
Effects of Meditation on Cardiovascular and Muscular Responses in Patients during Cardiac Rehabilitation: A Randomized Pilot Study

 ,
,  and
and
Abstract
:1. Introduction
2. Objectives
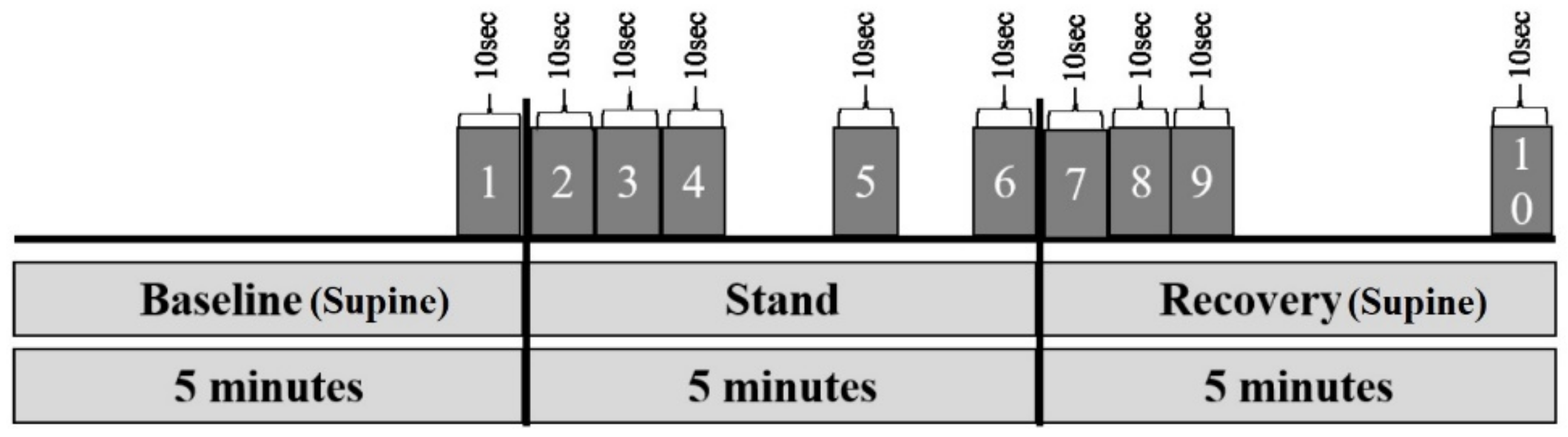
3. Materials and Methods
4. Results
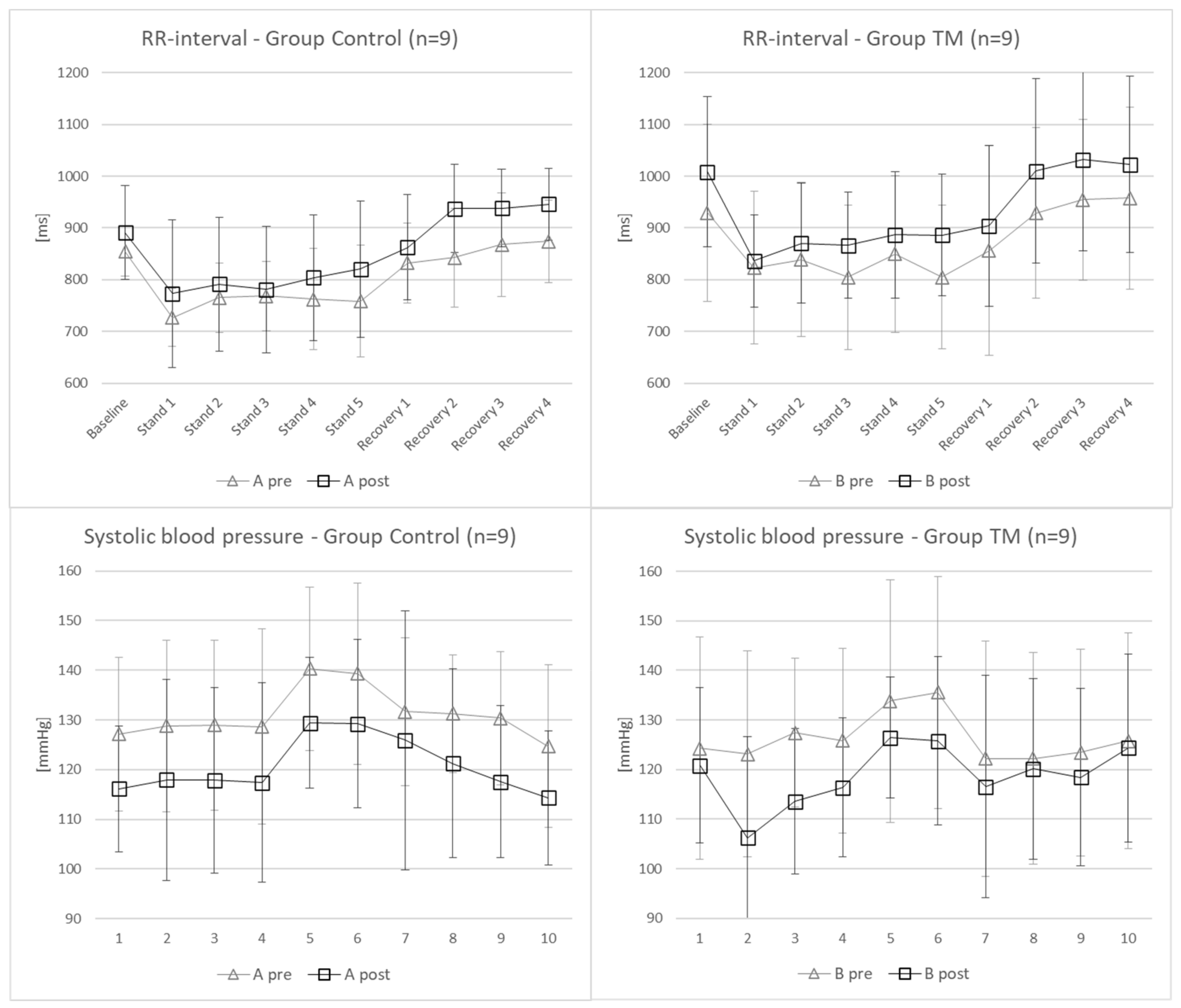
4.1. Cardiovascular Parameters
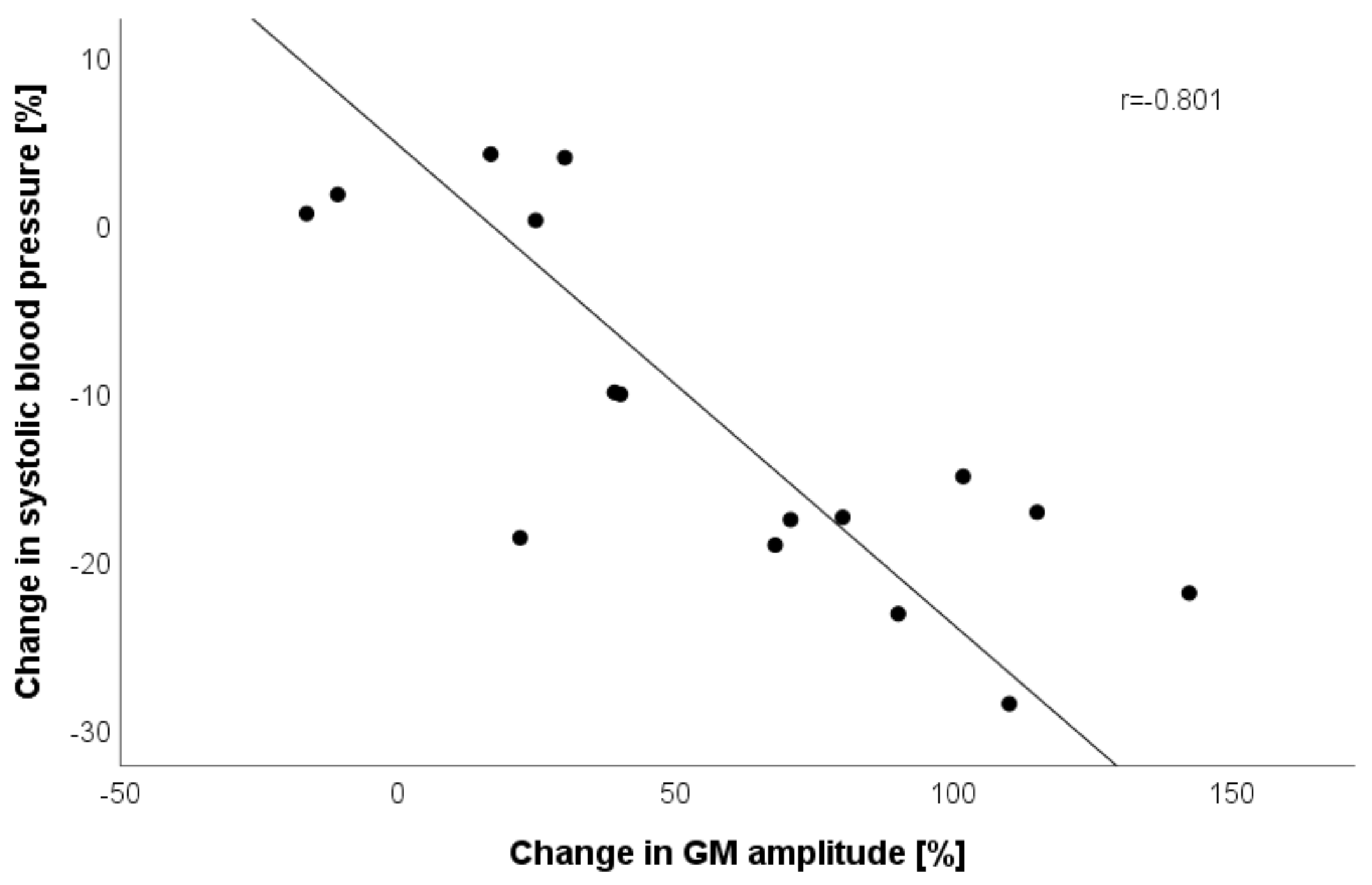
4.2. Tensiomyographic Parameters
5. Discussion
5.1. Limitations
5.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs) Key Facts What Are the Risk Factors for Cardiovascular Disease? World Health Organization: Geneva, Switzerland, 2017; pp. 1–6. [Google Scholar]
- Stampfer, M.J.; Hu, F.B.; Manson, J.E.; Rimm, E.B.; Willett, W.C. Primary prevention of coronary heart disease in women through diet and lifestyle. N. Engl. J. Med. 2000, 343, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Pignalberi, C.; Patti, G.; Chimenti, C.; Pasceri, V.; Maseri, A. Role of different determinants of psychological distress in acute coronary syndromes. J. Am. Coll. Cardiol. 1998, 32, 613–619. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, C.V.S.; Lima, M.G.; Ladeia, A.M. Meditation, Health and Scientific Investigations: Review of the Literature. J. Relig. Health 2017, 56, 411–427. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Lange, R.A.; Bairey-Merz, C.N.; Davidson, R.J.; Jamerson, K.; Mehta, P.K.; Michos, E.D.; Norris, K.; Ray, I.B.; Saban, K.L.; et al. Meditation and Cardiovascular Risk Reduction: A Scientific Statement from the American Heart Association. J. Am. Heart Assoc. 2017, 6, e002218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walton, K.G.; Schneider, R.H.; Salerno, J.W.; Nidich, S.I. Psychosocial stress and cardiovascular disease part 3: Clinical and policy implications of research on the Transcendental Meditation program. Behav. Med. 2005, 30, 173–184. [Google Scholar] [CrossRef]
- Barnes, V.A.; Orme-Johnson, D.W. Prevention and Treatment of Cardiovascular Disease in Adolescents and Adults through the Transcendental Meditation® Program: A Research Review Update. Curr. Hypertens. Rev. 2012, 8, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Rainforth, M.V.; Schneider, R.H.; Nidich, S.I.; Gaylord-King, C.; Salerno, J.W.; Anderson, J.W. Stress reduction programs in patients with elevated blood pressure: A systematic review and meta-analysis. Curr. Hypertens. Rep. 2007, 9, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Benson, H.; Wallace, R. Decreased blood pressure in hypertensive subjects who practiced meditation. Circulation 1972, 516, 45–46. [Google Scholar] [CrossRef]
- Blackwell, B.; Hanenson, I.B.; Bloomfield, S.; Magenheim, H.G. Effects of Transcendental Meditation on blood pressure: A controlled pilot experiment. Psychosom. Med. 1975, 37, 86. [Google Scholar]
- Agarwal, B.; Kharbanda, A. Effect of transcendental meditation on mild and moderate hypertension. J. Assoc. Physicians India 1981, 29, 591–596. [Google Scholar]
- Schneider, R.; Staggers, F.; Alexander, C.; Al, E. A randomized controlled trial of stress reduction for hypertension in older African Americans. Hypertension 1995, 26, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Schneider, R.; Staggers, F.; Sheppard, W.; Clayborne, B.; Rainforth, M.; Salerno, J.; Kondwani, K.; Smith, S.; Walton, K.; et al. Trial of stress reduction for hypertension in older African Americans. II. Sex and risk subgroup analysis. Hypertension 1996, 28, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Walton, K.G.; Schneider, R.H.; Nidich, S.I.; Salemo, J.W.; Nordstrom, C.K.; Merz, C.N.B. Psychosocial stress and cardiovascular disease part 2: Effectiveness of the transcendental meditation program in treatment and prevention. Behav. Med. 2002, 28, 106–123. [Google Scholar] [CrossRef] [Green Version]
- Barnes, V.A.; Kapuku, G.K.; Treiber, F.A. Impact of transcendental meditation on left ventricular mass in African American adolescents. Evid.-Based Complement. Altern. Med. 2012, 2012, 923153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, R.; Myers, H.; Marwaha, K.; Rainforth, M.; Salerno, J.; Nidich, S.; Gaylord-King, C.; Alexander, C.; Norris, K. Stress Reduction in the Prevention of Left Ventricular Hypertrophy: A Randomized Controlled Trial of Transcendental Meditation and Health Education in Hypertensive African Americans. Ethn. Dis. 2019, 29, 5577–5586. [Google Scholar] [CrossRef] [Green Version]
- Zamarra, J.; Schneider, R.; Besseghini, I.; Robinson, D.; Salerno, J. Usefulness of the transcendental meditation program in the treatment of patients with coronary artery disease. Am. J. Cardiol. 1995, 77, 867–870. [Google Scholar] [CrossRef]
- Castillo-Richmond, A.; Schneider, R.H.; Alexander, C.N.; Cook, R.; Myers, H.; Nidich, S.; Haney, C.; Rainforth, M.; Salerno, J. Effects of stress reduction on carotid atherosclerosis in hypertensive African Americans. Stroke 2000, 31, 568–573. [Google Scholar] [CrossRef]
- Dillbeck, M.C.; Orme-Johnson, D.W. Physiological differences between transcendental meditation and rest. Am. Psychol. 1987, 42, 879–881. [Google Scholar] [CrossRef]
- Alexander, C.N.; Swanson, G.C.; Rainforth, M.V.; Carlisle, T.W.; Todd, C.C.; Oates, R.M. Effects of the transcendental meditation program on stress reduction, health, and employee development: A prospective study in two occupational settings. Anxiety Stress Coping 1993, 6, 245–262. [Google Scholar] [CrossRef]
- Gaylord, C.; Orme-Johnson, D.; Travis, F. The effects of the Transcendental Meditation technique and progressive muscle relaxation on EEG coherence, stress reactivity, and mental health in black adults. Int. J. Neurosci. 1989, 46, 77–86. [Google Scholar] [CrossRef] [PubMed]
- MacLean, C.; Walton, K.; Wenneberg, S.; Levitsky, D.; Mandarino, J.; Waziri, R.; Hillis, S.; Schneider, R. Effects of the Transcendental Meditation program on adaptive mechanisms: Changes in hormone levels and responses to stress after 4 months of practice. Psychoneuroendocrinology 1997, 22, 277–295. [Google Scholar] [CrossRef]
- Alexander, C.N.; Robinson, P.; Rainforth, M. Treating and Preventing Alcohol, Nicotine, and Drug Abuse Through Transcendental Meditation: A review and statistical meta-analysis. Alcohol. Treat. Q. 1994, 11, 13–87. [Google Scholar] [CrossRef]
- Royer, A. The role of the Transcendental Meditation Technique in promoting smoking cessation. Alcohol. Treat. Q. 1994, 11, 221–239. [Google Scholar] [CrossRef]
- Orme-Johnson, D. Medical care utilization and the transcendental meditation program. Psychosom. Med. 1987, 49, 493–507. [Google Scholar] [CrossRef] [Green Version]
- Schneider, R.; Nidich, S.; Kotchen, J.M.; Kotchen, T.; Grim, C.; Rainforth, M.; King, C.G.; Salerno, J. Effects of stress reduction on clinical events in African Americans with coronary heart disease: A randomized clinical trial. Circulation 2009, 120, 461. [Google Scholar]
- Alexander, C.; Barnes, V.; Schneider, R.; Langer, E.; Newman, R.; Chandler, H.; Davies, J.; Rainforth, M. A randomized controlled trial of stress reduction on cardiovascular and all-cause mortality in the elderly: Results of 8 year and 15 year follow-ups. Circulation 1996, 93, 629. [Google Scholar]
- Schneider, R.H.; Alexander, C.N.; Staggers, F.; Rainforth, M.; Salerno, J.W.; Hartz, A.; Arndt, S.; Barnes, V.A.; Nidich, S.I. Long-term effects of stress reduction on mortality in persons ≥ 55 years of age with systemic hypertension. Am. J. Cardiol. 2005, 95, 1060–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Lyles, R.H.; Bauer-Wu, S. Mindfulness meditation lowers muscle sympathetic nerve activity and blood pressure in African-American males with chronic kidney disease. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2014, 307, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Hernelahti, M.; Tikkanen, H.O.; Karjalainen, J.; Kujala, U.M. Muscle fiber-type distribution as a predictor of blood pressure: A 19-year follow-up study. Hypertension 2005, 45, 1019–1023. [Google Scholar] [CrossRef] [Green Version]
- Houmard, J.A.; Weidner, M.L.; Koves, T.R.; Hickner, R.C.; Cortright, R.L. Association between muscle fiber composition and blood pressure levels during exercise in men. Am. J. Hypertens. 2000, 13, 586–592. [Google Scholar] [CrossRef] [Green Version]
- Šimunič, B.; Pišot, R.; Rittweger, J.; Degens, H. Age-related slowing of contractile properties differs between power, endurance, and nonathletes: A tensiomyographic assessment. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2018, 73, 1602–1608. [Google Scholar] [CrossRef]
- Brix, B.; White, O.; Ure, C.; Apich, G.; Simon, P.; Roessler, A.; Goswami, N. Hemodynamic responses in lower limb lymphedema patients undergoing physical therapy. Biology 2021, 10, 642. [Google Scholar] [CrossRef]
- Bokhari, S.; Schneider, R.H.; Salerno, J.W.; Rainforth, M.V.; Gaylord-King, C.; Nidich, S.I. Effects of cardiac rehabilitation with and without meditation on myocardial blood flow using quantitative positron emission tomography: A pilot study. J. Nucl. Cardiol. 2019, 28, 1596–1607. [Google Scholar] [CrossRef]
- Gould, K.L.; Johnson, N.P.; Bateman, T.M.; Beanlands, R.S.; Bengel, F.M.; Bober, R.; Camici, P.G.; Cerqueira, M.D.; Chow, B.J.W.; Di Carli, M.F.; et al. Anatomic versus physiologic assessment of coronary artery disease: Role of coronary flow reserve, fractional flow reserve, and positron emission tomography imaging in revascularization decision-making. J. Am. Coll. Cardiol. 2013, 62, 1639–1653. [Google Scholar] [CrossRef] [Green Version]
- Schindler, T.H.; Zhang, X.L.; Vincenti, G.; Mhiri, L.; Lerch, R.; Schelbert, H.R. Role of PET in the evaluation and understanding of coronary physiology. J. Nucl. Cardiol. 2007, 14, 589–603. [Google Scholar] [CrossRef] [Green Version]
- Klocke, F.J.; Baird, M.G.; Lorell, B.H.; Bateman, T.M.; Messer, J.V.; Berman, D.S.; O’Gara, P.T.; Carabello, B.A.; Russell, R.O.; Cerqueira, M.D.; et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidel. Circulation 2003, 108, 1404–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simunič, B.; Degens, H.; Rittweger, J.; Narici, M.; Mekjavić, I.B.; Pišot, R. Noninvasive estimation of myosin heavy chain composition in human skeletal muscle. Med. Sci. Sports Exerc. 2011, 43, 1619–1625. [Google Scholar] [CrossRef] [Green Version]
- Šimunič, B.; Koren, K.; Rittweger, J.; Lazzer, S.; Reggiani, C.; Rejc, E.; Pišot, R.; Narici, M.; Degens, H. Tensiomyography detects early hallmarks of bed-rest-induced atrophy before changes in muscle architecture. J. Appl. Physiol. 2019, 126, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Pišot, R.; Narici, M.V.; Šimunič, B.; De Boer, M.; Seynnes, O.; Jurdana, M.; Biolo, G.; Mekjavič, I.B. Whole muscle contractile parameters and thickness loss during 35-day bed rest. Eur. J. Appl. Physiol. 2008, 104, 409–414. [Google Scholar] [CrossRef]
- Juhlin-Dannfelt, A.; Frisk-Holmberg, M.; Karlsson, J.; Tesch, P. Central and Peripheral Circulation in Relation to Muscle-Fibre Composition in Normo- and Hyper-Tensive Man. Clin. Sci. 1979, 56, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P. Capillary density in skeletal muscle of man. Acta Physiol. Scand. 1975, 95, 203–205. [Google Scholar] [CrossRef]
- Duscha, B.D.; Kraus, W.E.; Keteyian, S.J.; Sullivan, M.J.; Green, H.J.; Schachat, F.H.; Pippen, A.M.; Brawner, C.A.; Blank, J.M.; Annex, B.H. Capillary density of skeletal muscle: A contributing mechanism for exercise intolerance in class II-III chronic heart failure independent of other peripheral alterations. J. Am. Coll. Cardiol. 1999, 33, 1956–1963. [Google Scholar] [CrossRef] [Green Version]
- Boulé, N.G.; Kenny, G.P.; Haddad, E.; Wells, G.A.; Sigal, R.J. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in Type 2 diabetes mellitus. Diabetologia 2003, 46, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Nishitani, M.; Shimada, K.; Masaki, M.; Sunayama, S.; Kume, A.; Fukao, K.; Sai, E.; Onishi, T.; Shioya, M.; Sato, H.; et al. Effect of cardiac rehabilitation on muscle mass, muscle strength, and exercise tolerance in diabetic patients after coronary artery bypass grafting. J. Cardiol. 2013, 61, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- France, C.R.; France, J.L.; Patterson, S.M. Blood pressure and cerebral oxygenation responses to skeletal muscle tension: A comparison of two physical maneuvers to prevent vasovagal reactions. Clin. Physiol. Funct. Imaging 2006, 26, 21–25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Control Group | TM Group | Total Sample |
|---|---|---|---|
| Male (n) | 8 (89%) | 8 (89%) | 16 (89%) |
| Female (n) | 1 (11%) | 1 (11%) | 2 (11%) |
| Age (years) | 58.56 (±7.86) | 59.78 (±7.84) | 59.17 (±7.45) |
| Height (cm) | 177.22 (±7.26) | 173.44 (±7.73) | 175.33 (±7.53) |
| Weight (kg) | 95.44 (±10.41) | 79.56 (±19.22) | 87.50(±17.08) |
| BMI (kg/m2) | 30.52 (±4.12) | 26.31 (±5.10) | 28.42 (±4.99) |
| Values are mean (±SD) | |||
| Cause of Cardiac Rehabilitation | |||
| MI | 4 (44%) | 3 (33%) | 7 (39%) |
| ACS | 1 (12%) | 1 (12%) | 2 (11%) |
| PCI | 2 (22%) | 2 (22%) | 4 (22%) |
| CABG | 2 (22%) | 3 (33%) | 5 (28%) |
| Results Group Control & Group TM: Pre-Post | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Epochs | p-Value: | p-Value: | |||||||||||
| Parameter | Group | Baseline | Stand 1 | Stand 2 | Stand 3 | Stand 4 | Stand 5 | Recovery 1 | Recovery 2 | Recovery 3 | Recovery 4 | Pre-Post | Pre-Post × Group |
| Heart rate [bpm] | Control pre (n = 9) | 71 (±5) | 84 (±8) | 79 (±7) | 80 (±7) | 80 (±11) | 81 (±12) | 74 (±8) | 73 (±9) | 71 (±9) | 70 (±8) | p = 0.058 | p = 0.900 |
| Control post (n = 9) | 72 (±10) | 81 (±16) | 78 (±13) | 79 (±14) | 77 (±13) | 77 (±15) | 72 (±8) | 65 (±6) | 65 (±6) | 65 (±5) | |||
| TM pre (n = 9) | 69 (±14) | 75 (±14) | 74 (±14) | 78 (±15) | 73 (±13) | 79 (±18) | 77 (±23) | 67 (±12) | 65 (±11) | 65 (±12) | |||
| TM post (n = 9) | 61 (±10) | 74 (±8) | 71 (±9) | 71 (±9) | 70 (±11) | 70 (±10) | 69 (±11) | 61 (±10) | 60 (±10) | 60 (±11) | |||
| RR-interval [ms] | Control pre (n = 9) | 855 (±48) | 727 (±55) | 765 (±67) | 768 (±67) | 762 (±98) | 758 (±108) | 832 (±77) | 843 (±96) | 868 (±100) | 874 (±79) | p = 0.050 | p = 0.836 |
| Control post (n = 9) | 891 (±91) | 773 (±143) | 791 (±129) | 781 (±122) | 804 (±122) | 821 (±132) | 863 (±102) | 937 (±85) | 938 (±75) | 946 (±69) | |||
| TM pre (n = 9) | 930 (±171) | 823 (±147) | 839 (±149) | 805 (±140) | 850 (±152) | 805 (±139) | 856 (±203) | 929 (±165) | 955 (±155) | 958 (±176) | |||
| TM post (n = 9) | 1009 (±146) | 836 (±89) | 870 (±116) | 867 (±102) | 887 (±122) | 886 (±118) | 904 (±156) | 1010 (±179) | 1032 (±177) | 1023 (±171) | |||
| Systolic blood pressure [mmHg] | Control pre (n = 9) | 127 (±15) | 129 (±17) | 129 (±17) | 129 (±20) | 140 (±16) | 139 (±18) | 132 (±15) | 131 (±12) | 130 (±13) | 125 (±16) | p = 0.012 | p = 0.854 |
| Control post (n = 9) | 116 (±13) | 118 (±20) | 118 (±19) | 117 (±20) | 129 (±13) | 129 (±17) | 126 (±26) | 121 (±19) | 118 (±15) | 114 (±14) | |||
| TM pre (n = 9) | 124 (±22) | 123 (±21) | 127 (±15) | 126 (±19) | 134 (±24) | 136 (±23) | 122 (±24) | 122 (±21) | 123 (±21) | 126 (±22) | |||
| TM post (n = 9) | 121 (±16) | 106 (±20) | 114 (±15) | 116 (±14) | 126 (±12) | 126 (±17) | 117 (±22) | 120 (±18) | 118 (±18) | 124 (±19) | |||
| Diastolic blood pressure [mmHg] | Control pre (n = 9) | 81 (±12) | 90 (±13) | 91 (±13) | 91 (±16) | 94 (±8) | 95 (±10) | 75 (±6) | 77 (±8) | 76 (±7) | 80 (±11) | p = 0.433 | p = 0.928 |
| Control post (n = 9) | 76 (±15) | 89 (±15) | 91 (±19) | 93 (±19) | 93 (±23) | 91 (±30) | 76 (±27) | 72 (±20) | 73 (±19) | 75 (±16) | |||
| TM pre (n = 9) | 82 (±15) | 90 (±19) | 93 (±15) | 93 (±18) | 93 (±21) | 95 (±20) | 70 (±11) | 75 (±17) | 76 (±18) | 81 (±18) | |||
| TM post (n = 9) | 80 (±8) | 76 (±9) | 83 (±4) | 85 (±6) | 89 (±7) | 89 (±13) | 73 (±14) | 73 (±10) | 74 (±11) | 79 (±12) | |||
| Mean arterial pressure [mmHg] | Control pre (n = 9) | 100 (±13) | 105 (±14) | 105 (±14) | 105 (±17) | 112 (±11) | 111 (±13) | 96 (±8) | 97 (±8) | 97 (±9) | 98 (±13) | p = 0.088 | p = 0.754 |
| Control post (n = 9) | 92 (±15) | 95 (±23) | 102 (±18) | 104 (±17) | 107 (±19) | 105 (±25) | 94 (±27) | 91 (±20) | 90 (±18) | 91 (±14) | |||
| TM pre (n = 9) | 99 (±19) | 103 (±19) | 106 (±15) | 105 (±19) | 109 (±22) | 111 (±21) | 95 (±23) | 93 (±18) | 94 (±19) | 99 (±18) | |||
| TM post (n = 9) | 97 (±11) | 87 (±12) | 94 (±7) | 97 (±8) | 104 (±8) | 103 (±13) | 89 (±16) | 92 (±12) | 91 (±13) | 97 (±14) | |||
| Stroke index [mL/m2] | Control pre (n = 9) | 31 (±7) | 28 (±4) | 27 (±4) | 27 (±2) | 26 (±4) | 26 (±4) | 37 (±7) | 38 (±7) | 38 (±7) | 32 (±8) | p = 0.797 | p = 0.839 |
| Control post (n = 9) | 32 (±7) | 29 (±4) | 27 (±4) | 26 (±2) | 27 (±4) | 26 (±4) | 35 (±7) | 37 (±7) | 39 (±7) | 34 (±8) | |||
| TM pre (n = 9) | 33 (±4) | 30 (±5) | 32 (±5) | 31 (±4) | 31 (±5) | 31 (±6) | 34 (±4) | 38 (±6) | 39 (±8) | 32 (±6) | |||
| TM post (n = 9) | 35 (±7) | 32 (±4) | 30 (±5) | 30 (±5) | 31 (±5) | 30 (±5) | 36 (±7) | 38 (±8) | 39 (±8) | 35 (±8) | |||
| Cardiac index [l/(±min·m2)] | Control pre (n = 9) | 2.2 (±0.4) | 2.3 (±0.4) | 2.1 (±0.3) | 2.2 (±0.3) | 2.1 (±0.4) | 2.1 (±0.3) | 2.7 (±0.2) | 2.8 (±0.6) | 2.7 (±0.5) | 2.2 (±0.4) | p = 0.217 | p = 0.822 |
| Control post (n = 9) | 2.3 (±0.9) | 2.3 (±0.5) | 2.1 (±0.3) | 2.1 (±0.2) | 2.0 (±0.3) | 2.0 (±0.3) | 2.6 (±0.6) | 2.4 (±0.6) | 2.6 (±0.8) | 2.2 (±0.7) | |||
| TM pre (n = 9) | 2.3 (±0.6) | 2.3 (±0.8) | 2.4 (±0.7) | 2.5 (±0.7) | 2.3 (±0.6) | 2.4 (±0.6) | 2.6 (±0.8) | 2.5 (±0.6) | 2.6 (±0.8) | 2.1 (±0.6) | |||
| TM post (n = 9) | 2.1 (±0.5) | 2.4 (±0.5) | 2.1 (±0.4) | 2.1 (±0.3) | 2.1 (±0.4) | 2.1 (±0.4) | 2.5 (±0.6) | 2.3 (±0.6) | 2.3 (±0.5) | 2.1 (±0.5) | |||
| TPRI [dyne·s·m2/cm5] | Control pre (n = 9) | 3670 (±597) | 3595 (±813) | 3832 (±712) | 3838 (±930) | 4269 (±851) | 4311 (±710) | 2920 (±617) | 2855 (±609) | 2977 (±646) | 3682 (±799) | p = 0.308 | p = 0.769 |
| Control post (n = 9) | 3602 (±1183) | 3323 (±767) | 3707 (±808) | 3938 (±591) | 4209 (±821) | 4328 (±903) | 3042 (±914) | 3074 (±910) | 2952 (±969) | 3465 (±1029) | |||
| TM pre (n = 9) | 3833 (±1350) | 3751 (±1585) | 3806 (±1424) | 3568 (±1330) | 4028 (±1622) | 4033 (±1524) | 2955 (±826) | 2971 (±955) | 3037 (±1053) | 3982 (±1500) | |||
| TM post (n = 9) | 3850 (±1328) | 3037 (±850) | 3634 (±602) | 3788 (±605) | 4129 (±851) | 3952 (±901) | 3019 (±995) | 3238 (±918) | 3223 (±826) | 3832 (±1328) | |||
| Parameter | Group | Pre | Post | pTIME (η2) | pTIME × GROUP |
|---|---|---|---|---|---|
| Vastus lateralis | |||||
| Contraction time (ms) | Control (n = 9) | 25.7 (±6.3) | 27.4 (±1.8) | 0.133 | 0.787 |
| Contraction time (ms) | TM (n = 9) | 25.7 (±3.2) | 28.1 (±3.8) | ||
| Amplitude (mm) | Control (n = 9) | 4.80 (±1.87) | 4.97 (±1.41) | 0.363 | 0.855 |
| Amplitude (mm) | TM (n = 9) | 6.11 (±1.41) | 6.36 (±1.57) | ||
| Gastrocnemius medialis | |||||
| Contraction time (ms) | Control (n = 9) | 21.6 (±3.6) | 26.6 (±4.9) | <0.001 (0.712) | 0.634 |
| Contraction time (ms) | TM (n = 9) | 24.7 (±4.9) | 28.9 (±6.8) | ||
| Amplitude (mm) | Control (n = 9) | 0.008 (0.524) | 0.305 | ||
| Amplitude (mm) | TM (n = 9) | ||||
| Biceps femoris | |||||
| Contraction time (ms) | Control (n = 9) | 35.6 (±8.2) | 44.1 (±5.4) | <0.001 (0.764) | 0.405 |
| Contraction time (ms) | TM (n = 9) | 40.9 (±10.9) | 47.1 (±9.3) | ||
| Amplitude (mm) | Control (n = 9) | 5.91 (±3.31) | 7.99 (±2.16) | <0.001 (0.714) | 0.151 |
| Amplitude (mm) | TM (n = 9) | 7.85 (±5.45) | 11.80 (±5.78) |
| Parameter | Contraction Time | Amplitude |
|---|---|---|
| Vastus lateralis | r = 0.139; p = 0.683 | r = −0.088; p = 0.798 |
| Gastrocnemius medialis | r = −0.631; p = 0.037 | r = −0.707; p = 0.015 |
| Biceps femoris | r = −0.522; p = 0.099 | r = −0.703; p = 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudlof, M.E.; Šimunić, B.; Steuber, B.; Bartel, T.O.; Neshev, R.; Mächler, P.; Dorr, A.; Picha, R.; Schmid-Zalaudek, K.; Goswami, N. Effects of Meditation on Cardiovascular and Muscular Responses in Patients during Cardiac Rehabilitation: A Randomized Pilot Study. J. Clin. Med. 2022, 11, 6143. https://doi.org/10.3390/jcm11206143
Rudlof ME, Šimunić B, Steuber B, Bartel TO, Neshev R, Mächler P, Dorr A, Picha R, Schmid-Zalaudek K, Goswami N. Effects of Meditation on Cardiovascular and Muscular Responses in Patients during Cardiac Rehabilitation: A Randomized Pilot Study. Journal of Clinical Medicine. 2022; 11(20):6143. https://doi.org/10.3390/jcm11206143
Chicago/Turabian StyleRudlof, Maximilian E., Boštjan Šimunić, Bianca Steuber, Till O. Bartel, Ruslan Neshev, Petra Mächler, Andreas Dorr, Rainer Picha, Karin Schmid-Zalaudek, and Nandu Goswami. 2022. "Effects of Meditation on Cardiovascular and Muscular Responses in Patients during Cardiac Rehabilitation: A Randomized Pilot Study" Journal of Clinical Medicine 11, no. 20: 6143. https://doi.org/10.3390/jcm11206143