
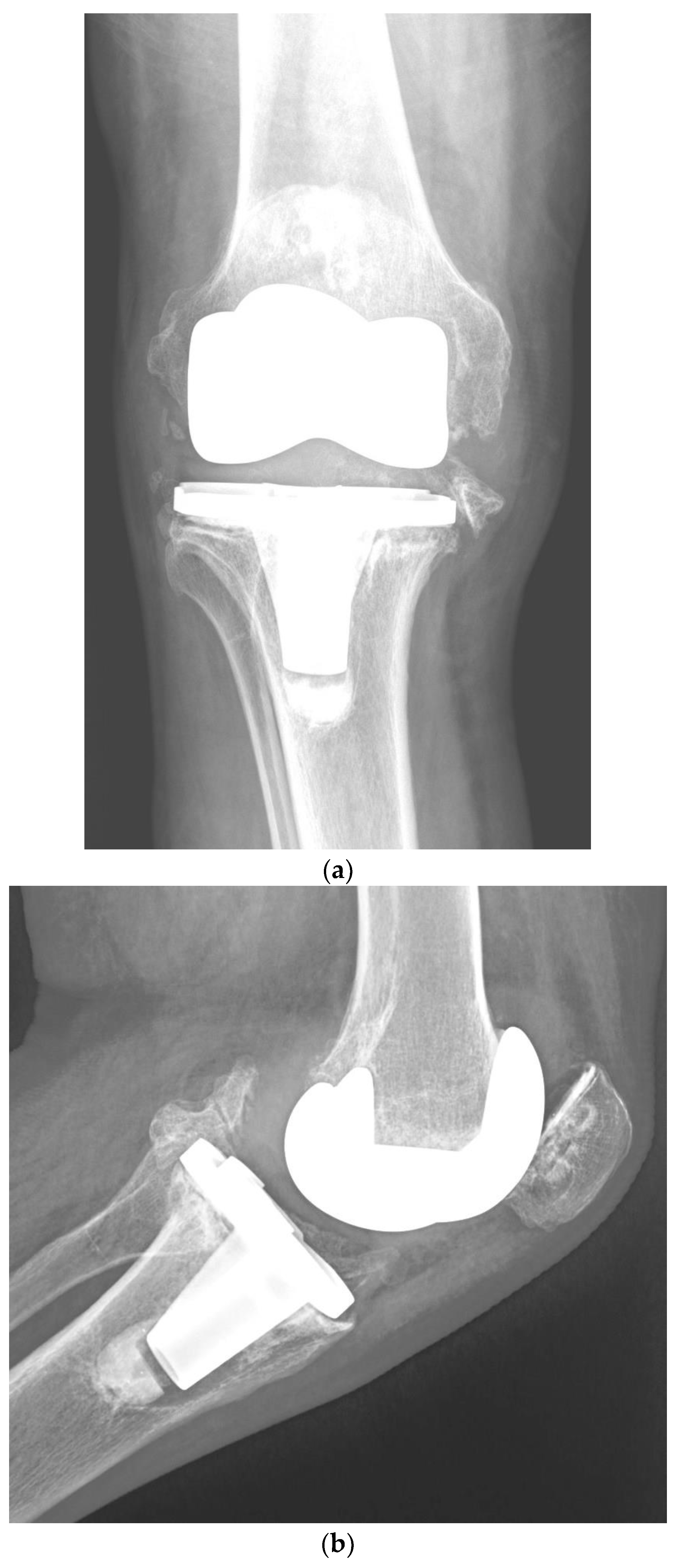
Risk Factors for Periprosthetic Joint Infection after Primary Total Knee Arthroplasty

Abstract
:1. Introduction
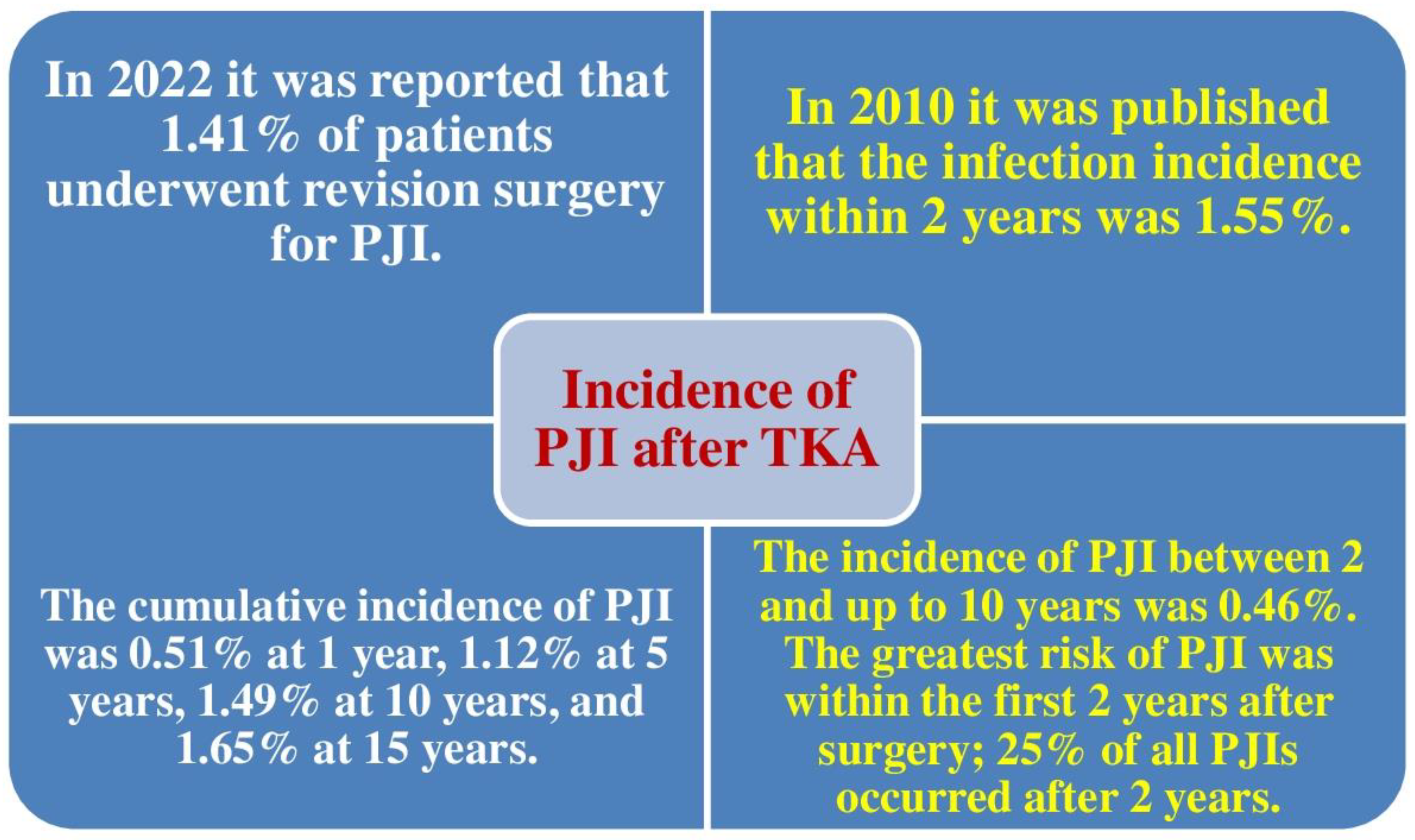
2. Incidence of PJI after TKA
3. Risk Factors for Periprosthetic Joint Infection following Primary TKA
3.1. Patient-Related Risk Factors
3.1.1. Male Gender, Procedure Type (bilateral), Length of Stay over 35 Days, and Usage of Transfusions Have Been Shown to Be Risk Factors for Postoperative PJI
3.1.2. Male Gender, Younger Age, Type II Diabetes, Posttraumatic Osteoarthritis, Patellar Resurfacing, and Discharge to Nursing Home Were Related to an Increased Risk of PJI
3.1.3. Previous Septic Arthritis Has Been Shown to Be a Risk Factor for Postoperative PJI
3.1.4. Smoking Is related to Higher Percentages of PJI
3.1.5. Hypoalbuminemia and Obesity Class II Are Dependable Predictors of PJI
3.1.6. Intra-Articular Injections Prior to TKA Are Related to a Higher Risk of PJI
3.1.7. Greater Glucose Variability in the Postoperative Period Is Related to Higher Percentages of PJI
3.1.8. Reduction of Patient’s Weight Diminishes the Probability of PJI and Minimizes Implant Failure
4. Surgical Risk Factors
4.1. Prolonged Surgical Time Correlates with Increased Infection Risk
4.2. Unilateral versus Bilateral TKA
4.3. Patellar Resurfacing
4.4. Risk Factors in the Postoperative Phase
5. Other Topics of Interest Related to the Risk of PJI following TKA
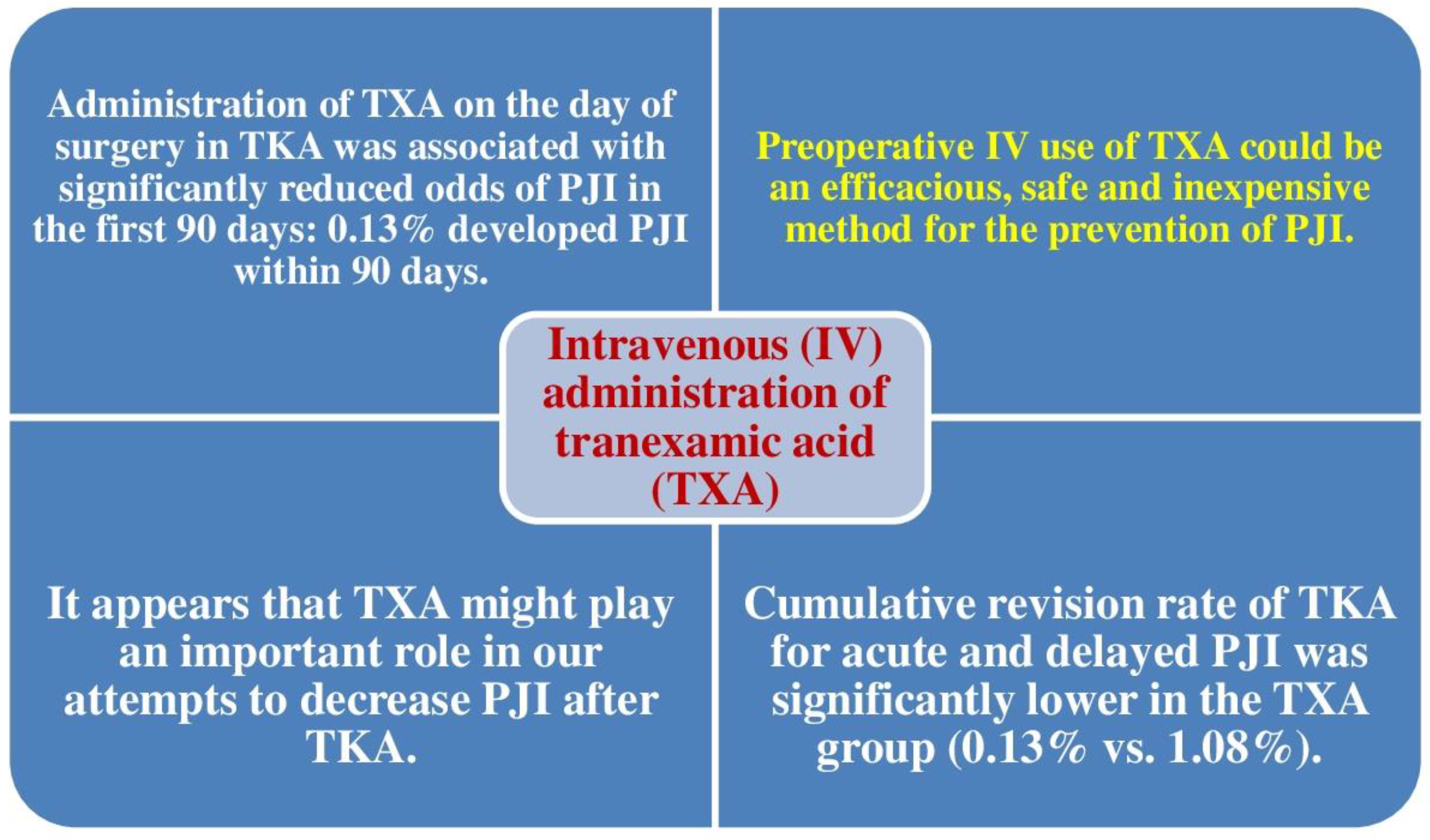
5.1. Tranexamic Acid Diminishes the Risk of Revision TKA for Acute and Late PJI
5.2. Prognostic Nutritional Index as a Predictor of Postoperative PJI
5.3. BMI Is a Superior Predictor of PJI Risk Than Local Quantities of Adipose Tissue
5.4. American College of Surgeons National Surgical Quality Improvement Program SSI Calculator
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Carulli, C.; Villano, M.; Bucciarelli, G.; Martini, C.; Innocenti, M. Painful knee arthroplasty: Definition and overview. Clin. Cases Miner. Bone Metab. 2011, 8, 23–25. [Google Scholar] [PubMed]
- Bengtson, S.; Knutson, K. The infected knee arthroplasty. A 6-year follow-up of 357 cases. Acta Orthop. Scand. 1991, 62, 301–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic joint infection. Lancet 2016, 387, 386–394. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Schmier, J.; Ong, K.L.; Zhao, K.; Parvizi, J. Infection Burden for Hip and Knee Arthroplasty in the United States. J. Arthroplast. 2008, 23, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Petrie, R.S.; Hanssen, A.D.; Osmon, D.R.; Ilstrup, D. Metal-backed patellar component failure in total knee arthroplasty: A possible risk for late infection. Am. J. Orthop. 1998, 27, 172–176. [Google Scholar] [PubMed]
- Zmistowski, B.; Restrepo, C.; Hess, J.; Adibi, D.; Cangoz, S.; Parvizi, J. Unplanned readmission after total joint arthroplasty: Rates, reasons, and risk factors. J. Bone Joint Surg. Am. 2013, 95, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. The EBJIS definition of periprosthetic joint infection. Bone Joint J. 2021, 103, 18–25. [Google Scholar] [CrossRef]
- Wingert, N.C.; Gotoff, J.; Parrilla, E.; Gotoff, R.; Hou, L.; Ghanem, E. The ACS NSQIP Risk Calculator Is a Fair Predictor of Acute Periprosthetic Joint Infection. Clin. Orthop. Relat. Res. 2016, 474, 1643–1648. [Google Scholar] [CrossRef]
- McMaster Arthroplasty Collaborative (MAC). Incidence and predictors of prosthetic joint infection following primary total knee arthroplasty: A 15-year population-based cohort study. J Arthroplast. 2022, 37, 367–372.e1. [Google Scholar] [CrossRef]
- Leonard, H.A.C.; Liddle, A.D.; Burke, O.; Murray, D.W.; Pandit, H. Single- or Two-stage Revision for Infected Total Hip Arthroplasty? A Systematic Review of the Literature. Clin. Orthop. Relat. Res. 2014, 472, 1036–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urish, K.L.; Bullock, A.G.; Kreger, A.M.; Shah, N.B.; Jeong, K.; Rothenberger, S.D.; the Infected Implant Consortium. A Multicenter Study of Irrigation and Debridement in Total Knee Arthroplasty Periprosthetic Joint Infection: Treatment Failure Is High. J. Arthroplast. 2018, 33, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.F.; Kim, K.; Cavadino, A.; Coleman, B.; Munro, J.T.; Young, S.W. Success Rates of Debridement, Antibiotics, and Implant Retention in 230 Infected Total Knee Arthroplasties: Implications for Classification of Periprosthetic Joint Infection. J. Arthroplast. 2021, 36, 305–310.e1. [Google Scholar] [CrossRef] [PubMed]
- Toh, R.X.; Yeo, Z.N.; Liow, M.H.L.; Yeo, S.J.; Lo, N.N.; Chen, J.Y. Debridement, antibiotics, and implant retention in periprosthetic joint infection: What predicts success or failure? J. Arthroplast. 2021, 36, 3562–3569. [Google Scholar] [CrossRef]
- Walkay, S.; Wallace, D.T.; Balasubramaniam, V.S.C.; Maheshwari, R.; Changulani, M.; Sarungi, M. Outcomes of Debridement, Antibiotics and Implant Retention (DAIR) for Periprosthetic Joint Infection in a High-Volume Arthroplasty Centre. Indian J. Orthop. 2022, 56, 1449–1456. [Google Scholar] [CrossRef]
- Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Kurdi, O.; Tauviqirrahman, M.; Winarni, T.I.; Jamari, J. Tresca stress study of CoCrMo-on-CoCrMo bearings based on body mass index using 2D computational Mmdel. J. Tribol. 2022, 33, 31–38. Available online: https://jurnaltribologi.mytribos.org/v33/JT-33-31-38.pdf (accessed on 12 October 2022).
- Shahi, A.; Parvizi, J. Prevention of Periprosthetic Joint Infection. Arch. Bone Jt. Surg. 2015, 3, 72–81. [Google Scholar] [CrossRef]
- Thompson, O.; W-Dahl, A.; Lindgren, V.; Gordon, M.; Robertsson, O.; Stefánsdóttir, A. Similar periprosthetic joint infection rates after and before a national infection control program: A study of 45,438 primary total knee arthroplasties. Acta Orthop. 2022, 93, 3–10. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J.; Berry, D.; Parvizi, J. Prosthetic Joint Infection Risk after TKA in the Medicare Population. Clin. Orthop. Relat. Res. 2010, 468, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Ko, M.S.; Choi, C.H.; Yoon, H.K.; Yoo, J.H.; Oh, H.C.; Lee, J.H.; Park, S.H. Risk factors of postoperative complications following total knee arthroplasty in Korea: A nationwide retrospective cohort study. Medicine 2021, 100, e28052. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Lau, E.; Kurtz, S.; Ong, K.; Berry, D.J. Patient-related Risk Factors for Postoperative Mortality and Periprosthetic Joint Infection in Medicare Patients Undergoing TKA. Clin. Orthop. Relat. Res. 2012, 470, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Cui, Y.; Li, X.; Miao, X.; Wen, Z.; Xue, Y.; Tian, J. Risk factors for deep infection after total knee arthroplasty: A meta-analysis. Arch. Orthop. Trauma. Surg. 2013, 133, 675–687. [Google Scholar] [CrossRef] [PubMed]
- Cordtz, R.L.; Zobbe, K.; Højgaard, P.; Kristensen, L.E.; Overgaard, S.; Odgaard, A.; Lindegaard, H.; Dreyer, L. Predictors of revision, prosthetic joint infection and mortality following total hip or total knee arthroplasty in patients with rheumatoid arthritis: A nationwide cohort study using Danish healthcare registers. Ann. Rheum. Dis. 2018, 77, 281–288. [Google Scholar] [CrossRef]
- Pancio, S.I.; Sousa, P.L.; Krych, A.J.; Abdel, M.P.; Levy, B.A.; Dahm, D.L.; Stuart, M.J. Increased Risk of Revision, Reoperation, and Implant Constraint in TKA After Multiligament Knee Surgery. Clin. Orthop. Relat. Res. 2017, 475, 1618–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.A.; Schleck, C.; Harmsen, W.S.; Jacob, A.K.; Warner, D.O.; Lewallen, D.G. Current tobacco use is associated with higher rates of implant revision and deep infection after total hip or knee arthroplasty: A prospective cohort study. BMC Med. 2015, 13, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Man, S.L.-C.; Chau, W.-W.; Chung, K.-Y.; Ho, K.K.W. Hypoalbuminemia and obesity class II are reliable predictors of peri-prosthetic joint infection in patient undergoing elective total knee arthroplasty. Knee Surg. Relat. Res. 2020, 32, 21. [Google Scholar] [CrossRef]
- Bedard, N.A.; Pugely, A.J.; Elkins, J.M.; Duchman, K.R.; Westermann, R.W.; Liu, S.S.; Gao, Y.; Callaghan, J.J. Do intraarticular injections increase the risk of infection after TKA? Clin. Orthop. Relat. Res. 2017, 475, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Shohat, N.; Restrepo, C.; Allierezaie, A.; Tarabichi, M.; Goel, R.; Parvizi, J. Increased Postoperative Glucose Variability Is Associated with Adverse Outcomes Following Total Joint Arthroplasty. J. Bone Jt. Surg. 2018, 100, 1110–1117. [Google Scholar] [CrossRef]
- Peersman, G.; Laskin, R.; Davis, J.; Peterson, M.G.E.; Richart, T. Prolonged Operative Time Correlates with Increased Infection Rate After Total Knee Arthroplasty. HSSJ 2006, 2, 70–72. [Google Scholar] [CrossRef] [Green Version]
- Odum, S.M.; Springer, B.D. In-Hospital Complication Rates and Associated Factors After Simultaneous Bilateral Versus Unilateral Total Knee Arthroplasty. J. Bone Jt. Surg. Am. 2014, 96, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, G.; Pryke, S.E.R.; Tewari, S.; Rogers, J.; Crowe, B.; Bridgfoot, L.; Smith, N. Safety and cost benefits of bilateral total knee replacement in an acute hospital. ANZ J. Surg. 2005, 75, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Memtsoudis, S.G.; Ma, Y.; González Della Valle, A.; Mazumdar, M.; Gaber-Baylis, L.K.; MacKenzie, C.R.; Sculco, T.P. Perioperative outcomes after unilateral and bilateral total knee arthroplasty. J. Am. Soc. Anesthesiol. 2009, 111, 1206–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilling, R.W.; Moulder, E.; Allgar, V.; Messner, J.; Sun, Z.; Mohsen, A. Patellar resurfacing in primary total knee replacement: A meta-analysis. J. Bone Jt. Surg. Am. 2012, 94, 2270–2278. [Google Scholar] [CrossRef]
- Lacko, M.; Jarčuška, P.; Schreierova, D.; Lacková, A.; Gharaibeh, A. Tranexamic acid decreases the risk of revision for acute and delayed periprosthetic joint infection after total knee replacement. Jt. Dis. Relat. Surg. 2020, 31, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Hong, G.J.; Wilson, L.A.; Liu, J.; Memtsoudis, S.G. Tranexamic Acid Administration is Associated with a Decreased Odds of Prosthetic Joint Infection Following Primary Total Hip and Primary Total Knee Arthroplasty: A National Database Analysis. J. Arthroplast. 2020, 36, 1109–1113. [Google Scholar] [CrossRef]
- Hanada, M.; Hotta, K.; Matsuyama, Y. Prognostic nutritional index as a risk factor for aseptic wound complications after total knee arthroplasty. J. Orthop. Sci. 2021, 26, 827–830. [Google Scholar] [CrossRef]
- Shearer, J.; Agius, L.; Burke, N.; Rahardja, R.; Young, S.W. BMI is a Better Predictor of Periprosthetic Joint Infection Risk Than Local Measures of Adipose Tissue After TKA. J. Arthroplast. 2020, 35, S313–S318. [Google Scholar] [CrossRef]
- Gómez-Barrena, E.; Warren, T.; Walker, I.; Jain, N.; Kort, N.; Loubignac, F.; Newman, S.; Perka, C.; Spinarelli, A.; Whitehouse, M.R.; et al. Prevention of Periprosthetic Joint Infection in Total Hip and Knee Replacement: One European Consensus. J. Clin. Med. 2022, 11, 381. [Google Scholar] [CrossRef]
- Hinarejos, P.; Guirro, P.; Leal, J.; Monserrat, F.; Pelfort, X.; Sorli, M.L.; Horcajada, J.P.; Piug, L. The use of erythromycin and colistin-loaded cement in total knee arthroplasty does not reduce the incidence of infection: A prospective randomized study in 3000 knees. J. Bone Jt. Surg. Am. 2013, 95, 769–774. [Google Scholar] [CrossRef]
- Chiu, F.-Y.; Chen, C.-M.; Lin, C.-F.J.; Lo, W.-H. Cefuroxime-impregnated cement in primary total knee arthroplasty: A prospective, randomized study of three hundred and forty knees. J. Bone Jt. Surg. Am. 2002, 84, 759–762. [Google Scholar] [CrossRef]
- Chiu, F.-Y.; Lin, C.-F.J. Antibiotic-Impregnated Cement in Revision Total Knee Arthroplasty. J. Bone Jt. Surg. 2009, 91, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Chiu, F.-Y.; Lin, C.-F.J.; Chen, C.-M.; Lo, W.-H.; Chaung, T.-Y. Cefuroxime-impregnated cement at primary total knee arthroplasty in diabetes mellitus. J. Bone Jt. Surgery. Br. Vol. 2001, 83, 691–695. [Google Scholar] [CrossRef]
- Calkins, T.E.; Culvern, C.; Nam, D.; Gerlinger, T.L.; Levine, B.R.; Sporer, S.M.; Della Valle, C.J. Dilute Betadine Lavage Reduces the Risk of Acute Postoperative Periprosthetic Joint Infection in Aseptic Revision Total Knee and Hip Arthroplasty: A Randomized Controlled Trial. J. Arthroplast. 2020, 35, 538–543.e1. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.; Whitehouse, M.; Blom, A.W.; Beswick, A.; Team, I. Patient-Related Risk Factors for Periprosthetic Joint Infection after Total Joint Arthroplasty: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0150866. [Google Scholar] [CrossRef]
- Adams, A.L.; Paxton, E.W.; Wang, J.Q.; Johnson, E.S.; Bayliss, E.A.; Ferrara, A.; Nakasato, C.; Bini, S.A.; Namba, R.S. Surgical Outcomes of Total Knee Replacement According to Diabetes Status and Glycemic Control, 2001 to 2009. J. Bone Jt. Surg. 2013, 95, 481–487. [Google Scholar] [CrossRef]
- Nelson, C.L.; Elkassabany, N.M.; Kamath, A.F.; Liu, J. Low Albumin Levels, More Than Morbid Obesity, Are Associated with Complications After TKA. Clin. Orthop. Relat. Res. 2015, 473, 3163–3172. [Google Scholar] [CrossRef] [Green Version]
- Peersman, G.; Laskin, R.; Davis, J.; Peterson, M. Infection in total knee replacement: A retrospective review of 6489 total knee replacements. Clin. Orthop. Relat. Res. 2001, 392, 15–23. [Google Scholar] [CrossRef]
- Bohl, D.D.; Shen, M.R.; Kayupov, E.; Cvetanovich, G.L.; Della Valle, C.J. Is Hypoalbuminemia Associated with Septic Failure and Acute Infection After Revision Total Joint Arthroplasty? A Study of 4517 Patients from the National Surgical Quality Improvement Program. J. Arthroplast. 2016, 31, 963–967. [Google Scholar] [CrossRef]
- Walls, J.D.; Abraham, D.; Nelson, C.L.; Kamath, A.F.; Elkassabany, N.M.; Liu, J. Hypoalbuminemia More Than Morbid Obesity is an Independent Predictor of Complications After Total Hip Arthroplasty. J. Arthroplast. 2015, 30, 2290–2295. [Google Scholar] [CrossRef]
- Rai, J.; Gill, S.S.; Kumar, B.R.J.S. The influence of preoperative nutritional status in wound healing after replacement arthroplasty. Orthopedics 2002, 25, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. (In Japanese) [Google Scholar] [PubMed]
- Tei, M.; Ikeda, M.; Haraguchi, N.; Takemasa, I.; Mizushima, T.; Ishii, H.; Yamamoto, H.; Sekimoto, M.; Doki, Y.; Mori, M. Risk factors for postoperative delirium in elderly patients with colorectal cancer. Surg. Endosc. 2010, 24, 2135–2139. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, R.; Sakamoto, Y.; Nakagawa, S.; Miyamoto, Y.; Yoshida, N.; Oki, E.; Watanabe, M.; Baba, H. Prognostic Nutritional Index Predicts Severe Complications, Recurrence, and Poor Prognosis in Patients with Colorectal Cancer Undergoing Primary Tumor Resection. Dis. Colon Rectum 2015, 58, 1048–1057. [Google Scholar] [CrossRef]
- Kirschbaum, S.; Erhart, S.; Perka, C.; Hube, R.; Thiele, K. Failure Analysis in Multiple TKA Revisions—Periprosthetic Infections Remain Surgeons’ Nemesis. J. Clin. Med. 2022, 11, 376. [Google Scholar] [CrossRef]
- Muwanis, M.; Barimani, B.; Luo, L.; Wang, C.K.; Dimentberg, R.; Albers, A. Povidone-iodine irrigation reduces infection after total hip and knee arthroplasty. Arch. Orthop. Trauma. Surg. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Buchalter, D.B.; Nduaguba, A.; Teo, G.M.; Kugelman, D.; Aggarwal, V.K.; Long, W.J. Cefazolin remains the linchpin for preventing acute periprosthetic joint infection following primary total knee arthroplasty. Bone Jt. Open 2022, 3, 35–41. [Google Scholar] [CrossRef]
- Parkulo, T.D.; Likine, E.; Ong, K.L.; Watson, H.; Smith, L.S.; Malkani, A.L. Manipulation Following Primary Total Knee Arthroplasty is Associated with Increased Rates of Infection and Revision. J. Arthroplast. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Mont, M.A.; Chen, A.F.; Della Valle, C.; Sodhi, N.; Lau, E.; Ong, K.L. Intra-Articular Corticosteroid or Hyaluronic Acid Injections Are Not Associated with Periprosthetic Joint Infection Risk following Total Knee Arthroplasty. J. Knee Surg. 2022, 35, 983–996. [Google Scholar] [CrossRef]
- Avila, A.; Acuña, A.J.; Do, M.T.; Samuel, L.T.; Kamath, A.F. Intra-articular injection receipt within 3 months prior to primary total knee arthroplasty is associated with increased periprosthetic joint infection risk. Knee Surg. Sport. Traumatol. Arthrosc. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, L.; Ren, X.; Nie, L. Do preoperative intra-articular injections of corticosteroids or hyaluronic acid increase the risk of infection after total knee arthroplasty? A meta-analysis. Bone Jt. Res. 2022, 11, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.-H.; Han, S.-B.; Song, J.-E. Risk of Periprosthetic Joint Infection in Patients with Total Knee Arthroplasty Undergoing Colonoscopy: A Nationwide Propensity Score Matched Study. J. Arthroplast. 2022, 37, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Rahardja, R.; Morris, A.J.; Hooper, G.J.; Grae, N.; Frampton, C.M.; Young, S.W. Surgical Helmet Systems Are Associated with a Lower Rate of Prosthetic Joint Infection After Total Knee Arthroplasty: Combined Results from the New Zealand Joint Registry and Surgical Site Infection Improvement Programme. J. Arthroplast. 2022, 37, 930–935.e1. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, N.P.; Browne, J.A.; Werner, B.C. The Timing of Preoperative Urinary Tract Infection Influences the Risk of Prosthetic Joint Infection Following Primary Total Hip and Knee Arthroplasty. J. Arthroplast. 2022, 19, S0883–S5403. [Google Scholar] [CrossRef]
- Fisher, N.D.; Bi, A.S.; Singh, V.; Sicat, C.S.; Schwarzkopf, R.; Aggarwal, V.K.; Rozell, J.C. Are patient-reported drug allergies associated with prosthetic joint infections and functional outcomes following total hip and knee arthroplasty? J. Arthroplast. 2022, 37, 26–30. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PJI Exists When | |
|---|---|
| 1 | There is a sinus tract communicating with the implant; or |
| 2 | A bacterium is isolated by culture from 2 or more separate tissue or fluid samples attained from the affected knee; or |
| 3 | When 4 of the following 6 criteria exist:
|
| Risk Factors | |
|---|---|
| Patient-related risk factors |
|
| Surgical risk factors |
|
| Risk factors in the postoperative period |
|
| Measures |
|---|
| Changeable Risk Factors Should Be Optimized before TKA |
| Patient education should involve skin cleaning methods with a remnant antiseptic solution |
| Alcoholic chlorhexidine provides better protection than alcoholic povidone-iodine against PJI |
| Alcohol-based solutions should be utilized in surgical hand preparation |
| A standardized method to the utilize of antiseptics should be in place, with special attention to the incision area |
| Antibiotic prophylaxis should be given before surgery and not routinely prolonged |
| Traffic and number of personnel in the operating room should be maintained to a minimum |
| Tranexamic acid and hemostatic drug utilization should be optimized to diminish the need for a surgical drain |
| Structured monitoring and reporting protocols for PJI should be in place |
| Specific instructions for PJI should be created and executed; these should be tailored to individual patient risk factors |
| Instructions based on level 1 or 2 of evidence should be deemed compulsory |
| Infections that appear 30 days after surgery can still be deemed to be PJI |
| Risk Factor | Control Needed |
|---|---|
| Hyperglycemia | Control preoperatively |
| Obesity | Try to control |
| Hypertension | Control preoperatively |
| Previous intra-articular injections | Avoid 6 months before |
| Hypoalbuminemia | Unknown if control decreases risk |
| Tobacco use | Cessation of smoking at least 1 month before |
| Previous infection | Wait at least 3 months after infection is resolved |
| Nutritional status | Unknown if control decreases risk |
| Preoperative anemia | Correct preoperatively |
| Steroid therapy | Avoid for 1 month before, if possible |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Merchan, E.C.; Delgado-Martinez, A.D. Risk Factors for Periprosthetic Joint Infection after Primary Total Knee Arthroplasty. J. Clin. Med. 2022, 11, 6128. https://doi.org/10.3390/jcm11206128
Rodriguez-Merchan EC, Delgado-Martinez AD. Risk Factors for Periprosthetic Joint Infection after Primary Total Knee Arthroplasty. Journal of Clinical Medicine. 2022; 11(20):6128. https://doi.org/10.3390/jcm11206128
Chicago/Turabian StyleRodriguez-Merchan, Emerito Carlos, and Alberto D. Delgado-Martinez. 2022. "Risk Factors for Periprosthetic Joint Infection after Primary Total Knee Arthroplasty" Journal of Clinical Medicine 11, no. 20: 6128. https://doi.org/10.3390/jcm11206128