
Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care
 ,
,
Abstract
:1. Introduction
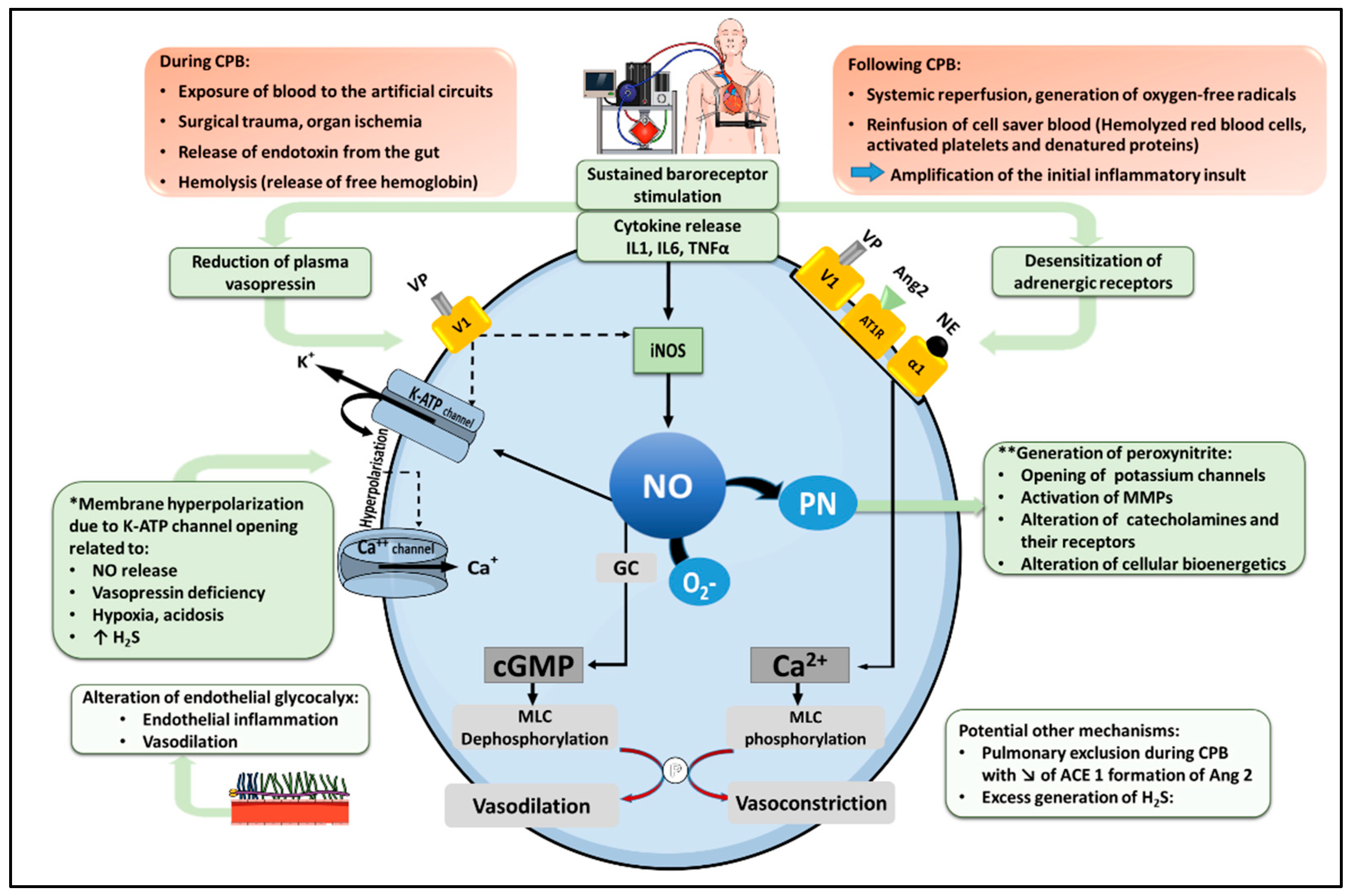
2. Pathophysiology of Vasoplegic Syndrome after CPB (Figure 1)
2.1. Physiology of Vascular Smooth Muscle Cell Contraction
2.2. Inflammatory Pathways Triggered by CPB
2.3. Adrenoreceptor Desensitization
2.4. Increased Nitric Oxide Biosynthesis
2.5. Relative Deficiency of Vasopressin
2.6. Activation of KATP Channels and Membrane Hyperpolarization in VSMCs
2.7. Dysfunction of the Renin-Angiotensin System
2.8. Endothelial Glycocalyx Alteration
2.9. Possible Role of an Excess Production of Hydrogen Sulfide
3. Predisposing Factors of Post-CPB Vasoplegic Syndrome
3.1. Patient-Related Factors
3.2. Pre- and Peri-Operative Drug Therapies
4. Outcome
5. Management
5.1. Peri-Operative Prevention
5.2. Volume Resuscitation
5.3. Vasoactive Drugs
5.3.1. Norepinephrine
5.3.2. Vasopressin
5.3.3. Angiotensin 2
5.3.4. Methylene Blue
5.3.5. Hydroxocobalamin
5.3.6. Vitamin C
5.4. Anti-Inflammatory Strategies
5.4.1. Corticosteroids
5.4.2. Extracorporeal Cytokine Adsorption Therapy
5.5. Management of VS after CPB: Summary of Evidence and Current Recommendations (Table 1)
6. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kristof, A.S.; Magder, S. Low systemic vascular resistance state in patients undergoing cardiopulmonary bypass. Crit. Care Med. 1999, 27, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Leyh, R.G.; Kofidis, T.; Strüber, M.; Fischer, S.; Knobloch, K.; Wachsmann, B.; Hagl, C.; Simon, A.R.; Haverich, A. Methylene blue: The drug of choice for catecholamine-refractory vasoplegia after cardiopulmonary bypass? J. Thorac. Cardiovasc. Surg. 2003, 125, 1426–1431. [Google Scholar] [CrossRef] [Green Version]
- Nash, C.M. Vasoplegic Syndrome in Patients Undergoing Cardiac Surgery: A Literature Review. AACN Adv. Crit. Care 2021, 32, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.; Zedan, A.; Nugent, K. Cardiac vasoplegia syndrome: Pathophysiology, risk factors and treatment. Am. J. Med. Sci. 2015, 349, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petermichl, W.; Gruber, M.; Schoeller, I.; Allouch, K.; Graf, B.M.; Zausig, Y.A. The additional use of methylene blue has a decatecholaminisation effect on cardiac vasoplegic syndrome after cardiac surgery. J. Cardiothorac. Surg. 2021, 16, 205. [Google Scholar] [CrossRef]
- Wan, S.; LeClerc, J.L.; Vincent, J.L. Inflammatory response to cardiopulmonary bypass: Mechanisms involved and possible therapeutic strategies. Chest 1997, 112, 676–692. [Google Scholar] [CrossRef]
- Gomes, W.J.; Carvalho, A.C.; Palma, J.H.; Gonçalves, I., Jr.; Buffolo, E. Vasoplegic syndrome: A new dilemma. J. Thorac. Cardiovasc. Surg. 1994, 107, 942–943. [Google Scholar] [CrossRef] [Green Version]
- Cremer, J.; Martin, M.; Redl, H.; Bahrami, S.; Abraham, C.; Graeter, T.; Haverich, A.; Schlag, G.; Borst, H.G. Systemic inflammatory response syndrome after cardiac operations. Ann. Thorac. Surg. 1996, 61, 1714–1720. [Google Scholar] [CrossRef]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.-L. Comparison of Dopamine and Norepinephrine in the Treatment of Shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Argenziano, M.; Chen, J.M.; Choudhri, A.F.; Cullinane, S.; Garfein, E.; Weinberg, A.D.; Smith, C.R., Jr.; Rose, E.A.; Landry, D.W.; Oz, M.C. Management of vasodilatory shock after cardiac surgery: Identification of predisposing factors and use of a novel pressor agent. J. Thorac. Cardiovasc. Surg. 1998, 116, 973–980. [Google Scholar] [CrossRef]
- Argenziano, M.; Choudhri, A.F.; Oz, M.C.; Rose, E.A.; Smith, C.R.; Landry, D.W. A prospective randomized trial of arginine vasopressin in the treatment of vasodilatory shock after left ventricular assist device placement. Circulation 1997, 96, II-286–II-290. [Google Scholar] [PubMed]
- Levin, M.A.; Lin, H.M.; Castillo, J.G.; Adams, D.H.; Reich, D.L.; Fischer, G.W. Early on-cardiopulmonary bypass hypotension and other factors associated with vasoplegic syndrome. Circulation 2009, 120, 1664–1671. [Google Scholar] [CrossRef] [Green Version]
- Hajjar, L.A.; Vincent, J.L.; Barbosa Gomes Galas, F.R.; Rhodes, A.; Landoni, G.; Osawa, E.A.; Melo, R.R.; Sundin, M.R.; Grande, S.M.; Gaiotto, F.A.; et al. Vasopressin versus Norepinephrine in Patients with Vasoplegic Shock after Cardiac Surgery: The VANCS Randomized Controlled Trial. Anesthesiology 2017, 126, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.S.; Hjortdal, V.E.; Andreasen, J.J.; Mortensen, P.E.; Jakobsen, C.J. 30-day mortality after coronary artery bypass grafting and valve surgery has greatly improved over the last decade, but the 1-year mortality remains constant. Ann. Card. Anaesth. 2015, 18, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Mazzeffi, M.; Zivot, J.; Buchman, T.; Halkos, M. In-hospital mortality after cardiac surgery: Patient characteristics, timing, and association with postoperative length of intensive care unit and hospital stay. Ann. Thorac. Surg. 2014, 97, 1220–1225. [Google Scholar] [CrossRef]
- Touyz, R.M.; Alves-Lopes, R.; Rios, F.J.; Camargo, L.L.; Anagnostopoulou, A.; Arner, A.; Montezano, A.C. Vascular smooth muscle contraction in hypertension. Cardiovasc. Res. 2018, 114, 529–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landry, D.W.; Oliver, J.A. The pathogenesis of vasodilatory shock. N. Engl. J. Med. 2001, 345, 588–595. [Google Scholar] [CrossRef]
- Surks, H.K.; Mochizuki, N.; Kasai, Y.; Georgescu, S.P.; Tang, K.M.; Ito, M.; Lincoln, T.M.; Mendelsohn, M.E. Regulation of myosin phosphatase by a specific interaction with cGMP- dependent protein kinase Ialpha. Science 1999, 286, 1583–1587. [Google Scholar] [CrossRef]
- Hall, R.I.; Smith, M.S.; Rocker, G. The systemic inflammatory response to cardiopulmonary bypass: Pathophysiological, therapeutic, and pharmacological considerations. Anesth. Analg. 1997, 85, 766–782. [Google Scholar] [CrossRef]
- Wan, S.; DeSmet, J.M.; Vincent, J.L.; LeClerc, J.L. Thrombus formation on a calcific and severely stenotic bicuspid aortic valve. Ann. Thorac. Surg. 1997, 64, 535–536. [Google Scholar] [CrossRef]
- McDaniel, N.L.; Rembold, C.M.; Richard, H.M.; Murphy, R.A. Cyclic AMP relaxes swine arterial smooth muscle predominantly by decreasing cell Ca2+ concentration. J. Physiol. 1991, 439, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Ohkawa, F.; Ikeda, U.; Kanbe, T.; Kawasaki, K.; Shimada, K. Effects of inflammatory cytokines on vascular tone. Cardiovasc. Res. 1995, 30, 711–715. [Google Scholar] [CrossRef]
- Weis, F.; Kilger, E.; Beiras-Fernandez, A.; Nassau, K.; Reuter, D.; Goetz, A.; Lamm, P.; Reindl, L.; Briegel, J. Association between vasopressor dependence and early outcome in patients after cardiac surgery. Anaesthesia 2006, 61, 938–942. [Google Scholar] [CrossRef]
- Kilger, E.; Weis, F.; Briegel, J.; Frey, L.; Goetz, A.E.; Reuter, D.; Nagy, A.; Schuetz, A.; Lamm, P.; Knoll, A.; et al. Stress doses of hydrocortisone reduce severe systemic inflammatory response syndrome and improve early outcome in a risk group of patients after cardiac surgery. Crit. Care Med. 2003, 31, 1068–1074. [Google Scholar] [CrossRef]
- Dayan, V.; Cal, R.; Giangrossi, F. Risk factors for vasoplegia after cardiac surgery: A meta-analysis. Interact Cardiovasc. Thorac. Surg. 2019, 28, 838–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic syndrome following cardiothoracic surgery-review of pathophysiology and update of treatment options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandasamy, K.; Prawez, S.; Choudhury, S.; More, A.S.; Ahanger, A.A.; Singh, T.U.; Parida, S.; Mishra, S.K. Atorvastatin prevents vascular hyporeactivity to norepinephrine in sepsis: Role of nitric oxide and α₁-adrenoceptor mRNA expression. Shock 2011, 36, 76–82. [Google Scholar] [CrossRef]
- Levy, B.; Fritz, C.; Tahon, E.; Jacquot, A.; Auchet, T.; Kimmoun, A. Vasoplegia treatments: The past, the present, and the future. Crit. Care 2018, 22, 52. [Google Scholar] [CrossRef] [Green Version]
- Pacher, P.; Beckman, J.S.; Liaudet, L. Nitric oxide and peroxynitrite in health and disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef] [Green Version]
- Delgado, R.; Rojas, A.; Glaría, L.A.; Torres, M.; Duarte, F.; Shill, R.; Nafeh, M.; Santin, E.; González, N.; Palacios, M. Ca(2+)-independent nitric oxide synthase activity in human lung after cardiopulmonary bypass. Thorax 1995, 50, 403–404. [Google Scholar] [CrossRef]
- Hill, G.E.; Snider, S.; Galbraith, T.A.; Forst, S.; Robbins, R.A. Glucocorticoid reduction of bronchial epithelial inflammation during cardiopulmonary bypass. Am. J. Respir. Crit. Care Med. 1995, 152, 1791–1795. [Google Scholar] [CrossRef] [PubMed]
- Sobey, C.G. Potassium Channel Function in Vascular Disease. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 28–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colson, P.H.; Bernard, C.; Struck, J.; Morgenthaler, N.G.; Albat, B.; Guillon, G. Post cardiac surgery vasoplegia is associated with high preoperative copeptin plasma concentration. Crit. Care 2011, 15, R255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Ashton, R.C., Jr.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin deficiency contributes to the vasodilation of septic shock. Circulation 1997, 95, 1122–1125. [Google Scholar] [CrossRef]
- Cuda, L.; Liaudet, L.; Ben-Hamouda, N. [Vasopressin in the critically ill patient]. Rev. Med. Suisse 2020, 16, 652–656. [Google Scholar]
- Wakatsuki, T.; Nakaya, Y.; Inoue, I. Vasopressin modulates K(+)-channel activities of cultured smooth muscle cells from porcine coronary artery. Am J. Physiol. 1992, 263, H491–H496. [Google Scholar] [CrossRef]
- Barrett, L.K.; Singer, M.; Clapp, L.H. Vasopressin: Mechanisms of action on the vasculature in health and in septic shock. Crit. Care Med. 2007, 35, 33–40. [Google Scholar] [CrossRef]
- Emori, T.; Hirata, Y.; Ohta, K.; Kanno, K.; Eguchi, S.; Imai, T.; Shichiri, M.; Marumo, F. Cellular mechanism of endothelin-1 release by angiotensin and vasopressin. Hypertension 1991, 18, 165–170. [Google Scholar] [CrossRef] [Green Version]
- Imai, T.; Hirata, Y.; Emori, T.; Yanagisawa, M.; Masaki, T.; Marumo, F. Induction of endothelin-1 gene by angiotensin and vasopressin in endothelial cells. Hypertension 1992, 19, 753–757. [Google Scholar] [CrossRef] [Green Version]
- Siess, W.; Stifel, M.; Binder, H.; Weber, P.C. Activation of V1-receptors by vasopressin stimulates inositol phospholipid hydrolysis and arachidonate metabolism in human platelets. Biochem. J. 1986, 233, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Ko, E.A.; Han, J.; Jung, I.D.; Park, W.S. Physiological roles of K+ channels in vascular smooth muscle cells. J. Smooth Muscle Res. 2008, 44, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.W. Modulation of ATP-sensitive K+ channels in skeletal muscle by intracellular protons. Nature 1990, 343, 375–377. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.C.; Li, Q. Lactate activates ATP-sensitive potassium channels in guinea pig ventricular myocytes. J. Clin. Investig. 1991, 88, 1772–1777. [Google Scholar] [CrossRef] [PubMed]
- Landry, D.W.; Oliver, J.A. The ATP-sensitive K+ channel mediates hypotension in endotoxemia and hypoxic lactic acidosis in dog. J. Clin. Investig. 1992, 89, 2071–2074. [Google Scholar] [CrossRef]
- Tang, G.; Wu, L.; Liang, W.; Wang, R. Direct stimulation of K(ATP) channels by exogenous and endogenous hydrogen sulfide in vascular smooth muscle cells. Mol. Pharmacol. 2005, 68, 1757–1764. [Google Scholar] [CrossRef] [Green Version]
- Liaudet, L.; Szabo, C. Blocking mineralocorticoid receptor with spironolactone may have a wide range of therapeutic actions in severe COVID-19 disease. Crit. Care 2020, 24, 318. [Google Scholar] [CrossRef]
- Chow, J.H.; Wittwer, E.D.; Wieruszewski, P.M.; Khanna, A.K. Evaluating the evidence for angiotensin II for the treatment of vasoplegia in critically ill cardiothoracic surgery patients. J. Thorac. Cardiovasc. Surg. 2022, 163, 1407–1414. [Google Scholar] [CrossRef]
- Myers, G.J.; Wegner, J. Endothelial Glycocalyx and Cardiopulmonary Bypass. J. Extra Corpor. Technol. 2017, 49, 174–181. [Google Scholar]
- Voyvodic, P.L.; Min, D.; Liu, R.; Williams, E.; Chitalia, V.; Dunn, A.K.; Baker, A.B. Loss of Syndecan-1 Induces a Pro-inflammatory Phenotype in Endothelial Cells with a Dysregulated Response to Atheroprotective Flow. J. Biol. Chem. 2014, 289, 9547–9559. [Google Scholar] [CrossRef] [Green Version]
- Boer, C.; Koning, N.J.; Van Teeffelen, J.; Vonk, A.B.; Vink, H. Changes in microcirculatory perfusion during cardiac surgery are paralleled by alterations in glycocalyx integrity. Crit. Care 2013, 17, P212. [Google Scholar] [CrossRef] [Green Version]
- Abou-Arab, O.; Kamel, S.; Beyls, C.; Huette, P.; Bar, S.; Lorne, E.; Galmiche, A.; Guinot, P.G. Vasoplegia After Cardiac Surgery Is Associated with Endothelial Glycocalyx Alterations. J. Cardiothorac. Vasc. Anesth. 2020, 34, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Szabo, C. Hydrogen sulfide, an enhancer of vascular nitric oxide signaling: Mechanisms and implications. Am. J. Physiol. Cell Physiol. 2017, 312, C3–C15. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, A.K.; Sikka, G.; Gazi, S.K.; Steppan, J.; Jung, S.M.; Bhunia, A.K.; Barodka, V.M.; Gazi, F.K.; Barrow, R.K.; Wang, R.; et al. Hydrogen sulfide as endothelium-derived hyperpolarizing factor sulfhydrates potassium channels. Circ. Res. 2011, 109, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Coletta, C.; Szabo, C. Potential role of hydrogen sulfide in the pathogenesis of vascular dysfunction in septic shock. Curr. Vasc. Pharmacol. 2013, 11, 208–221. [Google Scholar] [PubMed]
- Burnes, M.L.; Boettcher, B.T.; Woehlck, H.J.; Zundel, M.T.; Iqbal, Z.; Pagel, P.S. Hydroxocobalamin as a Rescue Treatment for Refractory Vasoplegic Syndrome After Prolonged Cardiopulmonary Bypass. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1012–1014. [Google Scholar] [CrossRef]
- Roderique, J.D.; VanDyck, K.; Holman, B.; Tang, D.; Chui, B.; Spiess, B.D. The Use of High-Dose Hydroxocobalamin for Vasoplegic Syndrome. Ann. Thorac. Surg. 2014, 97, 1785–1786. [Google Scholar] [CrossRef]
- Tsiouris, A.; Wilson, L.; Haddadin, A.S.; Yun, J.J.; Mangi, A.A. Risk assessment and outcomes of vasoplegia after cardiac surgery. Gen. Thorac. Cardiovasc. Surg. 2017, 65, 557–565. [Google Scholar] [CrossRef]
- van Vessem, M.E.; Palmen, M.; Couperus, L.E.; Mertens, B.; Berendsen, R.R.; Tops, L.F.; Verwey, H.F.; de Jonge, E.; Klautz, R.J.; Schalij, M.J.; et al. Incidence and predictors of vasoplegia after heart failure surgery. Eur. J. Cardiothorac. Surg. 2017, 51, 532–538. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar] [CrossRef]
- Asleh, R.; Alnsasra, H.; Daly, R.C.; Schettle, S.D.; Briasoulis, A.; Taher, R.; Dunlay, S.M.; Stulak, J.M.; Behfar, A.; Pereira, N.L.; et al. Predictors and Clinical Outcomes of Vasoplegia in Patients Bridged to Heart Transplantation with Continuous-Flow Left Ventricular Assist Devices. J. Am. Heart Assoc. 2019, 8, e013108. [Google Scholar] [CrossRef]
- Bolton, C.H.; Downs, L.G.; Victory, J.G.; Dwight, J.F.; Tomson, C.R.; Mackness, M.I.; Pinkney, J.H. Endothelial dysfunction in chronic renal failure: Roles of lipoprotein oxidation and pro-inflammatory cytokines. Nephrol. Dial. Transplant. 2001, 16, 1189–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, S.G.; Fida, N. Should angiotensin converting enzyme inhibitors/angiotensin II receptor antagonists be omitted before cardiac surgery to avoid postoperative vasodilation? Interact. Cardiovasc. Thorac. Surg. 2008, 7, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J.J.; Nouthe, B.; Sia, Y.T.; Spaziano, M. Effect of preoperative renin-angiotensin system blockade on vasoplegia after cardiac surgery: A systematic review with meta-analysis. World J. Cardiol. 2022, 14, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Pigott, D.W.; Nagle, C.; Allman, K.; Westaby, S.; Evans, R.D. Effect of omitting regular ACE inhibitor medication before cardiac surgery on haemodynamic variables and vasoactive drug requirements. Br. J. Anaesth. 1999, 83, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Webb, C.M.; Underwood, R.; Anagnostopoulos, C.; Bennett, J.G.; Pepper, J.; Lincoln, C.; Collins, P. The effect of angiotensin converting enzyme inhibition on myocardial function and blood pressure after coronary artery bypass surgery--a randomised study. Eur. J. Cardiothorac. Surg. 1998, 13, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Ten Broecke, P.W.; De Hert, S.G.; Mertens, E.; Adriaensen, H.F. Effect of preoperative beta-blockade on perioperative mortality in coronary surgery. Br. J. Anaesth. 2003, 90, 27–31. [Google Scholar] [CrossRef]
- Patarroyo, M.; Simbaqueba, C.; Shrestha, K.; Starling, R.C.; Smedira, N.; Tang, W.H.; Taylor, D.O. Pre-operative risk factors and clinical outcomes associated with vasoplegia in recipients of orthotopic heart transplantation in the contemporary era. J. Heart Lung Transplant. 2012, 31, 282–287. [Google Scholar] [CrossRef]
- Byrne, J.G.; Leacche, M.; Paul, S.; Mihaljevic, T.; Rawn, J.D.; Shernan, S.K.; Mudge, G.H.; Stevenson, L.W. Risk factors and outcomes for ‘vasoplegia syndrome’ following cardiac transplantation. Eur. J. Cardiothorac. Surg. 2004, 25, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Gomes, W.J.; Carvalho, A.C.; Palma, J.H.; Teles, C.A.; Branco, J.N.; Silas, M.G.; Buffolo, E. Vasoplegic syndrome after open heart surgery. J. Cardiovasc. Surg. 1998, 39, 619–623. [Google Scholar]
- Landis, R.C.; Brown, J.R.; Fitzgerald, D.; Likosky, D.S.; Shore-Lesserson, L.; Baker, R.A.; Hammon, J.W. Attenuating the Systemic Inflammatory Response to Adult Cardiopulmonary Bypass: A Critical Review of the Evidence Base. J. Extra Corpor. Technol. 2014, 46, 197–211. [Google Scholar]
- Anastasiadis, K.; Antonitsis, P.; Haidich, A.B.; Argiriadou, H.; Deliopoulos, A.; Papakonstantinou, C. Use of minimal extracorporeal circulation improves outcome after heart surgery; a systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. 2013, 164, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; De Backer, D. Circulatory Shock. N. Engl. J. Med. 2013, 369, 1726–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, R. Stressed vs. unstressed volume and its relevance to critical care practitioners. Clin. Exp. Emerg. Med. 2016, 3, 52–54. [Google Scholar] [CrossRef]
- Boyd, J.H.; Forbes, J.; Nakada, T.A.; Walley, K.R.; Russell, J.A. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit. Care Med. 2011, 39, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, F.; Meade, M.O.; Hébert, P.C.; Asfar, P.; Lauzier, F.; Seely, A.J.E.; Day, A.G.; Mehta, S.; Muscedere, J.; Bagshaw, S.M.; et al. Higher versus lower blood pressure targets for vasopressor therapy in shock: A multicentre pilot randomized controlled trial. Intensive Care Med. 2016, 42, 542–550. [Google Scholar] [CrossRef]
- Marik, P.E. Early Management of Severe Sepsis: Concepts and Controversies. Chest 2014, 145, 1407–1418. [Google Scholar] [CrossRef] [Green Version]
- Hernández, G.; Ospina-Tascón, G.A.; Damiani, L.P.; Estenssoro, E.; Dubin, A.; Hurtado, J.; Friedman, G.; Castro, R.; Alegría, L.; Teboul, J.L.; et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients with Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. J. Am. Med. Assoc. 2019, 321, 654–664. [Google Scholar] [CrossRef]
- Ltaief, Z.; Schneider, A.G.; Liaudet, L. Pathophysiology and clinical implications of the veno-arterial PCO2 gap. Crit. Care 2021, 25, 318. [Google Scholar] [CrossRef]
- Shaefi, S.; Mittel, A.; Klick, J.; Evans, A.; Ivascu, N.S.; Gutsche, J.; Augoustides, J.G.T. Vasoplegia After Cardiovascular Procedures-Pathophysiology and Targeted Therapy. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1013–1022. [Google Scholar] [CrossRef]
- Desai, N.; Garry, D. Assessing dynamic fluid-responsiveness using transthoracic echocardiography in intensive care. BJA Educ. 2018, 18, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Muller, L.; Toumi, M.; Bousquet, P.J.; Riu-Poulenc, B.; Louart, G.; Candela, D.; Zoric, L.; Suehs, C.; de La Coussaye, J.E.; Molinari, N.; et al. An increase in aortic blood flow after an infusion of 100 ml colloid over 1 minute can predict fluid responsiveness: The mini-fluid challenge study. Anesthesiology 2011, 115, 541–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, A.; Lionetti, G.; Foti, L.; Bellotti, E.; Marcomini, N.; Cammarota, G.; Bennett, V.; Saderi, L.; Sotgiu, G.; Della Corte, F.; et al. Mini fluid chAllenge aNd End-expiratory occlusion test to assess flUid responsiVEness in the opeRating room (MANEUVER study): A multicentre cohort study. Eur. J. Anaesthesiol. 2021, 38, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, L.A.; Vincent, J.L.; Galas, F.R.; Nakamura, R.E.; Silva, C.M.; Santos, M.H.; Fukushima, J.; Kalil Filho, R.; Sierra, D.B.; Lopes, N.H.; et al. Transfusion requirements after cardiac surgery: The TRACS randomized controlled trial. JAMA 2010, 304, 1559–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, C.G.; Sessler, D.I.; Mascha, E.J.; Sabik, J.F., 3rd; Li, L.; Duncan, A.I.; Zimmerman, N.M.; Blackstone, E.H. A Randomized Clinical Trial of Red Blood Cell Transfusion Triggers in Cardiac Surgery. Ann. Thorac. Surg. 2017, 104, 1243–1250. [Google Scholar] [CrossRef]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Medicis, E.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef]
- Murphy, G.J.; Pike, K.; Rogers, C.A.; Wordsworth, S.; Stokes, E.A.; Angelini, G.D.; Reeves, B.C.; Investigators, T.I. Liberal or restrictive transfusion after cardiac surgery. N. Engl. J. Med. 2015, 372, 997–1008. [Google Scholar] [CrossRef] [Green Version]
- Mueller, M.M.; Van Remoortel, H.; Meybohm, P.; Aranko, K.; Aubron, C.; Burger, R.; Carson, J.L.; Cichutek, K.; De Buck, E.; Devine, D.; et al. Patient Blood Management: Recommendations From the 2018 Frankfurt Consensus Conference. JAMA 2019, 321, 983–997. [Google Scholar] [CrossRef]
- Tibi, P.; McClure, R.S.; Huang, J.; Baker, R.A.; Fitzgerald, D.; Mazer, C.D.; Stone, M.; Chu, D.; Stammers, A.H.; Dickinson, T.; et al. STS/SCA/AmSECT/SABM Update to the Clinical Practice Guidelines on Patient Blood Management. Ann. Thorac. Surg. 2021, 112, 981–1004. [Google Scholar] [CrossRef]
- Anand, I.S.; Chandrashekhar, Y.; Wander, G.S.; Chawla, L.S. Endothelium-derived relaxing factor is important in mediating the high output state in chronic severe anemia. J. Am. Coll. Cardiol. 1995, 25, 1402–1407. [Google Scholar] [CrossRef] [Green Version]
- Martin, W.; Smith, J.A.; White, D.G. The mechanisms by which haemoglobin inhibits the relaxation of rabbit aorta induced by nitrovasodilators, nitric oxide, or bovine retractor penis inhibitory factor. Br. J. Pharmacol. 1986, 89, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Atsma, F.; Veldhuizen, I.; de Kort, W.; van Kraaij, M.; Pasker-de Jong, P.; Deinum, J. Hemoglobin level is positively associated with blood pressure in a large cohort of healthy individuals. Hypertension 2012, 60, 936–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asfar, P.; Meziani, F.; Hamel, J.F.; Grelon, F.; Megarbane, B.; Anguel, N.; Mira, J.P.; Dequin, P.F.; Gergaud, S.; Weiss, N.; et al. High versus low blood-pressure target in patients with septic shock. N. Engl. J. Med. 2014, 370, 1583–1593. [Google Scholar] [CrossRef] [Green Version]
- Lamontagne, F.; Richards-Belle, A.; Thomas, K.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Camsooksai, J.; Darnell, R.; Gordon, A.C.; Henry, D.; et al. Effect of Reduced Exposure to Vasopressors on 90-Day Mortality in Older Critically Ill Patients with Vasodilatory Hypotension: A Randomized Clinical Trial. J. Am. Med. Assoc. 2020, 323, 938–949. [Google Scholar] [CrossRef]
- De Backer, D.; Cecconi, M.; Lipman, J.; Machado, F.; Myatra, S.N.; Ostermann, M.; Perner, A.; Teboul, J.L.; Vincent, J.L.; Walley, K.R. Challenges in the management of septic shock: A narrative review. Intensive Care Med. 2019, 45, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, H.; Zhang, D. Timing of norepinephrine initiation in patients with septic shock: A systematic review and meta-analysis. Crit. Care 2020, 24, 488. [Google Scholar] [CrossRef] [PubMed]
- Bakker, J.; Kattan, E.; Annane, D.; Castro, R.; Cecconi, M.; De Backer, D.; Dubin, A.; Evans, L.; Gong, M.N.; Hamzaoui, O.; et al. Current practice and evolving concepts in septic shock resuscitation. Intensive Care Med. 2022, 48, 148–163. [Google Scholar] [CrossRef] [PubMed]
- Guarracino, F.; Habicher, M.; Treskatsch, S.; Sander, M.; Szekely, A.; Paternoster, G.; Salvi, L.; Lysenko, L.; Gaudard, P.; Giannakopoulos, P.; et al. Vasopressor Therapy in Cardiac Surgery-An Experts’ Consensus Statement. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1018–1029. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Bastien, O.; Bendjelid, K.; Cariou, A.; Chouihed, T.; Combes, A.; Mebazaa, A.; Megarbane, B.; Plaisance, P.; Ouattara, A.; et al. Experts’ recommendations for the management of adult patients with cardiogenic shock. Ann. Intensive Care 2015, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). J. Am. Med. Assoc. 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Sponholz, C.; Schelenz, C.; Reinhart, K.; Schirmer, U.; Stehr, S.N. Catecholamine and volume therapy for cardiac surgery in Germany–results from a postal survey. PLoS ONE 2014, 9, e103996. [Google Scholar] [CrossRef] [Green Version]
- Stolk, R.F.; van der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; van der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef] [PubMed]
- Dünser, M.W.; Mayr, A.J.; Ulmer, H.; Knotzer, H.; Sumann, G.; Pajk, W.; Friesenecker, B.; Hasibeder, W.R. Arginine vasopressin in advanced vasodilatory shock: A prospective, randomized, controlled study. Circulation 2003, 107, 2313–2319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torgersen, C.; Dünser, M.W.; Wenzel, V.; Jochberger, S.; Mayr, V.; Schmittinger, C.A.; Lorenz, I.; Schmid, S.; Westphal, M.; Grander, W.; et al. Comparing two different arginine vasopressin doses in advanced vasodilatory shock: A randomized, controlled, open-label trial. Intensive Care Med. 2010, 36, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, D.H.; Kim, J.S.; Lim, S.H.; Hong, Y.W. Comparative effects of norepinephrine and vasopressin on internal thoracic arterial graft flow after off-pump coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2011, 141, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Liu, X.; Hu, Y.; Li, W.; Li, N. The effect of vasopressin on the hemodynamics in CABG patients. J. Cardiothorac. Surg. 2013, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Dünser, M.W.; Bouvet, O.; Knotzer, H.; Arulkumaran, N.; Hajjar, L.A.; Ulmer, H.; Hasibeder, W.R. Vasopressin in Cardiac Surgery: A Meta-analysis of Randomized Controlled Trials. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2225–2232. [Google Scholar] [CrossRef]
- McIntyre, W.F.; Um, K.J.; Alhazzani, W.; Lengyel, A.P.; Hajjar, L.; Gordon, A.C.; Lamontagne, F.; Healey, J.S.; Whitlock, R.P.; Belley-Côté, E.P. Association of Vasopressin Plus Catecholamine Vasopressors vs Catecholamines Alone with Atrial Fibrillation in Patients with Distributive Shock: A Systematic Review and Meta-analysis. J. Am. Med. Assoc. 2018, 319, 1889–1900. [Google Scholar] [CrossRef]
- Nedel, W.L.; Rech, T.H.; Ribeiro, R.A.; Pellegrini, J.A.S.; Moraes, R.B. Renal Outcomes of Vasopressin and Its Analogs in Distributive Shock: A Systematic Review and Meta-Analysis of Randomized Trials. Crit. Care Med. 2019, 47, e44–e51. [Google Scholar] [CrossRef]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017, 377, 419–430. [Google Scholar] [CrossRef]
- Klijian, A.; Khanna, A.K.; Reddy, V.S.; Friedman, B.; Ortoleva, J.; Evans, A.S.; Panwar, R.; Kroll, S.; Greenfeld, C.R.; Chatterjee, S. Treatment with Angiotensin II Is Associated with Rapid Blood Pressure Response and Vasopressor Sparing in Patients With Vasoplegia After Cardiac Surgery: A Post-Hoc Analysis of Angiotensin II for the Treatment of High-Output Shock (ATHOS-3) Study. J. Cardiothorac. Vasc. Anesth. 2021, 35, 51–58. [Google Scholar] [CrossRef]
- Coulson, T.G.; Miles, L.F.; Serpa Neto, A.; Pilcher, D.; Weinberg, L.; Landoni, G.; Zarbock, A.; Bellomo, R. A double-blind randomised feasibility trial of angiotensin-2 in cardiac surgery. Anaesthesia 2022, 77, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Pushparajah Mak, R.S.; Liebelt, E.L. Methylene Blue: An Antidote for Methemoglobinemia and Beyond. Pediatr. Emerg. Care 2021, 37, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Kofler, O.; Simbeck, M.; Tomasi, R.; Hinske, L.C.; Klotz, L.V.; Uhle, F.; Born, F.; Pichlmaier, M.; Hagl, C.; Weigand, M.A.; et al. Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study. J. Clin. Med. 2022, 11, 1121. [Google Scholar] [CrossRef] [PubMed]
- Özal, E.; Kuralay, E.; Yildirim, V.; Kilic, S.; Bolcal, C.; Kücükarslan, N.; Günay, C.; Demirkilic, U.; Tatar, H. Preoperative Methylene Blue Administration in Patients at High Risk for Vasoplegic Syndrome During Cardiac Surgery. Ann. Thorac. Surg. 2005, 79, 1615–1619. [Google Scholar] [CrossRef]
- Kofidis, T.; Strüber, M.; Wilhelmi, M.; Anssar, M.; Simon, A.; Harringer, W.; Haverich, A. Reversal of severe vasoplegia with single-dose methylene blue after heart transplantation. J. Thorac. Cardiovasc. Surg. 2001, 122, 823–824. [Google Scholar] [CrossRef] [Green Version]
- Levin, R.L.; Degrange, M.A.; Bruno, G.F.; Del Mazo, C.D.; Taborda, D.J.; Griotti, J.J.; Boullon, F.J. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann. Thorac. Surg. 2004, 77, 496–499. [Google Scholar] [CrossRef]
- Yiu, P.; Robin, J.; Pattison, C.W. Reversal of refractory hypotension with single-dose methylene blue after coronary artery bypass surgery. J. Thorac. Cardiovasc. Surg. 1999, 118, 195–196. [Google Scholar] [CrossRef] [Green Version]
- Mehaffey, J.H.; Johnston, L.E.; Hawkins, R.B.; Charles, E.J.; Yarboro, L.; Kern, J.A.; Ailawadi, G.; Kron, I.L.; Ghanta, R.K. Methylene Blue for Vasoplegic Syndrome After Cardiac Operation: Early Administration Improves Survival. Ann. Thorac. Surg. 2017, 104, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Ramezanpour Ahangar, E.; Annamaraju, P. Hydroxocobalamin; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Weinberg, J.B.; Chen, Y.; Jiang, N.; Beasley, B.E.; Salerno, J.C.; Ghosh, D.K. Inhibition of nitric oxide synthase by cobalamins and cobinamides. Free Radic. Biol. Med. 2009, 46, 1626–1632. [Google Scholar] [CrossRef] [Green Version]
- Kruszyna, H.; Magyar, J.S.; Rochelle, L.G.; Russell, M.A.; Smith, R.P.; Wilcox, D.E. Spectroscopic studies of nitric oxide (NO) interactions with cobalamins: Reaction of NO with superoxocobalamin(III) likely accounts for cobalamin reversal of the biological effects of NO. J. Pharmacol. Exp. Ther. 1998, 285, 665–671. [Google Scholar]
- Haouzi, P.; Chenuel, B.; Sonobe, T. High-dose hydroxocobalamin administered after H2S exposure counteracts sulfide-poisoning-induced cardiac depression in sheep. Clin. Toxicol. 2015, 53, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, P.C.; Hendry-Hofer, T.B.; Witeof, A.E.; Brenner, M.; Mahon, S.B.; Boss, G.R.; Haouzi, P.; Bebarta, V.S. Hydrogen Sulfide Toxicity: Mechanism of Action, Clinical Presentation, and Countermeasure Development. J. Med. Toxicol. 2019, 15, 287–294. [Google Scholar] [CrossRef]
- Shapeton, A.D.; Mahmood, F.; Ortoleva, J.P. Hydroxocobalamin for the Treatment of Vasoplegia: A Review of Current Literature and Considerations for Use. J. Cardiothorac. Vasc. Anesth. 2019, 33, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Klemm, S.; Glienke, C. Evaluation of hydroxocobalamin in vasoplegia in cardiac surgery. Crit. Care Med. 2016, 44, 131. [Google Scholar] [CrossRef]
- Bak, M.A.; Smith, J.A.; Murfin, B.; Chen, Y. High-Dose Hydroxocobalamin for Refractory Vasoplegia Post Cardiac Surgery. Cureus 2022, 14, e28267. [Google Scholar] [CrossRef]
- Shah, P.R.; Reynolds, P.S.; Pal, N.; Tang, D.; McCarthy, H.; Spiess, B.D. Hydroxocobalamin for the treatment of cardiac surgery-associated vasoplegia: A case series. Can. J. Anaesth. 2018, 65, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Seelhammer, T.G.; Plack, D.; Nei, S.; Wittwer, E.; Nelson, J.; Nabzdyk, C.G.S. Extended duration infusion of high-dose hydroxocobalamin for vasoplegic syndrome following cardiac surgery. Heart Lung 2021, 50, 173–176. [Google Scholar] [CrossRef]
- Carr, A.C.; Shaw, G.M.; Fowler, A.A.; Natarajan, R. Ascorbate-dependent vasopressor synthesis: A rationale for vitamin C administration in severe sepsis and septic shock? Crit. Care 2015, 19, 418. [Google Scholar] [CrossRef] [Green Version]
- Dillon, P.F.; Root-Bernstein, R.S.; Lieder, C.M. Antioxidant-independent ascorbate enhancement of catecholamine-induced contractions of vascular smooth muscle. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H2353–H2360. [Google Scholar] [CrossRef]
- Berger, M.M.; Oudemans-van Straaten, H.M. Vitamin C supplementation in the critically ill patient. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 193–201. [Google Scholar] [CrossRef]
- Rodemeister, S.; Duquesne, M.; Adolph, M.; Nohr, D.; Biesalski, H.K.; Unertl, K. Massive and long-lasting decrease in vitamin C plasma levels as a consequence of extracorporeal circulation. Nutrition 2014, 30, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Yanase, F.; Bitker, L.; Hessels, L.; Osawa, E.; Naorungroj, T.; Cutuli, S.L.; Young, P.J.; Ritzema, J.; Hill, G.; Latimer-Bell, C.; et al. A Pilot, Double-Blind, Randomized, Controlled Trial of High-Dose Intravenous Vitamin C for Vasoplegia After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2020, 34, 409–416. [Google Scholar] [CrossRef]
- Lamontagne, F.; Masse, M.H.; Menard, J.; Sprague, S.; Pinto, R.; Heyland, D.K.; Cook, D.J.; Battista, M.C.; Day, A.G.; Guyatt, G.H.; et al. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. N. Engl. J. Med. 2022, 386, 2387–2398. [Google Scholar] [CrossRef] [PubMed]
- Wacker, D.A.; Burton, S.L.; Berger, J.P.; Hegg, A.J.; Heisdorffer, J.; Wang, Q.; Medcraft, E.J.; Reilkoff, R.A. Evaluating Vitamin C in Septic Shock: A Randomized Controlled Trial of Vitamin C Monotherapy. Crit. Care Med. 2022, 50, e458–e467. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, B.; Cohen, J. Hydrocortisone in Vasodilatory Shock. Crit. Care Clin. 2019, 35, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Mak, J.C.; Nishikawa, M.; Barnes, P.J. Glucocorticosteroids increase beta 2-adrenergic receptor transcription in human lung. Am. J. Physiol. 1995, 268, L41–L46. [Google Scholar] [CrossRef]
- Sakaue, M.; Hoffman, B.B. Glucocorticoids induce transcription and expression of the alpha 1B adrenergic receptor gene in DTT1 MF-2 smooth muscle cells. J. Clin. Investig. 1991, 88, 385–389. [Google Scholar] [CrossRef]
- Annane, D.; Renault, A.; Brun-Buisson, C.; Megarbane, B.; Quenot, J.P.; Siami, S.; Cariou, A.; Forceville, X.; Schwebel, C.; Martin, C.; et al. Hydrocortisone plus Fludrocortisone for Adults with Septic Shock. N. Engl. J. Med. 2018, 378, 809–818. [Google Scholar] [CrossRef]
- Annane, D.; Sébille, V.; Charpentier, C.; Bollaert, P.E.; François, B.; Korach, J.M.; Capellier, G.; Cohen, Y.; Azoulay, E.; Troché, G.; et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. J. Am. Med. Assoc. 2002, 288, 862–871. [Google Scholar] [CrossRef] [Green Version]
- Sprung, C.L.; Annane, D.; Keh, D.; Moreno, R.; Singer, M.; Freivogel, K.; Weiss, Y.G.; Benbenishty, J.; Kalenka, A.; Forst, H.; et al. Hydrocortisone therapy for patients with septic shock. N. Engl. J. Med. 2008, 358, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, B.; Finfer, S.; Cohen, J.; Rajbhandari, D.; Arabi, Y.; Bellomo, R.; Billot, L.; Correa, M.; Glass, P.; Harward, M.; et al. Adjunctive Glucocorticoid Therapy in Patients with Septic Shock. N. Engl. J. Med. 2018, 378, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.M.; Nierich, A.P.; Rosseel, P.M.; van der Maaten, J.M.; Hofland, J.; Diephuis, J.C.; Schepp, R.M.; Boer, C.; Moons, K.G.; van Herwerden, L.A.; et al. Intraoperative high-dose dexamethasone for cardiac surgery: A randomized controlled trial. J. Am. Med. Assoc. 2012, 308, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, R.; Young, E.; Noora, J.; Farrokhyar, F.; Blackall, M.; Teoh, K. Pulse low dose steroids attenuate post-cardiopulmonary bypass SIRS.; SIRS I. J. Surg. Res. 2006, 132, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Chai, T.; Zhuang, X.; Tian, M.; Yang, X.; Qiu, Z.; Xu, S.; Cai, M.; Lin, Y.; Chen, L. Meta-Analysis: Shouldn’t Prophylactic Corticosteroids be Administered During Cardiac Surgery with Cardiopulmonary Bypass? Front. Surg. 2022, 9, 832205. [Google Scholar] [CrossRef]
- Ricci, Z.; Romagnoli, S.; Reis, T.; Bellomo, R.; Ronco, C. Hemoperfusion in the intensive care unit. Intensive Care Med. 2022, 48, 1397–1408. [Google Scholar] [CrossRef]
- Diab, M.; Lehmann, T.; Bothe, W.; Akhyari, P.; Platzer, S.; Wendt, D.; Deppe, A.-C.; Strauch, J.; Hagel, S.; Günther, A.; et al. Cytokine Hemoadsorption During Cardiac Surgery Versus Standard Surgical Care for Infective Endocarditis (REMOVE): Results from a Multicenter Randomized Controlled Trial. Circulation 2022, 145, 959–968. [Google Scholar] [CrossRef]
- Goetz, G.; Hawlik, K.; Wild, C. Extracorporeal Cytokine Adsorption Therapy As a Preventive Measure in Cardiac Surgery and As a Therapeutic Add-On Treatment in Sepsis: An Updated Systematic Review of Comparative Efficacy and Safety. Crit. Care Med. 2021, 49, 1347–1357. [Google Scholar] [CrossRef]
- Heymann, M.; Schorer, R.; Putzu, A. Mortality and adverse events of hemoadsorption with CytoSorb® in critically ill patients: A systematic review and meta-analysis of randomized controlled trials. Acta Anaesthesiol. Scand. 2022. [Google Scholar] [CrossRef]


{kind=link}
| Definition | Distributive Form of Circulatory Shock ≤ 24 h after CPB Initiation, Characterized by:
|
| Predisposing factors | |
| Patient-related factors | Advanced age; anemia; low LVEF; renal failure |
| Pre-/peri-operative drugs | Diuretics; sympatho-adrenergic inotropes; ACEI (controversial) |
| Operative factors | CPB/aortic cross clamping time; redo surgery; combined surgery; LVAD surgery; HTx |
| Pathophysiology | |
| Initiating events | Systemic inflammatory response triggered by:
|
| Mechanisms of pathological vasodilation |
|
| Outcome |
|
| Management |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ltaief, Z.; Ben-Hamouda, N.; Rancati, V.; Gunga, Z.; Marcucci, C.; Kirsch, M.; Liaudet, L. Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care. J. Clin. Med. 2022, 11, 6407. https://doi.org/10.3390/jcm11216407
Ltaief Z, Ben-Hamouda N, Rancati V, Gunga Z, Marcucci C, Kirsch M, Liaudet L. Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care. Journal of Clinical Medicine. 2022; 11(21):6407. https://doi.org/10.3390/jcm11216407
Chicago/Turabian StyleLtaief, Zied, Nawfel Ben-Hamouda, Valentina Rancati, Ziyad Gunga, Carlo Marcucci, Matthias Kirsch, and Lucas Liaudet. 2022. "Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care" Journal of Clinical Medicine 11, no. 21: 6407. https://doi.org/10.3390/jcm11216407