

One-Year Visual Outcomes and Corneal Higher-Order Aberration Assessment of Small-Incision Lenticule Extraction for the Treatment of Myopia and Myopic Astigmatism
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
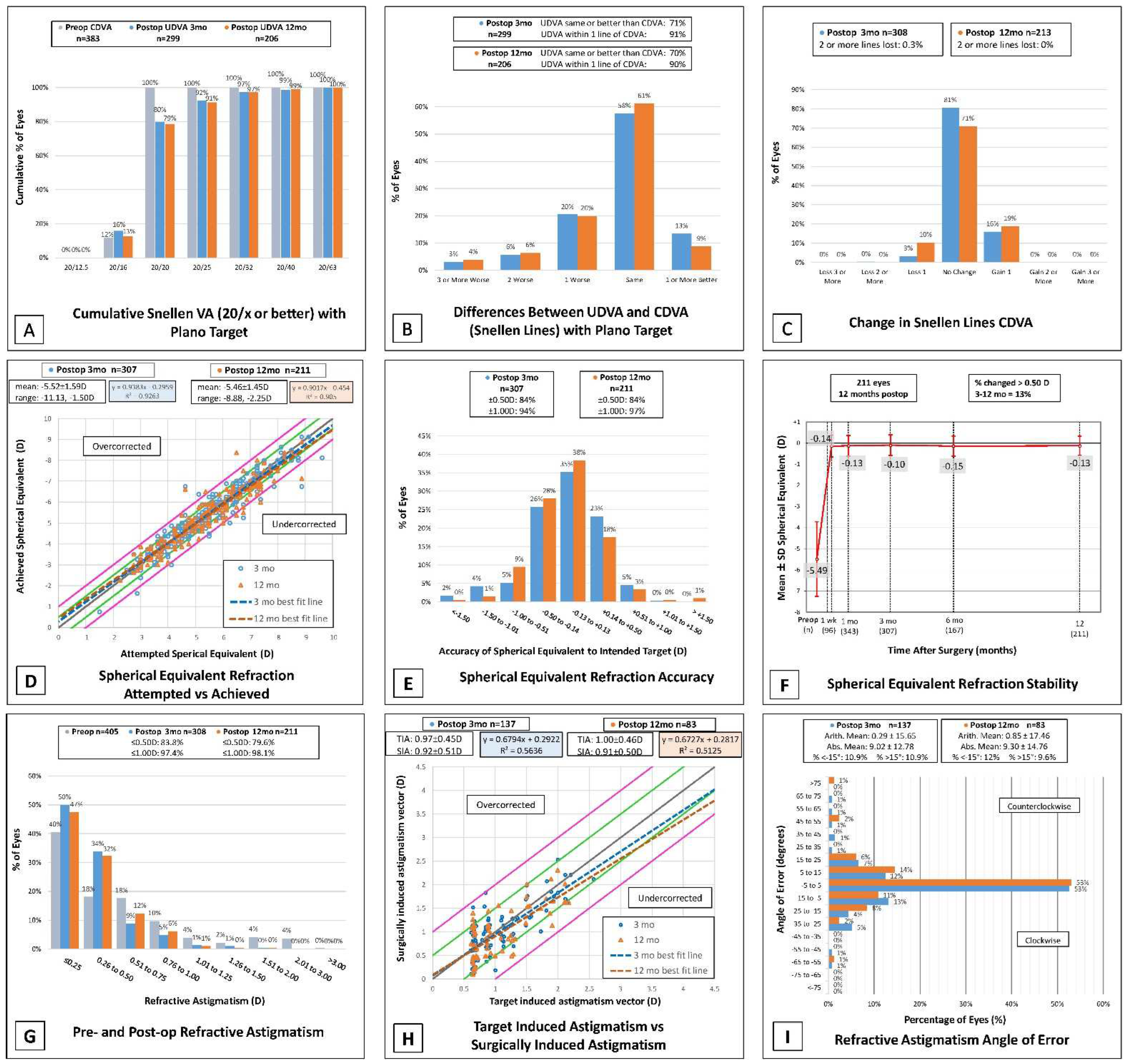
3.2. Efficacy, Visual Acuity, and Safety
3.3. Accuracy and Stability
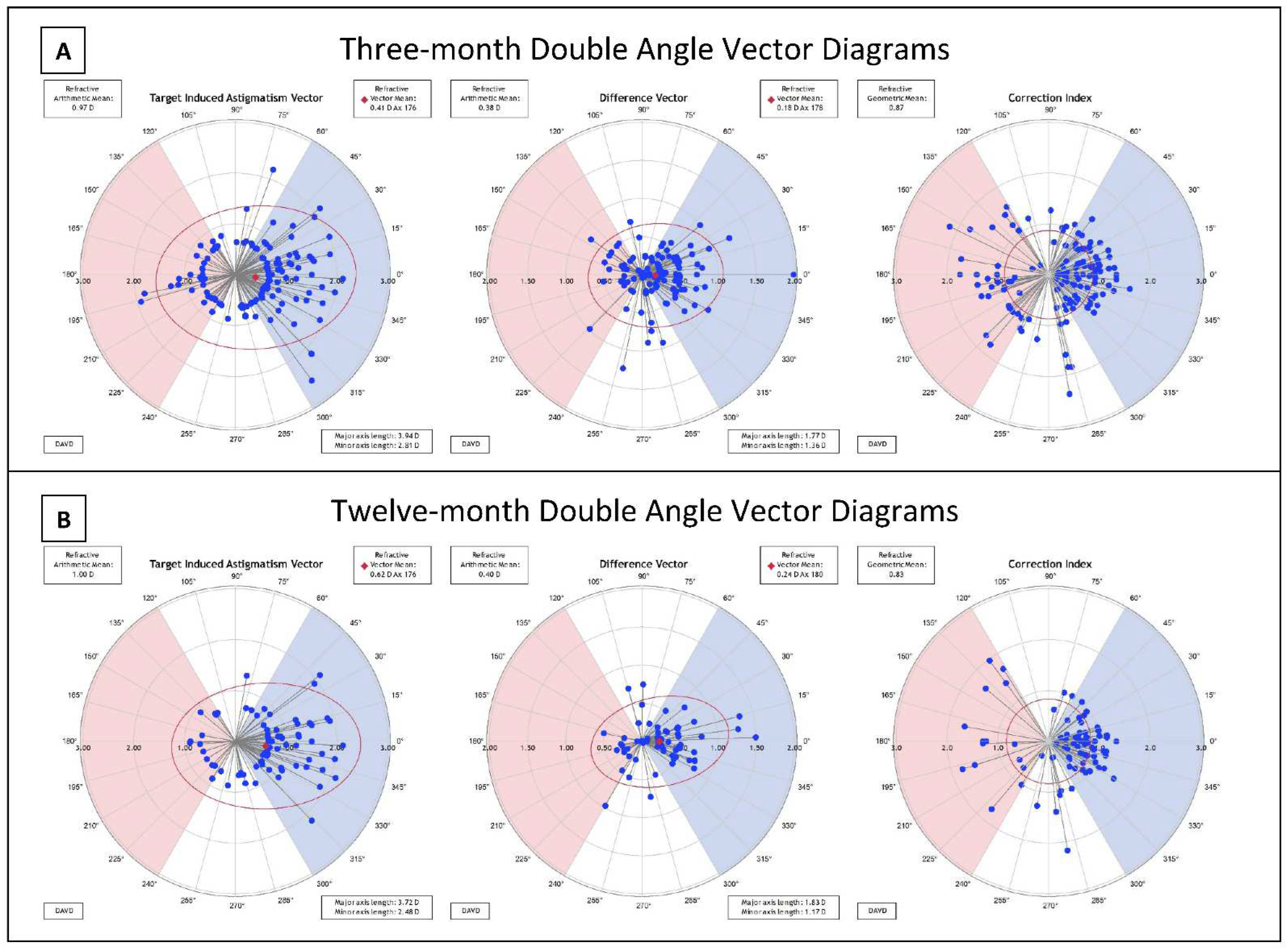
3.4. Astigmatism and Vector Analysis
3.5. Long-Term Outcomes beyond 12 Months
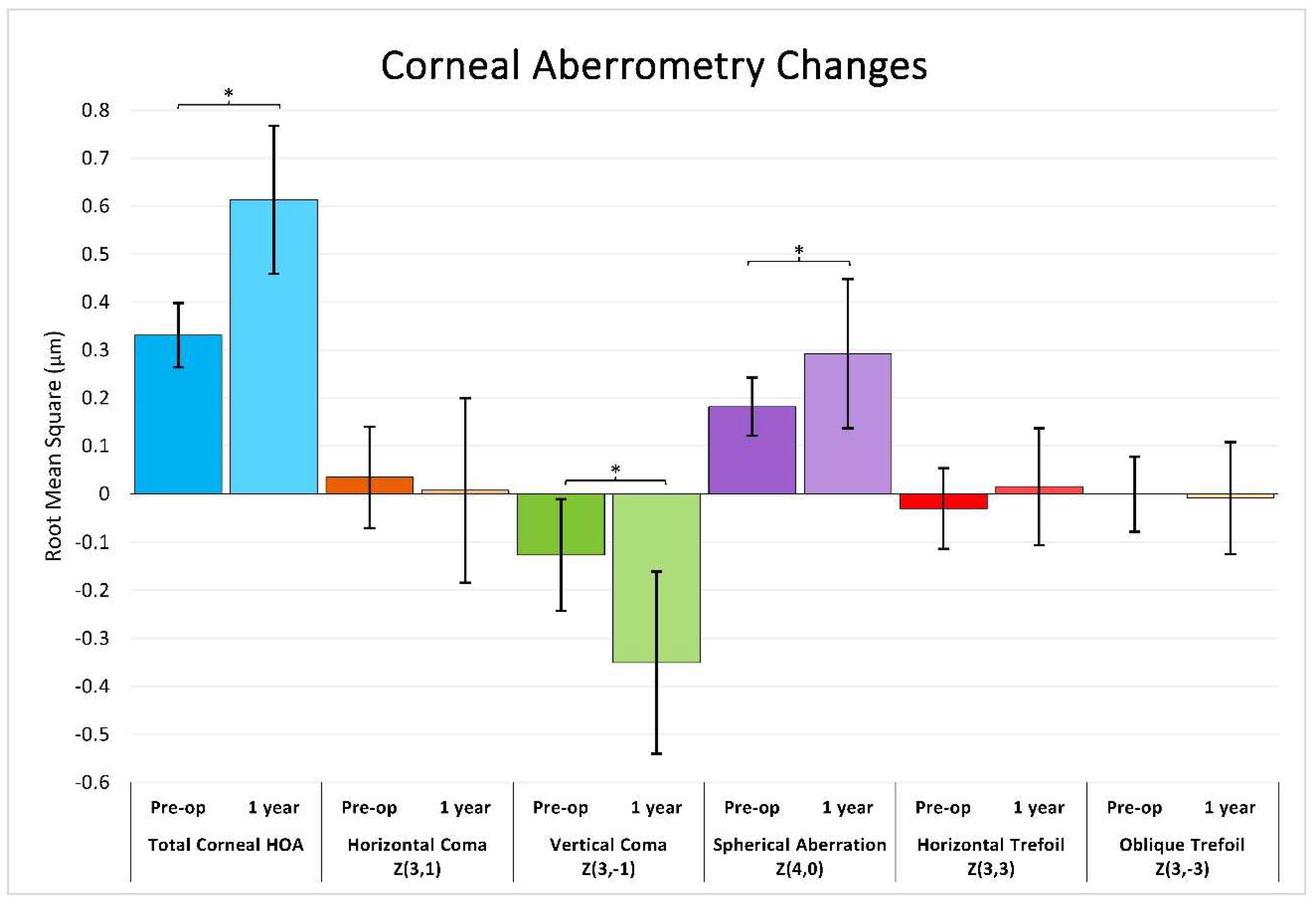
3.6. Corneal Wavefront Aberrometry
3.7. Adverse Events and Complications
4. Discussion

{kind=link}
{kind=link}
{kind=link}
| Study | Year | Preop SEQ (SD) | Preop Sph (SD) | Preop Cyl (SD) | n | %UDVA ≥ 20/20 | %UDVA ≥ 20/40 | %CDVA Loss ≥ 2 lines | %SEQ ≤ 0.50 D | %SEQ ≤ 1.00 D |
|---|---|---|---|---|---|---|---|---|---|---|
| 3 months | ||||||||||
| Current Study | 2022 | −5.59 (1.62) | −5.29 (1.60) | −0.62 (0.60) | 308 | 80% | 99% | 0.30% | 84% | 94% |
| Ivarsen and Hjortdal [15] | 2014 | --- | --- | <−2.50 D | 669 | --- | 81% ≥20/25 | 2.80% | --- | --- |
| ≥−2.50 D | 106 | --- | 64% ≥20/25 | 0.90% | --- | --- | ||||
| Hjordtal et al. [16] | 2012 | −7.19 (1.30) | −6.41 (1.77) | −0.60 (0.46) | 670 | --- | --- | --- | 80.10% | 94.20% |
| Hansen et al. [17] | 2016 | −6.82 (1.66) | --- | −0.83 (0.84) | 722 | --- | 83% ≥20/25 | 1.60% | 88% | 98% |
| Kamiya et al. (multi- center) [18] | 2019 | −4.33 (1.61) | --- | −0.64 (0.51) | 252 | 100% | 100% | 0.80% | 88% | 98% |
| Liu et al. (3–6 mo) [19] | 2021 | −4.96 (2.07) | --- | −1.04 (0.77) | 462 | 93% | --- | 0% | 98% | 100% |
| 12 months | ||||||||||
| Current Study | 2022 | −5.55 (1.48) | −5.22 (1.43) | −0.58 (0.61) | 213 | 79% | 99% | 0% | 84% | 97% |
| VisuMax FDA PMA [4] | 2018 | −5.48 | −4.82 (2.39) | −1.34 (0.80) | 349 | 89.40% | 98.90% | 0% | 94.80% | 99.10% |
| Dishler et al. [20] | 2020 | −5.41 (2.31) | −4.65 (2.33) | −1.52 (0.70) | 300 | 89.00% | 99.00% | 0% | 95.30% | 99.30% |
| Chansue et al. [21] | 2015 | −4.96 (1.88) | −4.61 (1.85) | −0.71 (0.61) | 318/347 | 90% | 98% | 0% | 93% | 99% |
| Wu et al. [22] | 2016 | <−6.0 D | −6.49 (0.93) | −0.82 (0.68) | 65 | --- | --- | --- | 95.40% | 100% |
| ≥−6.0 D | −4.21 (1.10) | −0.95 (0.88) | 91 | --- | --- | --- | 96.70% | 100% | ||
| >1 year | ||||||||||
| Current Study (1.5–5 yrs) | 2022 | −4.91 (1.46) | −4.73 (1.45) | −0.36 (0.42) | 31 | 63% | 96.70% | 0% | 77.80% | 96.30% |
| Han et al. (3 yrs) [23] | 2019 | −6.54 (1.69) | −6.14 (1.62) | −0.80 (0.68) | 60 | 90% | --- | 2% lost 1 line | 80% | --- |
| Yildirim et al. (2 yrs) [24] | 2016 | −7.10 (0.95) | −6.64 (0.88) | −0.82 (0.55) | 45 | 80% | 100% | 2% lost 1 line | 92% | 100% |
| Tian et al. (5 yrs) [25] | 2022 | −7.16 (1.51) | −6.74 (1.45) | −0.84 (0.70) | 41 | 90.20% | 100% | 0% | 87.80% | 95.10% |
| Pedersen et al. (3 yrs) [26] | 2015 | −7.30 (1.40) | --- | −0.70 (0.60) | 87 | 72% | --- | --- | 78% | 90% |
| Blum et al. (5 yrs) [27] | 2016 | --- | --- | --- | 56 | --- | --- | 0% | 48.20% | 78.60% |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sekundo, W.; Kunert, K.; Russmann, C.; Gille, A.; Bissmann, W.; Stobrawa, G.; Sticker, M.; Bischoff, M.; Blum, M. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia. Six-month results. J. Cataract Refract. Surg. 2008, 34, 1513–1520. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. Small incision lenticule extraction (SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes. Eye Vis. 2014, 1, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, R. History and Results; Indications and Contraindications of SMILE Compared with LASIK. Asia Pac. J. Ophthalmol. 2019, 8, 371–376. [Google Scholar] [CrossRef]
- FDA SSED SMILE (Visumax). 2018. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P150040 (accessed on 29 April 2022).
- Moshirfar, M.; Murri, M.S.; Shah, T.J.; Linn, S.H.; Ronquillo, Y.; Birdsong, O.C.; Hoopes, P.C., Jr. Initial Single-Site Surgical Experience with SMILE: A Comparison of Results to FDA SMILE, and the Earliest and Latest Generation of LASIK. Ophthalmol. Ther. 2018, 7, 347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holladay, J.T. Visual acuity measurements. J. Cataract Refract. Surg. 2004, 30, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Alpins, N. Astigmatism analysis by the Alpins method. J. Cataract Refract. Surg. 2001, 27, 31–49. [Google Scholar] [CrossRef]
- Moshirfar, M.; Thomson, A.C.; West, W.B.; Hall, M.N.; McCabe, S.E.; Thomson, R.J.; Ronquillo, Y.C.; Hoopes, P.C. Initial Single-Site Experience Using SMILE for the Treatment of Astigmatism in Myopic Eyes and Comparison of Astigmatic Outcomes with Existing Literature. Clin. Ophthalmol. 2020, 14, 3551. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Checklist of Information Usually Submitted in an Investigational Device Exemptions (IDE) Application for Refractive Surgery Lasers; U.S. Food and Drug Administration: Silver Spring, MD, USA, 1996.
- Schallhorn, J.M.; Schallhorn, S.C.; Hannan, S.J. Impact of Refractive Outcomes on Bias in Follow-up and Completion of Patient-Reported Outcome Measures after Laser Vision Correction. Ophthalmology 2021, 128, 1284–1291. [Google Scholar] [CrossRef]
- Jin, H.Y.; Wan, T.; Yu, X.N.; Yao, K. Corneal higher-order aberrations of the anterior surface, posterior surface, and total cornea after small incision lenticule extraction (SMILE): High myopia versus mild to moderate myopia. BMC Ophthalmol. 2018, 18, 295. [Google Scholar] [CrossRef] [Green Version]
- Sekundo, W.; Gertnere, J.; Bertelmann, T.; Solomatin, I. One-year refractive results, contrast sensitivity, high-order aberrations and complications after myopic small-incision lenticule extraction (ReLEx SMILE). Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 837–843. [Google Scholar] [CrossRef]
- Li, M.; Zhao, J.; Miao, H.; Shen, Y.; Sun, L.; Tian, M.; Wadium, E.; Zhou, X. Mild Decentration Measured by a Scheimpflug Camera and Its Impact on Visual Quality Following SMILE in the Early Learning Curve. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3886–3892. [Google Scholar] [CrossRef] [Green Version]
- Mrochen, M.; Kaemmerer, M.; Mierdel, P.; Seiler, T. Increased higher-order optical aberrations after laser refractive surgery: A problem of subclinical decentration. J. Cataract Refract. Surg. 2001, 27, 362–369. [Google Scholar] [CrossRef]
- Ivarsen, A.; Hjortdal, J. Correction of myopic astigmatism with small incision lenticule extraction. J. Refract. Surg. 2014, 30, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjortdal, J.; Vestergaard, A.H.; Ivarsen, A.; Ragunathan, S.; Asp, S. Predictors for the outcome of small-incision lenticule extraction for myopia. J. Refract. Surg. 2012, 28, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Hansen, R.S.; Lyhne, N.; Grauslund, J.; Vestergaard, A.H. Small-incision lenticule extraction (SMILE): Outcomes of 722 eyes treated for myopia and myopic astigmatism. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 399–405. [Google Scholar] [CrossRef]
- Kamiya, K.; Takahashi, M.; Nakamura, T.; Kojima, T.; Toda, I.; Kariya, M. A Multicenter Study on Early Outcomes of Small-Incision Lenticule Extraction for Myopia. Sci. Rep. 2019, 9, 4067. [Google Scholar] [CrossRef] [Green Version]
- Liu, E.T.; Sella, R.; Goernert, P.; Kim, K.; Chen, H.; Lin, R.T. Refractive results with SMILE using lower energy settings in the United States. PLoS ONE 2021, 16, e0258835. [Google Scholar] [CrossRef]
- Dishler, J.G.; Slade, S.; Seifert, S.; Schallhorn, S.C. Small-Incision Lenticule Extraction (SMILE) for the Correction of Myopia with Astigmatism: Outcomes of the United States Food and Drug Administration Premarket Approval Clinical Trial. Ophthalmology 2020, 127, 1020–1034. [Google Scholar] [CrossRef]
- Chansue, E.; Tanehsakdi, M.; Swasdibutra, S.; McAlinden, C. Efficacy, predictability and safety of small incision lenticule extraction (SMILE). Eye Vis. 2015, 2, 14. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Wang, Y.; Zhang, H.; Zhang, J.; Li, H.; Dou, R. One-year visual outcome of small incision lenticule extraction (SMILE) surgery in high myopic eyes: Retrospective cohort study. BMJ Open 2016, 6, e010993. [Google Scholar] [CrossRef]
- Han, T.; Xu, Y.; Han, X.; Zeng, L.; Shang, J.; Chen, X.; Zhou, X. Three-year outcomes of small incision lenticule extraction (SMILE) and femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK) for myopia and myopic astigmatism. Br. J. Ophthalmol. 2019, 103, 565. [Google Scholar] [CrossRef] [Green Version]
- Yıldırım, Y.; Alagöz, C.; Demir, A.; Ölçücü, O.; Özveren, M.; Ağca, A.; Özgürhan, E.B.; Demirok, A. Ori gi nal Ar tic le 200 Long-term Results of Small-incision Lenticule Extraction in High Myopia. Turk. J. Ophthalmol. 2016, 46, 200–204. [Google Scholar] [CrossRef]
- Tian, M.; Jian, W.; Miao, H.; Li, M.; Xia, F.; Zhou, X. Five-Year Follow-Up of Visual Outcomes and Optical Quality After Small Incision Lenticule Extraction for Moderate and High Myopia. Ophthalmol. Ther. 2022, 11, 355. [Google Scholar] [CrossRef]
- Pedersen, I.B.; Ivarsen, A.; Hjortdal, J. Three-Year Results of Small Incision Lenticule Extraction for High Myopia: Refractive Outcomes and Aberrations. J. Refract. Surg. 2015, 31, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Blum, M.; Täubig, K.; Gruhn, C.; Sekundo, W.; Kunert, K.S. Five-year results of Small Incision Lenticule Extraction (ReLEx SMILE). Br. J. Ophthalmol. 2016, 100, 1192–1195. [Google Scholar] [CrossRef]



| Demographics | Treated for Spherical Myopia Only | Treated for Astigmatic Myopia | All Treated Eyes | Targeted for Monovision | Required PRK Enhancement |
|---|---|---|---|---|---|
| Number of eyes | 217 eyes | 188 eyes | 405 eyes | 22 eyes | 15 eyes |
| (no. of patients) | (129 patients) | (116 patients) | (207 patients) | −5.40% | (11 patients) |
| Gender | |||||
| Male | 52 (40%) | 43 (37%) | 85 (41%) | 9 (41%) | 3 (20%) |
| Female | 77 (60%) | 73 (63%) | 122 (59%) | 13 (59%) | 8 (80%) |
| Surgical Eye | |||||
| OD | 111 (51%) | 92 (49%) | 203 (50%) | 4 (18%) | 6 (40%) |
| OS | 106 (49%) | 96 (51%) | 202 (50%) | 18 (82%) | 9 (60%) |
| Age (years) | |||||
| Mean (SD) | 34.4 (7.6) | 34.6 (7.9) | 34.5 (7.7) | 46.8 (4.5) | 34.2 (6.2) |
| Min., Max. | 18, 55 | 21, 57 | 18, 57 | 39, 54 | 25, 45 |
| MRSE | −5.27 (1.55) | −5.84 (1.53) | −5.55 (1.57) | --- | --- |
| Average sphere | −5.16 (1.55) | −5.30 (1.51) | −5.23 (1.54) | --- | --- |
| Average cylinder | −0.22 (0.22) | −1.10 (0.62) | −0.63 (0.63) | --- | --- |
| Outcomes | Preoperative | 3 Months | 12 Months | >1 Year (Range: 18 mo–3 yr) |
|---|---|---|---|---|
| CDVA (LogMAR) | n = 383 | n = 309 | n = 211 | n = 26 |
| Mean (SD) | −0.007 (0.027) | −0.015 (0.042) | −0.022 (0.046) | 0.015 (0.087) |
| Range (Min, Max) | −0.14, 0.04 | −0.14, 0.18 | −0.14, 0.06 | −0.02, 0.44 |
| UDVA (LogMAR) | n = 376 * | n = 299 | n = 207 | n = 30 |
| Mean (SD) | 1.43 (0.24) | 0.026 (0.099) | 0.025 (0.091) | 0.08 (0.134) |
| Range (Min, Max) | 0.1, 1.7 | −0.14, 0.8 | −0.14, 0.54 | 0, 0.54 |
| Sphere | n = 405 | n = 309 | n = 211 | n = 27 |
| Mean (SD) | −5.23 (1.54) | 0.088 (0.486) | 0.075 (0.447) | −0.120 (0.487) |
| Range (Min, Max) | −10.75, −1.5 | −2, 1.5 | −1.5, 2.25 | −1.0, 0.75 |
| Cylinder | n = 405 | n = 309 | n = 211 | n = 27 |
| Mean (SD) | −0.621 (0.606) | −0.375 (0.334) | −0.400 (0.326) | −0.417 (0.277) |
| Range (Min, Max) | −3.25, 0 | −2, 0.5 | −1.75, 0 | −1, 0 |
| ≤0.50 D (%) | --- | 83.80% | 78.60% | 81.40% |
| ≤1.00 D (%) | --- | 97.40% | 97.10% | 100% |
| MSE | n = 405 | n = 309 | n = 211 | n = 27 |
| Mean (SD) | −5.54 (1.57) | −0.099 (0.489) | −0.127 (0.451) | −0.329 (0.460) |
| Range (Min, Max) | −11.125, −1.5 | −2.125, 1.25 | −1.75, 1.875 | −1.25, 0.625 |
| ±0.50 D of Intended (%) | --- | 84.10% | 84.80% | 77.80% |
| ±1.00 D of Intended (%) | --- | 94.80% | 95.20% | 96.30% |
| Efficacy Index ** | --- | 0.944 (0.182) | 0.939 (0.171) | 0.834 (0.174) |
| Safety Index *** | --- | 1.037 (0.124) | 1.026 (0.123) | 0.979 (0.091) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Payne, C.J.; Webster, C.R.; Moshirfar, M.; Handlon, J.J.; Ronquillo, Y.C.; Hoopes, P.C. One-Year Visual Outcomes and Corneal Higher-Order Aberration Assessment of Small-Incision Lenticule Extraction for the Treatment of Myopia and Myopic Astigmatism. J. Clin. Med. 2022, 11, 6294. https://doi.org/10.3390/jcm11216294
Payne CJ, Webster CR, Moshirfar M, Handlon JJ, Ronquillo YC, Hoopes PC. One-Year Visual Outcomes and Corneal Higher-Order Aberration Assessment of Small-Incision Lenticule Extraction for the Treatment of Myopia and Myopic Astigmatism. Journal of Clinical Medicine. 2022; 11(21):6294. https://doi.org/10.3390/jcm11216294
Chicago/Turabian StylePayne, Carter J., Courtney R. Webster, Majid Moshirfar, Jaiden J. Handlon, Yasmyne C. Ronquillo, and Phillip C. Hoopes. 2022. "One-Year Visual Outcomes and Corneal Higher-Order Aberration Assessment of Small-Incision Lenticule Extraction for the Treatment of Myopia and Myopic Astigmatism" Journal of Clinical Medicine 11, no. 21: 6294. https://doi.org/10.3390/jcm11216294