
Prevalence of Osteoporosis Assessed by DXA and/or CT in Severe Obese Patients
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
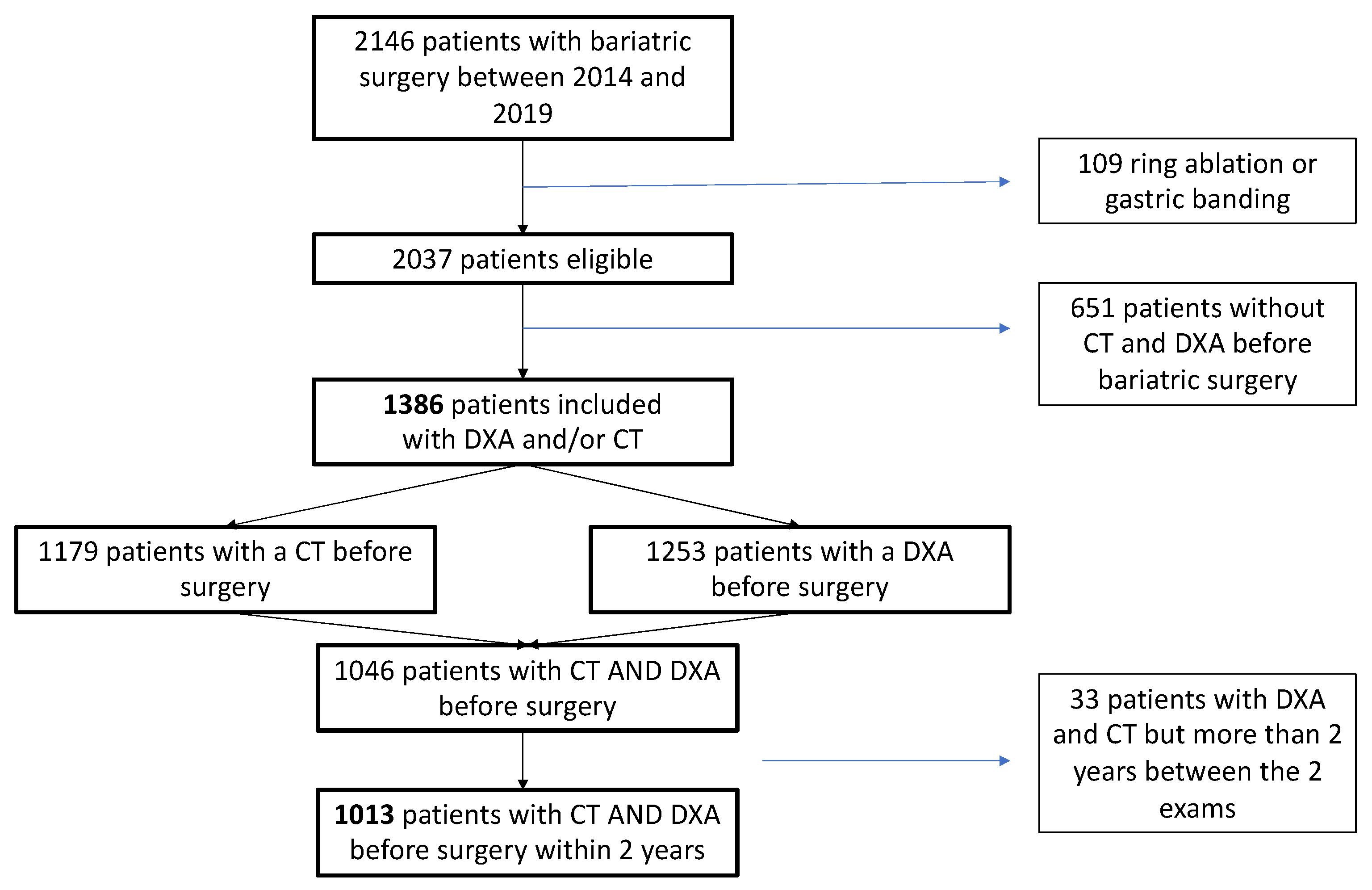
2.1. Population
2.2. DXA Evaluation
2.3. CT Evaluation
2.4. Vertebral Facture
2.5. Ethics Approval
2.6. Statistical Analysis
3. Results
3.1. Population
3.2. Patients with Both CT and DXA Evaluation within 2 Years (n = 1013)
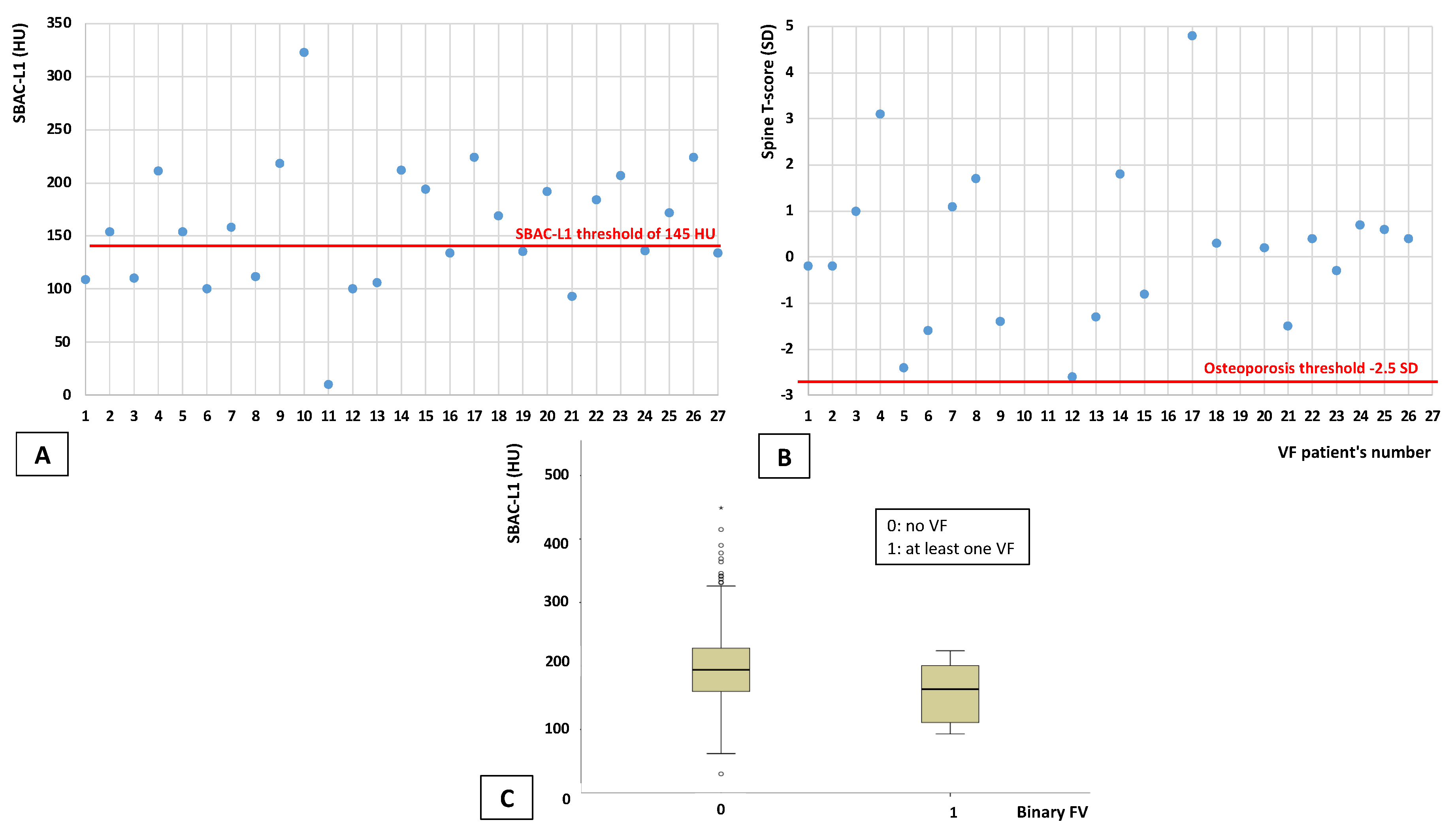
3.3. Discordance Analysis between CT and DXA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Physical Status: The Use of and Interpretation of Anthropometry, Report of a WHO Expert Committee; WHO: Geneva, Switzerland, 1995; Volume 854, pp. 1–452. [Google Scholar]
- Cheng, H.L.; Medlow, S.; Steinbeck, K. The Health Consequences of Obesity in Young Adulthood. Curr. Obes. Rep. 2016, 5, 30–37. [Google Scholar] [CrossRef] [PubMed]
- MeMechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; McMahon, M.M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical practice guidelines for the periop-erative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: Cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity 2013, 21 (Suppl. 1), S1–S27. [Google Scholar]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep. Ser. 1994, 843, 1–129. [Google Scholar]
- Briot, K.; Roux, C.; Thomas, T.; Blain, H.; Buchon, D.; Chapurlat, R.; Debiais, F.; Feron, J.M.; Gauvain, J.B.; Guggenbuhl, P.; et al. 2018 update of French recommendations on the management of postmenopausal osteoporosis. Jt. Bone Spine 2018, 85, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, P.; Mouquet, M.-C. Quel Risque De Décès Un an Après Une Fracture Du Col Du FÉmur? Direction de la Recherche, des Études, de l’Évaluation et des Statistiques: Paris, France, 2016; Volume 6.
- Yu, E.W. Bone metabolism after bariatric surgery. J. Bone Miner. Res. 2014, 29, 1507–1518. [Google Scholar] [CrossRef] [Green Version]
- Scibora, L.M.; Ikramuddin, S.; Buchwald, H.; Petit, M.A. Examining the Link Between Bariatric Surgery, Bone Loss, and Osteoporosis: A Review of Bone Density Studies. Obes. Surg. 2012, 22, 654–667. [Google Scholar] [CrossRef]
- Premaor, M.O.; Pilbrow, L.; Tonkin, C.; A Parker, R.; Compston, J. Obesity and fractures in postmenopausal women. J. Bone Miner. Res. 2010, 25, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Kanis, J.A.; Odén, A.; McCloskey, E.; Chapurlat, R.D.; Christiansen, C.; Cummings, S.R.; Diez-Perez, A.; Eisman, J.A.; Fujiwara, S.; et al. A Meta-Analysis of the Association of Fracture Risk and Body Mass Index in Women. J. Bone Miner. Res. 2013, 29, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Chen, Y.; Li, J.; Chen, D.; Cheng, Z.; Xu, S.; Huang, Y.; Wang, Q. A meta-analysis of the effects of bariatric surgery on fracture risk. Obes. Rev. 2018, 19, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Gregson, C.; for the GLOW Investigators; Dennison, E.; Compston, J.E.; Adami, S.; Adachi, J.D.; Anderson, F.A.; Boonen, S.; Chapurlat, R.; Diez-Perez, A.; et al. Disease-specific perception of fracture risk and incident fracture rates: GLOW cohort study. Osteoporos. Int. 2014, 25, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickhardt, P.J.; Pooler, B.D.; Lauder, T.; Del Rio, A.M.; Bruce, R.J.; Binkley, N. Opportunistic Screening for Osteoporosis Using Abdominal Computed Tomography Scans Obtained for Other Indications. Ann. Intern. Med. 2013, 158, 588–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrier-Cornet, J.; Omorou, A.Y.; Fauny, M.; Loeuille, D.; Chary-Valckenaere, I. Opportunistic screening for osteoporosis using thoraco-abdomino-pelvic CT-scan assessing the vertebral density in rheumatoid arthritis patients. Osteoporos. Int. 2019, 30, 1215–1222. [Google Scholar] [CrossRef]
- Fauny, M.; Albuisson, E.; Bauer, E.; Perrier-Cornet, J.; Chary-Valckenaere, I.; Loeuille, D. Study of vertebral fracture and Scano-graphic Bone Attenuation Coefficient in rheumatoid arthritis and ankylosing spondylitis vs. controls. Sci. Rep. 2019, 9, 13323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauny, M.; Bauer, E.; Albuisson, E.; Perrier-Cornet, J.; Deibener, J.; Chabot, F.; Mandry, D.; Huttin, O.; Chary-Valckenaere, I.; Loeuille, D. Vertebral fracture prevalence and measurement of the scanographic bone attenuation coefficient on CT-scan in patients with systemic sclerosis. Rheumatol. Int. 2018, 38, 1901–1910. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Lee, S.; Liu, J.; Yao, J.; Lay, N.; Graffy, P.M.; Summers, R.M. Population-based opportunistic osteoporosis screening: Validation of a fully automated CT tool for assessing longitudinal BMD changes. Br. J. Radiol. 2019, 92, 20180726. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Graffy, P.M.; Ziemlewicz, T.J.; Lee, S.J.; Summers, R.M.; Pickhardt, P.J. Opportunistic Osteoporosis Screening at Routine Abdominal and Thoracic CT: Normative L1 Trabecular Attenuation Values in More than 20,000 Adults. Radiology 2019, 291, 360–367. [Google Scholar] [CrossRef]
- Alpantaki, K.; Bano, A.; Pasku, D.; Mavrogenis, A.F.; Papagelopoulos, P.J.; Sapkas, G.S.; Korres, D.S.; Katonis, P. Thoracolumbar burst fractures: A systematic review of management. Orthopedics 2010, 33, 422–429. [Google Scholar] [CrossRef] [Green Version]
- Genant, H.K.; Wu, C.Y.; van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitative technique. J. Bone Miner. Res. 1993, 8, 1137–1148. [Google Scholar] [CrossRef]
- Greco, E.A.; Fornari, R.; Rossi, F.; Santiemma, V.; Prossomariti, G.; Annoscia, C.; Aversa, A.; Brama, M.; Marini, M.; Donini, L.M.; et al. Is obesity protective for osteoporosis? Evaluation of bone mineral density in individuals with high body mass index. Int. J. Clin. Pract. 2010, 64, 817–820. [Google Scholar] [CrossRef]
- Hsu, Y.-H.; A Venners, S.; A Terwedow, H.; Feng, Y.; Niu, T.; Li, Z.; Laird, N.; Brain, J.D.; Cummings, S.R.; Bouxsein, M.L.; et al. Relation of body composition, fat mass, and serum lipids to osteoporotic fractures and bone mineral density in Chinese men and women. Am. J. Clin. Nutr. 2006, 83, 146–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldroyd, A.; Mitchell, K.; Bukhari, M. The prevalence of osteoporosis in an older population with very high body mass index: Evidence for an association. Int. J. Clin. Pract. 2014, 68, 771–774. [Google Scholar] [CrossRef]
- Lespessailles, E.; Paccou, J.; Javier, R.-M.; Thomas, T.; Cortet, B.; GRIO Scientific Committee. Obesity, Bariatric Surgery, and Fractures. J. Clin. Endocrinol. Metab. 2019, 104, 4756–4768. [Google Scholar] [CrossRef] [PubMed]
- Kaze, A.D.; Rosen, H.N.; Paik, J.M. A meta-analysis of the association between body mass index and risk of vertebral fracture. Osteoporos. Int. 2017, 29, 31–39. [Google Scholar] [CrossRef]
- Kim, K.-C.; Shin, D.-H.; Lee, S.-Y.; Im, J.-A.; Lee, D.-C. Relation between Obesity and Bone Mineral Density and Vertebral Fractures in Korean Postmenopausal Women. Yonsei Med. J. 2010, 51, 857–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obésité et Ostéoporose. Available online: https://www.edimark.fr/lettre-rhumatologue/obesite-osteoporose (accessed on 25 February 2022).
- Cortet, B.; Roux, C. Obésité et ostéoporose. Rev. Rhum. Monogr. 2016, 83, 25–28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| DXA and CT | |
|---|---|
| Demographical Data | n = 1013 |
| Age (years) | 49.0 (±18.0) |
| Sex (women) | 776 (76.6%) |
| BMI (kg/m²) | 44.6 (±8.3) |
| Diabetes | 316 (31.2%) |
| Cardiovascular risk factor | 584 (57.7%) |
| Tabaco Smokers Never smokers | 412 (42%) 569 (58%) |
| Alcohol | 42 (4.3%) |
| Vitamin D deficiency | 842 (91.3%) |
| CT | |
| Vertebral fractures (patients) | 22 (2.2%) |
| Number of vertebral fractures | 32 |
| SBAC-L1(HU) | 194.0 (±69.0) |
| SBAC-L1 ≤ 145 HU | 163 (16.1%) |
| SBAC-L1 >145 HU | 850 (83.9%) |
| DXA | |
| Femoral neck | |
| BMD (g/cm²) | 1.098 (±0.15) |
| T-score (SD) | 0.9 (±1.5) |
| Osteoporosis | 2 (0.2%) |
| Osteopenia | 65 (6.4%) |
| Hip | |
| BMD (g/cm²) | 1.169 (±0.15) |
| T-score (SD) | 1.4 (±1.6) |
| Osteoporosis | 0 (0%) |
| Osteopenia | 21 (2.1%) |
| Spine (L1-L4) | |
| BMD (g/cm²) | 1.273 (±0.16) |
| T-score (SD) | 0.8 (±1.7) |
| Osteoporosis | 8 (0.79%) |
| Osteopenia | 73 (7.2%) |
| Osteoporosis on at least one site | 8 (0.8%) |
| Osteopenia on at least one site | 119 (11.7%) |
| Fat mass (kg) | 60.5 (±17.8) |
| Lean mass (kg) | 55.6 (±14.2) |
| Fat mass/total weight (%) | 51.0% (±6.3) |
| Android fat mass/Gynoid fat mass | 1.6 (±0.7) |
| Lipodystrophy index | 0.8 (±0.3) |
| Sarcopenia | 10.1 (±1.9) |
| VAT (g) | 2407.0 (±1594.0) |
| SBAC-L1 | Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | >145 HU | ≤145 HU | p Value | OR | CI 95 | p Value | OR | CI 95 | |
| Demographic data | 850 patients | 163 patients | |||||||
| Age (year) | 1013 | 47.0 (±16.0) | 59.0 (±12.0) | 0.0001 | 1.1 | [1.10–1.14] | 0.0001 | 1.1 | [1.08–1.16] |
| Sex (women) | 1013 | 678 (79.8%) | 98 (60.1%) | 0.0001 | 0.4 | [0.27–0.55] | 0.6 | 1.3 | [0.47–3.82] |
| BMI (g/cm²) | 1013 | 44.8 (±8.5) | 43.0 (±7.4) | 0.01 | 0.9 | [0.9–0.99] | 0.0001 | 0.9 | [0.82–0.92] |
| Diabetes | 1013 | 245 (28.8%) | 71 (43.6%) | 0.0001 | 1.9 | [1.35–2.68] | 0.3 | 0.8 | [0.43–1.32] |
| Cardiovascular risk factor | 1013 | 460 (54.1%) | 124 (76.1%) | 0.0001 | 2.7 | [1.84–3.96] | 0.8 | 1.1 | [0.61–1.94] |
| Tabacco Smokers Never smokers | 981 | 337 (39.6%) 487 (57.3%) | 75 (46.0%) 82 (50.3%) | 0.11 | 1.3 | [0.94–1.86] | |||
| Alcohol | 981 | 31 (3.6%) | 11 (6.7%) | 0.07 | 1.9 | [0.95–3.92] | |||
| Vitamin D deficiency | 922 | 708 (83.3%) | 134 (82.2%) | 0.5 | 0.8 | [0.45–1.48] | |||
| CT | 1013 | 850 patients | 163 patients | ||||||
| Vertebral fractures (patients) | 13 (1.5%) | 9 (5.5%) | 0.003 | 3.8 | [1.58–8.96] | ||||
| DXA | 1013 | 850 patients | 163 patients | ||||||
| Femoral neck | |||||||||
| BMD (g/cm²) | 1.120 (±0.14) | 0.985 (±0.16) | 0.0001 | 0.001 | [0.0001–0.004] | 0.03 | 0.04 | [0.005–0.33] | |
| T-score (SD) | 1.1 (±1.3) | −0.2 (±1.6) | 0.0001 | 0.3 | [0.28–0.42] | ||||
| Osteoporosis | 2 (0.2%) | 0 (0%) | |||||||
| Osteopenia | 25 (2.9%) | 40 (24.5%) | 0.0001 | 11.1 | [6.45–18.97] | ||||
| Hip | |||||||||
| BMD (g/cm²) | 1.189 (±0.14) | 1.067 (±0.14) | 0.0001 | 0.002 | [0.001–0.009] | ||||
| T-score (SD) | 1.5 (±1.4) | 0.3 (±1.3) | 0.0001 | 0.4 | [0.30–0.45] | ||||
| Osteoporosis | 0 (0%) | 0 (0%) | |||||||
| Osteopenia | 10 (1.2%) | 11 (6.7%) | 0.0001 | 6.0 | [2.51–14.48] | ||||
| Spine (L1-L4) | |||||||||
| BMD (g/cm²) | 1.295 (±0.15) | 1.159 (±0.14) | 0.0001 | 0.001 | [0.0001–0.006] | 0.0001 | 0.001 | [0.0001–0.008] | |
| T-score (SD) | 1.0 (±1.5) | −0.2 (±1.3) | 0.0001 | 0.4 | [0.38–0.53] | ||||
| Osteoporosis | 3 (0.4%) | 5 (3.1%) | 0.003 | 9.0 | [2.12–38.02] | ||||
| Osteopenia | 39 (4.6%) | 34 (20.9%) | 0.0001 | 5.6 | [3.41–9.30] | ||||
| Osteoporosis on at least on site | 3 (0.4%) | 5 (3.1%) | 0.003 | 8.9 | [2.11–37.68] | ||||
| Osteopenia on at least one site | 60 (7.1%) | 59 (36.2%) | 0.0001 | 7.8 | [5.12–11.91] | ||||
| Fat mass (kg) | 60.9 (±17.8) | 59.3 (±19.3) | 0.09 | 0.99 | [0.98–1.00] | ||||
| Lean mass (kg) | 55.4 (±13.4) | 57.9 (±20.2) | 0.007 | 1.02 | [1.01–1.04] | 0.002 | 1.1 | [1.03–1.13] | |
| Fat mass/total weight (%) | 51.2% (±6.2) | 49.4% (±7.9) | 0.0001 | 0.94 | [0.92–0.97] | ||||
| Android fat mass/Gynoid fat mass | 1.6 (±0.7) | 1.8 (±0.8) | 0.001 | 2.3 | [1.69–3.08] | ||||
| Lipodystrophy index | 0.8 (±0.3) | 0.6 (±0.3) | 0.0001 | 0.068 | [0.026–0.180] | 0.9 | 1.1 | [0.18–7.47] | |
| Sarcopenia | 10.1 (±1.9) | 10.4 (±2.1) | 0.39 | 1.05 | [0.94–1.18] | ||||
| VAT (g) | 2301.5 (±1472.8) | 3104.0 (±2372.0) | 0.0001 | 1 | [1–1.001] | 0.02 | 1 | [1.0–1.001] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halin, M.; Allado, E.; Albuisson, E.; Brunaud, L.; Chary-Valckenaere, I.; Loeuille, D.; Quilliot, D.; Fauny, M. Prevalence of Osteoporosis Assessed by DXA and/or CT in Severe Obese Patients. J. Clin. Med. 2022, 11, 6114. https://doi.org/10.3390/jcm11206114
Halin M, Allado E, Albuisson E, Brunaud L, Chary-Valckenaere I, Loeuille D, Quilliot D, Fauny M. Prevalence of Osteoporosis Assessed by DXA and/or CT in Severe Obese Patients. Journal of Clinical Medicine. 2022; 11(20):6114. https://doi.org/10.3390/jcm11206114
Chicago/Turabian StyleHalin, Marion, Edem Allado, Eliane Albuisson, Laurent Brunaud, Isabelle Chary-Valckenaere, Damien Loeuille, Didier Quilliot, and Marine Fauny. 2022. "Prevalence of Osteoporosis Assessed by DXA and/or CT in Severe Obese Patients" Journal of Clinical Medicine 11, no. 20: 6114. https://doi.org/10.3390/jcm11206114