (n = 3719) | p-Value | |||
|---|---|---|---|---|---|
| Accumulated surgical experiences (cases) | 1–1000 | 70 (7.0%) | 930 | 0.017 | |
| 1001–2000 | 49 (4.9%) | 951 | |||
| 2001–3000 | 48 (4.8%) | 952 | |||
| 3001–3922 | 36 (3.9%) | 886 | |||
| Initial 1000 cases | Learning period | 1–25 | 7 (28.0%) | 18 | <0.001 |
| Proficient period | 26–100 | 3 (4.0%) | 72 | ||
| Expert period | 101–1000 | 60 (6.7%) | 840 | ||
| rPSEH Group (n = 203) | Control Group (n = 3719) | p-Value | ||
|---|---|---|---|---|
| Age (years old) | 64.9 ± 14.7 | 54.8 ± 18.0 | <0.001 | |
| Sex | Male | 138 | 2369 | 0.245 |
| Female | 65 | 1350 | ||
| BMI (kg/m2) | 25.1 ± 3.7 | 23.9 ± 3.7 | <0.001 | |
| Pre-op JOA score | 14.3 ± 4.9 | 13.5 ± 5.3 | 0.044 | |
| Pre-op ODI | 41.8 ± 16.3 | 44.2 ± 19.5 | 0.118 | |
| The number of pre-op epidural injection | 1.2 ± 1.8 | 1.0 ± 1.9 | 0.343 | |
| Pre-op motor weakness | MMT = 5 | 187 | 3228 | 0.018 |
| MMT ≤ 4 | 14 | 479 | ||
| Pre-op bowel bladder disfunction | (−) | 201 | 3685 | 0.541 |
| (+) | 0 | 22 |
| rPSEH Group (n = 203) | Control Group (n = 3719) | p-Value | ||
|---|---|---|---|---|
| Diagnosis | LSS | 159 | 1731 | <0.001 |
| LDH | 44 | 1988 | ||
| The number of surgical segments | 1 level | 129 | 3122 | <0.001 |
| 2 levels | 61 | 518 | ||
| 3 levels | 13 | 78 | ||
| 4 levels | 0 | 1 | ||
| Surgical time per segment (min) | 82.3 ± 27.0 | 69.4 ± 26.1 | <0.001 | |
| Intraoperative dural puncture (cases) | (−) | 195 | 3639 | 0.251 |
| (+) | 8 | 75 | ||
| In-hospital period (days) | 7.4 ± 3.4 | 6.4 ± 2.2 | <0.001 | |
| Additional painkiller use (times) | 1.2 ± 1.2 | 1.1 ± 0.9 | 0.023 |
| Explanation Variables | Reference | aOR | p-Value | 95%CI | |
|---|---|---|---|---|---|
| Age | (55 years) | ≤54 | 1.87 | 0.002 | 1.25–2.81 |
| BMI | (≥25 kg/m2) | <25 | 1.33 | 0.056 | 0.99–1.79 |
| Surgical experiences | (1–1000 cases) | ≥1001 | 1.62 | 0.003 | 1.19–2.22 |
| Diagnosis | (LSS) | LDH | 1.93 | 0.004 | 1.24–3.01 |
| Surgical time per segment | (≥70 min) | <70 | 1.44 | 0.038 | 1.02–2.04 |
| Surgical segments | (multilevel) | One level | 1.74 | <0.001 | 1.25–2.41 |
| Pre-op JOA score | (≥14 points) | <14 | 1.07 | 0.649 | 0.80–1.44 |
| Pre-op motor weakness | (−) | (+) | 1.35 | 0.301 | 0.76–2.39 |
| Clinical Scores | rPSEH Group (n = 203) | Control Group (n = 3719) | p-Value |
|---|---|---|---|
| JOA score | 0.037 | ||
| Preoperative | 14.3 ± 4.9 | 13.5 ± 5.3 | |
| Postoperative | 26.4 ± 2.4 | 26.6 ± 2.5 | |
| ODI | 0.014 | ||
| Preoperative | 41.8 ± 16.3 | 44.2 ± 19.5 | |
| Postoperative | 9.5 ± 12.0 | 7.2 ± 9.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwamae, M.; Tamai, K.; Kaneda, K.; Terai, H.; Katsuda, H.; Shimada, N.; Nakamura, H. Increased Surgical Experience in Microendoscopic Spinal Surgery Can Reduce Development of Postoperative Spinal Epidural Hematoma and Improve the Clinical Outcomes. J. Clin. Med. 2022, 11, 6495. https://doi.org/10.3390/jcm11216495
Iwamae M, Tamai K, Kaneda K, Terai H, Katsuda H, Shimada N, Nakamura H. Increased Surgical Experience in Microendoscopic Spinal Surgery Can Reduce Development of Postoperative Spinal Epidural Hematoma and Improve the Clinical Outcomes. Journal of Clinical Medicine. 2022; 11(21):6495. https://doi.org/10.3390/jcm11216495
Chicago/Turabian StyleIwamae, Masayoshi, Koji Tamai, Kunikazu Kaneda, Hidetomi Terai, Hiroshi Katsuda, Nagakazu Shimada, and Hiroaki Nakamura. 2022. "Increased Surgical Experience in Microendoscopic Spinal Surgery Can Reduce Development of Postoperative Spinal Epidural Hematoma and Improve the Clinical Outcomes" Journal of Clinical Medicine 11, no. 21: 6495. https://doi.org/10.3390/jcm11216495