
Microscopic Hematuria at Kidney Donor Screening and Post-Donation Kidney Outcomes
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
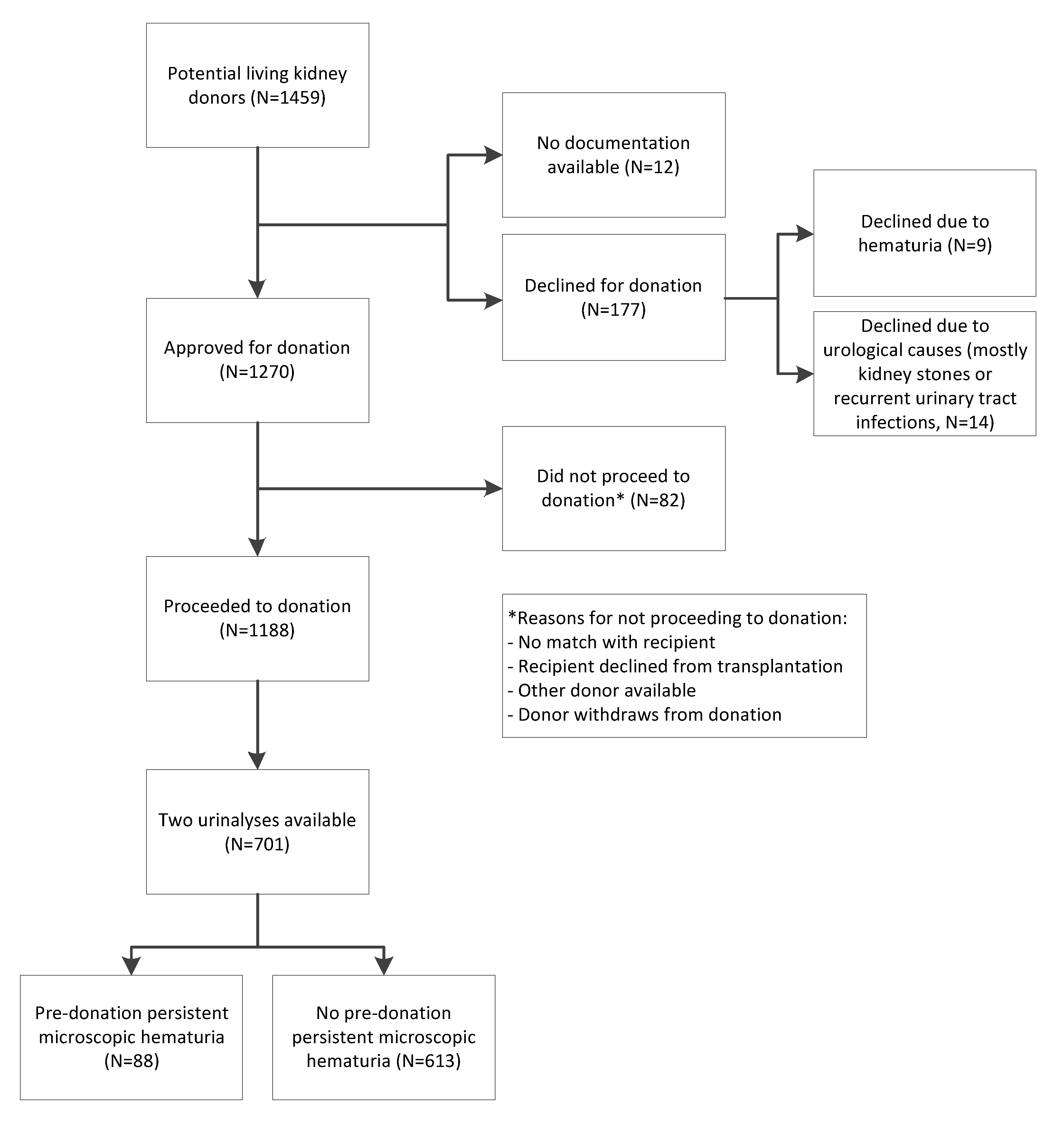
2.1. Study Population
2.2. Urinalyses and Definition of Microscopic Hematuria
2.3. Post-Donation Outcomes
2.4. Statistical Analyses
3. Results
3.1. Pre-Donation Characteristics of the Living Kidney Donor Population
3.2. Post-Donation Outcomes
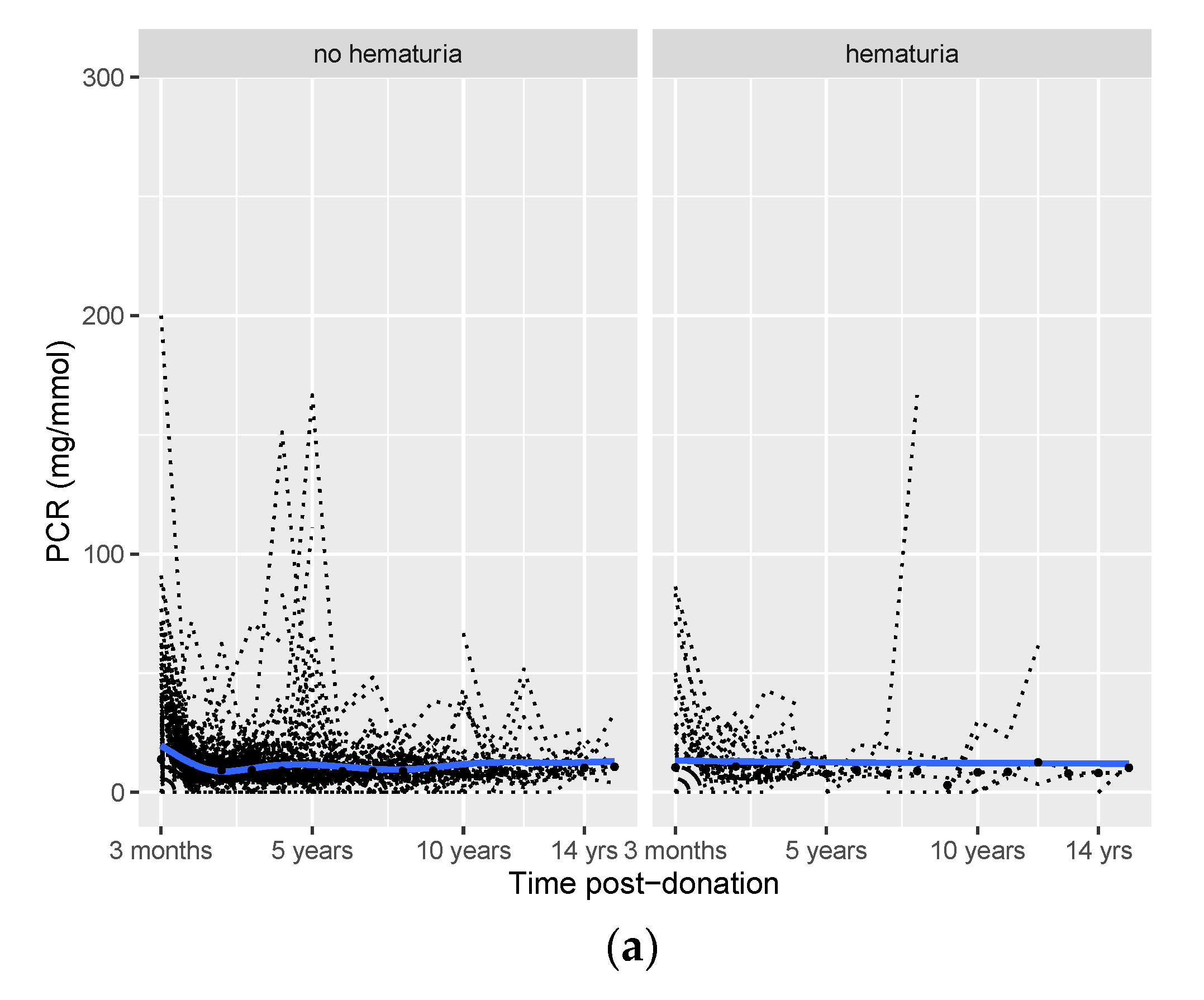
3.3. Effect of Hematuria on Long-Term Post-Donation Proteinuria, SBP, and eGFR Course
3.4. Sensitivity Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohr, D.; Kenneth, P.; Offord, M.; Owen, R.; Melton, J. Asymptomatic Microhematuria and Urologic Disease: A Population-Based Study. JAMA 1986, 256, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Brown, R. Microscopic Hematuria. N. Engl. J. Med. 2003, 349, 1292–1293. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.A.; Lisa, B. British Transplantation Society/Renal Association UK guidelines for living donor kidney transplantation 2018: Summary of updated guidance. Transplantation 2018, 102, e307. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.; Kasiske, B.; Levey, A.; Adams, P.; Alberú, J.; Bakr, M.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101, S1–S109. [Google Scholar] [CrossRef] [Green Version]
- Vadivel, N.; Stankovic, A.; Rennke, H.G.; Singh, A.K. Accepting prospective kidney donors with asymptomatic urinary abnormalities: Are we shooting in the dark? Kidney Int. 2007, 71, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Savige, J.; Rana, K.; Tonna, S.; Ruzza, M.; Dagher, H.; Wang, Y. Thin Basement Membrane Nephropathy. Kidney Int. 2003, 64, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Gross, O.; Weber, M.; Fries, J.W.U.; Müller, G.A. Living donor kidney transplantation from relatives with mild urinary abnormalities in Alport syndrome: Long-term risk, benefit and outcome. Nephrol. Dial. Transplant. 2009, 24, 1626–1630. [Google Scholar] [CrossRef] [Green Version]
- Hall, C.; Bradley, R.; Kerr, A.; Attoti, R.; Peat, D. Clinical value of renal biopsy in patients with asymptomatic microscopic hematuria with and without low-grade proteinuria. Clin. Nephrol. 2004, 62, 267–272. [Google Scholar] [CrossRef]
- McGregor, D.; Lynn, K.; Bailey, R.; Robson, R.; Gardner, J. Clinical audit of the use of renal biopsy in the management of isolated microscopic hematuria. Clin. Nephrol. 1998, 49, 345–348. [Google Scholar]
- Kido, R.; Shibagaki, Y.; Iwadoh, K.; Nakajima, I.; Fuchinoue, S.; Fujita, T.; Teraoka, S. Persistent glomerular hematuria in living kidney donors confers a risk of progressive kidney disease in donors after heminephrectomy. Am. J. Transplant. 2010, 10, 1597–1604. [Google Scholar] [CrossRef]
- Koushik, R.; Garvey, C.; Manivel, J.C.; Matas, A.J.; Kasiske, B.L. Persistent, asymptomatic, microscopic hematuria in prospective kidney donors. Transplantation 2005, 80, 1425–1429. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.R.; Sun, I.O.; Hong, Y.A.; Kim, H.G.; Park, H.S.; Chung, B.H.; Choi, B.S.; Park, C.W.; Kim, Y.S.; Yang, C.W. The role of kidney biopsy to determine donation from prospective kidney donors with asymptomatic urinary abnormalities. Transplant. Proc. 2012, 44, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Hassan, E.A.; Ali, T.Z.; Abdulbaki, A.; Ibrahim, I.A.; Almanae, H.M.; Aleid, H.A. Histopathologic Findings of Potential Kidney Donors With Asymptomatic Microscopic Hematuria: Impact on Donation. Transplant. Proc. 2017, 49, 1729–1732. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H.; Hsu, C.; Vitiinghoff, E.; Lin, F.; Bansal, N. Comparison of Associations of Urine Protein-Creatinine Ratio Versus Albumin-Creatinine Ratio With Complications of CKD: A Cross-sectional Analysis. Am. J. Kidney Dis. 2013, 62, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Van Londen, M.; Aarts, B.M.; Deetman, P.E.; van der Weijden, J.; Eisenga, M.F.; Navis, G.; Bakker, S.J.; de Borst, M.H.; van Londen, M.; on behalf of the NIGRAM Consortium. Post-transplant hypophosphatemia and the risk of death-censored graft failure and mortality after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2017, 12, 1301–1310. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Annals of Internal Medicine Article Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular. Ann. Intern. Med. 2014, 145, 247–254. [Google Scholar] [CrossRef]
- Vivante, A.; Afek, A.; Frenkel-Nir, Y.; Tzur, D.; Farfel, A.; Golan, E.; Chaiter, Y.; Shohat, T.; Skorecki, K.; Calderon-Margalit, R. Persistent asymptomatic isolated microscopic hematuria in Israeli adolescents and young adults and risk for end-stage renal disease. JAMA-J. Am. Med. Assoc. 2011, 306, 729–736. [Google Scholar] [CrossRef] [Green Version]
- Niertransplantatie, L.O.; van der Heide, J.H. Nederlandse Richtlijn: Evaluatie Van Potentiële Donoren Voor Levende Donor Niertransplantatie; NTV: Haarlem, The Netherlands, 2008; pp. 23–27. [Google Scholar]
- Lam, N.N.; Lloyd, A.; Lentine, K.L.; Quinn, R.R.; Ravani, P.; Hemmelgarn, B.R.; Klarenbach, S.; Garg, A.X. Changes in kidney function follow living donor nephrectomy. Kidney Int. 2020, 98, 176–186. [Google Scholar] [CrossRef]
- Matas, A.J.; Vock, D.M.; Ibrahim, H.N. GFR ≤ 25 years postdonation in living kidney donors with (vs. without) a first-degree relative with ESRD. Am. J. Transplant. 2018, 18, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Choi, C.; Ahn, S.; Min, S.K.; Ha, J.; Ahn, C.; Kim, Y.; Lee, H.; Min, S.I. Midterm outcome of kidney transplantation from donors with thin basement membrane nephropathy. Transplantation 2018, 102, E180–E184. [Google Scholar] [CrossRef]
- D’Amico, G. Natural history of idiopathic IgA nephropathy: Role of clinical and histological prognostic factors. Am. J. Kidney Dis. 2000, 36, 227–237. [Google Scholar] [CrossRef]
- Nieuwhof, C.; Doorenbos, C.; Grave, W.; de Heer, F.; de Leeuw, P.; Zeppenfeldt, E.; van Breda Vriesman, P.J. A prospective study of the natural history of idiopathic non-proteinuric hematuria. Kidney Int. 1996, 49, 222–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Haan, A.; Eijgelsheim, M.; Vogt, L.; Knoers, N.V.A.M. Diagnostic Yield of Next-Generation Sequencing in Patients with Chronic Kidney Disease of Unknown Etiology. Front. Genet. 2019, 10, 1264. [Google Scholar] [CrossRef] [PubMed]
- Waterman, A.D.; Dew, M.A.; Davis, C.L.; McCabe, M.; Wainright, J.L.; Forland, C.L.; Bolton, L.; Cooper, M. Living-donor follow-up attitudes and practices in U.S. kidney and liver donor programs. Transplantation 2013, 95, 883–888. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Microscopic Hematuria | |||
|---|---|---|---|
| Total (n = 701) | Present (n = 88) | Absent (n = 613) | |
| Female sex, n (%) | 345 (49) | 70 (80) | 275 (45) c |
| Caucasian race, n (%) | 701 (100) | 88 (100) | 613 (100) |
| Living related donations, n (%) | 328 (47) | 38 (43) | 290 (47) |
| Age, years | 52 (11) | 54 (11) | 52 (11) |
| Weight, kg | 81 (14) | 77 (13) | 81 (14) c |
| Height, cm | 175 (9) | 171 (9) | 175 (9) b |
| BMI, kg/m2 | 26 (4) | 26 (3) | 26 (4) |
| BSA, m2 | 1.96 (0.20) | 1.89 (0.18) | 1.96 (0.20) b |
| SBP, mmHg | 127 (13) | 125 (11) | 127 (13) |
| DBP, mmHg | 76 (9) | 75 (9) | 76 (9) |
| Hypertension a, n (%) | 183 (26) | 23 (26) | 160 (26) |
| Use of antihypertensive medication, n (%) | 51 (7) | 5 (6) | 46 (8) |
| mGFR, mL/min | 115 (22) | 111 (22) | 115 (22) b |
| mGFRBSA, mL/min/1.73 m2 | 102 (16) | 101 (16) | 102 (16) |
| eGFR, ml/min/1.73 m2 | 88 (14) | 88 (14) | 89 (14) |
| Serum creatinine, µmol/L | 78 (14) | 72 (11) | 78 (14)c |
| Serum glucose, mmol/L | 5.3 (0.6) | 5.3 (0.5) | 5.3 (0.6) |
| HbA1C, % | 5.5 (0.4) | 5.5 (0.3) | 5.5 (0.4) |
| Diabetes, n (%) | 6 (1) | 1 (1) | 5 (1) |
| Serum cholesterol, mmol/L LDL HDL Triglycerides | 5.3 (1.0) 3.5 (0.9) 1.6 (0.5) 1.4 (0.9) | 5.3 (1.0) 3.4 (1.1) 1.7 (0.5) 1.2 (0.8) | 5.4 (1.0) 3.5 (0.9) 1.5 (0.5) 1.4 (0.9) b |
| Serum urea, mmol/L | 5.4 (1.3) | 5.3 (1.2) | 5.5 (1.3) |
| Serum potassium, mmol/L | 3.9 (0.3) | 3.9 (0.3) | 3.9 (0.3) |
| Serum sodium, mmol/L | 141 (3) | 141 (3) | 141 (3) b |
| Sodium excretion, mmol/24 h | 195 (73) | 172 (66) | 199 (73) b |
| PCR, mg/mmol | 5 (0–12) | 9 (0–15) | 0 (0–12) |
| erythrocytes per µL | n.a. | 10 (6–22) | n.a. |
| Outcome PCR | Outcome eGFR | Outcome SBP | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | P | Estimate | 95% CI | P | Estimate | 95% CI | P | |
| Hematuria a | 0.28 | −0.01 to 0.56 | 0.05 | −1.17 | −3.66 to 1.32 | 0.36 | 1.18 | −1.86 to 4.22 | 0.45 |
| Time | 0.04 | 0.03 to 0.05 | <0.001 | 0.34 | 0.23 to 0.44 | <0.001 | 0.92 | 0.75 to 1.09 | <0.001 |
| Hematuria×time | −0.02 | −0.08 to 0.03 | 0.38 | 0.10 | −0.34 to 0.54 | 0.65 | 0.50 | −0.21 to 1.21 | 0.17 |
| Outcome PCR | Outcome eGFR | Outcome SBP | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | P | Estimate | 95% CI | P | Estimate | 95% CI | P | |
| Hematuria a | 0.22 | −0.19 to 0.64 | 0.30 | −2.64 | −6.14 to 0.87 | 0.14 | 1.74 | −2.45 to 5.92 | 0.42 |
| Time | 0.05 | 0.03 to 0.06 | <0.001 | 0.24 | 0.10 to 0.38 | 0.001 | 0.80 | 0.58 to 1.02 | <0.001 |
| Hematuria×time | −0.02 | −0.10 to 0.06 | 0.66 | 0.41 | −0.18 to 0.99 | 0.17 | 0.002 | −0.89 to 0.90 | 0.996 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| St. β | 95% CI | P | St. β | 95% CI | P | |
| Age, years | −0.52 | −0.64 to −0.45 | <0.001 | - | - | - |
| Sex, 1 = female | −0.10 | −0.21 to 0.01 | 0.07 | 0.01 | −0.12 to 0.13 | 0.93 |
| BMI, kg/m2 | −0.01 | −0.12 to 0.09 | 0.80 | - | - | - |
| BSA, m2 | 0.07 | −0.04 to 0.16 | 0.22 | 0.01 | −0.11 to 0.12 | 0.93 |
| eGFR, mL/min/1.73 m2 | 0.59 | 0.51 to 0.68 | <0.001 | 0.59 | 0.50 to 0.38 | <0.001 |
| SBP, mmHg | −0.08 | −0.19 to 0.02 | 0.13 | −0.03 | −0.12 to 0.06 | 0.50 |
| HbA1c, % | −0.08 | −0.19 to 0.04 | 0.19 | −0.09 | −0.19 to 0.01 | 0.07 |
| ln(PCR), mg/mmol | −0.07 | −0.27 to 0.13 | 0.49 | - | - | - |
| Hematuria, 1 = positive | −0.05 | −0.17 to 0.07 | 0.40 | −0.06 | −0.16 to 0.04 | 0.23 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | |
| Outcome PCR group | ||||||
| Hematuria, 1 = positive | 0.71 | 0.35 to 0.43 | 0.34 | 0.49 | 0.16 to 1.51 | 0.22 |
| Age | 1.00 | 0.98 to 1.02 | 0.72 | 0.99 | 0.96 to 1.02 | 0.62 |
| Female sex | 0.85 | 0.56 to 1.31 | 0.46 | 0.91 | 0.42 to 1.97 | 0.81 |
| Pre-donation PCR | 1.03 | 0.53 to 2.00 | 0.93 | 1.11 | 0.53 to 2.34 | 0.78 |
| Outcome eGFR group | ||||||
| Hematuria, 1 = positive | 1.23 | 0.50 to 3.03 | 0.65 | 1.45 | 0.56 to 3.72 | 0.44 |
| Age | 0.98 | 0.95 to 1.01 | 0.10 | 0.96 | 0.93 to 0.99 | 0.01 |
| Female sex | 0.84 | 0.44 to 1.59 | 0.58 | 0.73 | 0.37 to 1.45 | 0.37 |
| Pre-donation eGFR | 0.98 | 0.96 to 1.00 | 0.11 | 0.97 | 0.94 to 0.99 | 0.01 |
| Outcome SBP group | ||||||
| Hematuria, 1 = positive | 0.65 | 0.41 to 1.04 | 0.07 | 0.63 | 0.37 to 1.05 | 0.07 |
| Age | 1.00 | 0.98 to 1.01 | 0.62 | 1.02 | 1.00 to 1.04 | 0.02 |
| Female sex | 0.95 | 0.70 to 1.28 | 0.72 | 0.69 | 0.49 to 0.97 | 0.03 |
| Pre-donation SBP | 0.94 | 0.92 to 0.95 | <0.001 | 0.93 | 0.92 to 0.95 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Weijden, J.; van Londen, M.; Pol, R.A.; Sanders, J.-S.F.; Navis, G.; Nolte, I.M.; de Borst, M.H.; Berger, S.P. Microscopic Hematuria at Kidney Donor Screening and Post-Donation Kidney Outcomes. J. Clin. Med. 2022, 11, 6281. https://doi.org/10.3390/jcm11216281
van der Weijden J, van Londen M, Pol RA, Sanders J-SF, Navis G, Nolte IM, de Borst MH, Berger SP. Microscopic Hematuria at Kidney Donor Screening and Post-Donation Kidney Outcomes. Journal of Clinical Medicine. 2022; 11(21):6281. https://doi.org/10.3390/jcm11216281
Chicago/Turabian Stylevan der Weijden, Jessica, Marco van Londen, Robert A. Pol, Jan-Stephan F. Sanders, Gerjan Navis, Ilja M. Nolte, Martin H. de Borst, and Stefan P. Berger. 2022. "Microscopic Hematuria at Kidney Donor Screening and Post-Donation Kidney Outcomes" Journal of Clinical Medicine 11, no. 21: 6281. https://doi.org/10.3390/jcm11216281