
Impact of Pre-Operative Right Ventricular Response to Hemodynamic Optimization on Outcomes in Patients with LVADs
Abstract
:1. Introduction
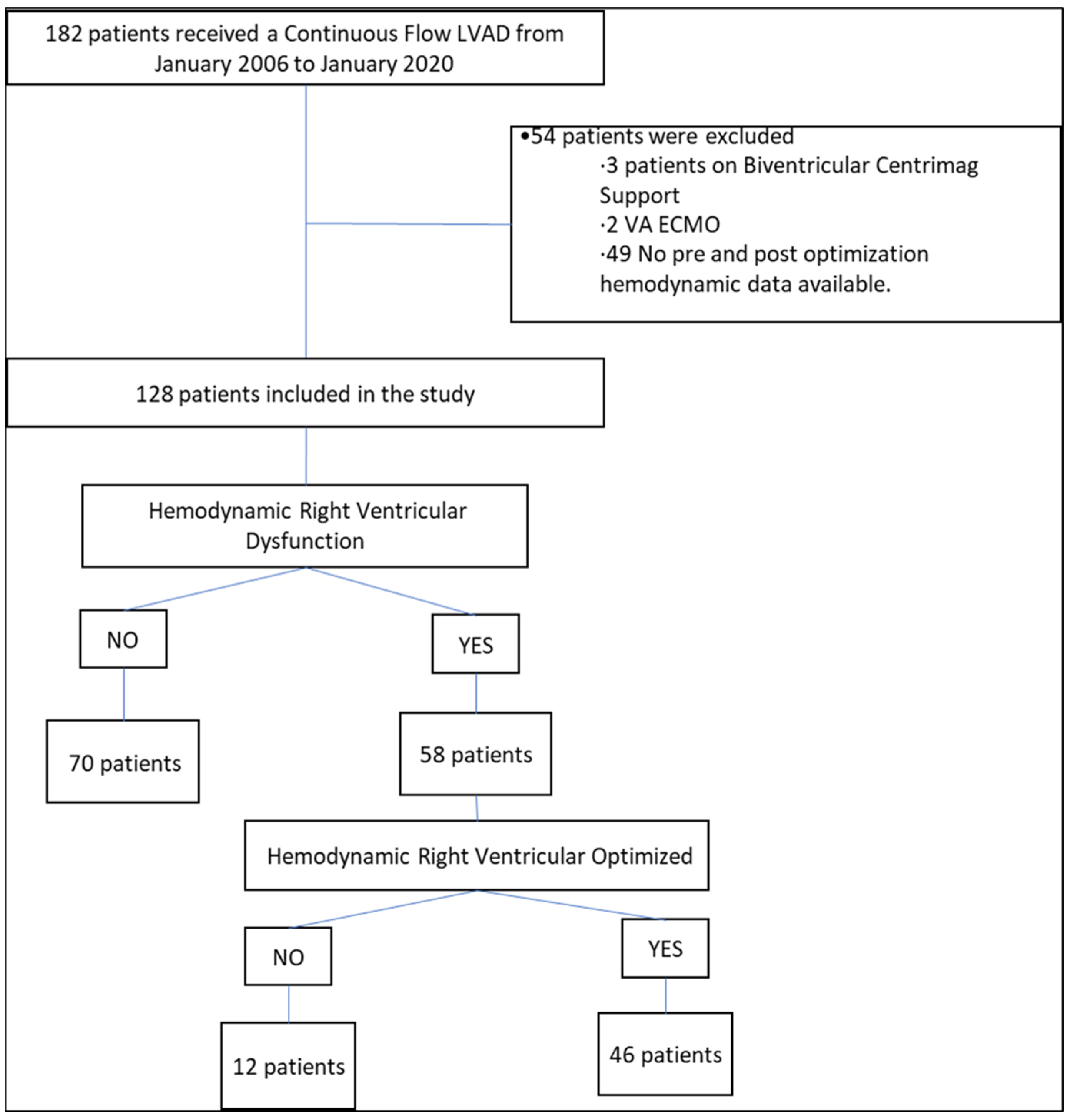
2. Methods
Statistical Analysis
3. Results
3.1. Hemodynamic Parameters
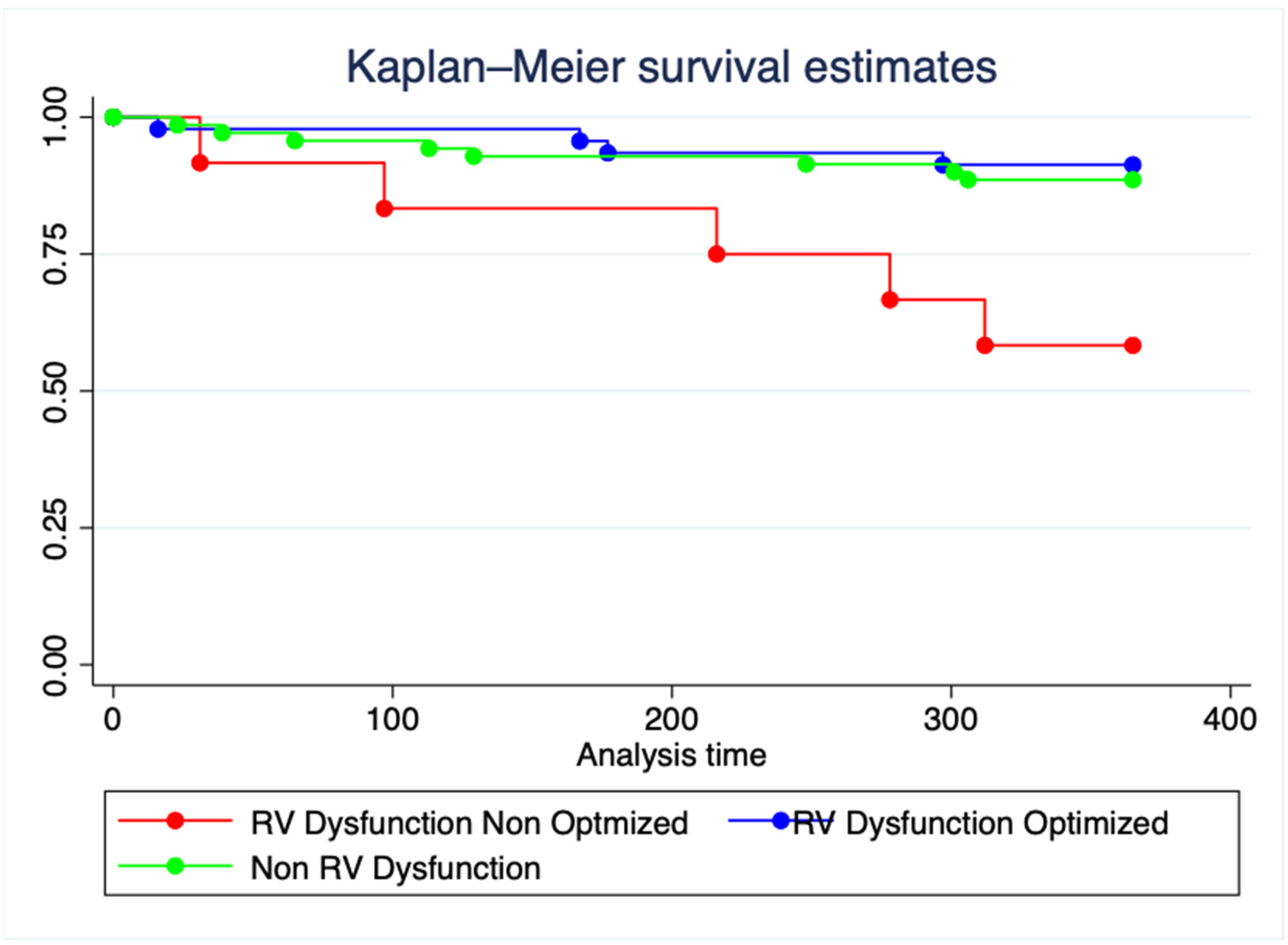
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Colombo, P.C.; Cleveland, J.C.; Long, J.W.; Salerno, C.; Goldstein, D.J.; Patel, C.B.; Ewald, G.A.; Tatooles, A.J.; Silvestry, S.C.; et al. Hemocompatibility-Related Outcomes in the MOMENTUM 3 Trial at 6 Months. Circulation 2017, 135, 2003–2012. [Google Scholar] [CrossRef] [PubMed]
- Coco, V.l.; De Piero, M.E.; Massimi, G.; Chiarini, G.; Raffa, G.M.; Kowalewski, M.; Maessen, J.; Lorusso, R. Right ventricular failure after left ventricular assist device implantation: A review of the literature. J. Thorac. Dis. 2021, 13, 1256–1269. [Google Scholar] [CrossRef] [PubMed]
- Argiriou, M.; Kolokotron, S.-M.; Sakellaridis, T.; Argiriou, O.; Charitos, C.; Zarogoulidis, P.; Katsikogiannis, N.; Kougioumtzi, I.; Machairiotis, N.; Tsiouda, T.; et al. Right heart failure post left ventricular assist device implantation. J. Thorac. Dis. 2014, 6, S52–S59. [Google Scholar] [CrossRef]
- Frankfurter, C.; Molinero, M.; Vishram-Nielsen, J.K.; Foroutan, F.; Mak, S.; Rao, V.; Billia, F.; Orchanian-Cheff, A.; Alba, A.C. Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation. Circ. Heart Fail. 2020, 13, e006994. [Google Scholar] [CrossRef] [PubMed]
- Kormos, R.L.; Teuteberg, J.J.; Pagani, F.D.; Russell, S.D.; John, R.; Miller, L.W.; Massey, T.; Milano, C.A.; Moazami, N.; Sundareswaran, K.S.; et al. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricular assist device: Incidence, risk factors and effect on outcomes. J. Thorac. Cardiovasc. Surg. 2010, 139, 1316–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Paruchuri, V.; Denofrio, D.; Kapur, N.K. Pulmonary Artery Pulsatility Index Is Associated With Right Ventricular Failure After Left Ventricular Assist Device Surgery. J. Card. Fail. 2016, 22, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Hsi, B.; Joseph, D.; Trachtenberg, B.; Bhimaraj, A.; Suarez, E.E.; Xu, J.; Guha, A.; Kim, J.H. Degree of change in right ventricular adaptation measures during axillary Impella support informs risk stratification for early, severe right heart failure following durable LVAD implantation. J. Heart Lung Transplant. 2021, 41, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.H.; Wang, Q.; Yaranov, D.M.; Albert, C.; Wolski, K.; Wagener, J.; Aggarwal, A.; Menon, V.; Jacob, M.; Tang, W.; et al. Dynamic Assessment of Pulmonary Artery Pulsatility Index Provides Incremental Risk Assessment for Early Right Ventricular Failure After Left Ventricular Assist Device. J. Card. Fail. 2021, 27, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, A.N.; Ternus, B.W.; Stulak, J.M.; Clavell, A.L.; Schettle, S.D.; Behfar, A.; Jentzer, J.C. Optimal Hemodynamics and Risk of Severe Outcomes Post-Left Ventricular Assist Device Implantation. ASAIO J. 2021, 68, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.-J.R.; Kiernan, M.S.; Choudhary, G.; Levine, D.J.; Sodha, N.R.; Ehsan, A.; Yousefzai, R. Right Ventricular Failure Post-Implantation of Left Ventricular Assist Device: Prevalence, Pathophysiology and Predictors. ASAIO J. 2019, 66, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Lampert, B.C. Right ventricular failure after left ventricular assist devices. J. Heart Lung Transplant. 2015, 34, 1123–1130. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pre-LVAD | Total | SD/% | No RV Dysfunction | SD/% | RV Dysfunction Optimized | SD/% | RV Dysfunction No Optimized | SD/% | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Demographic | 128 | 100 | 70 | 54.7 | 46 | 35.9 | 12 | 9.4 | |
| Age, y | 57.96 | 12.5 | 60.31 | 11.3 | 54.5 | 14.57 | 57.58 | 7.02 | 0.04 |
| Male | 95 | 74.2 | 53 | 75.71 | 34 | 73.91 | 8 | 66.67 | 0.8 |
| Ischemic Cardiomyopathy | 40 | 31.3 | 26 | 37.14 | 12 | 26.09 | 2 | 16.67 | 0.23 |
| Hypertension | 53 | 41.4 | 33 | 47.14 | 15 | 32.61 | 5 | 41.67 | 0.29 |
| Diabetes | 60 | 46.9 | 34 | 48.57 | 22 | 47.83 | 4 | 33.33 | 0.61 |
| COPD | 19 | 14.8 | 12 | 17.14 | 6 | 13.04 | 1 | 8.33 | 0.66 |
| Chronic Kidney Disease | 45 | 35.2 | 27 | 38.57 | 15 | 32.61 | 3 | 25.00 | 0.59 |
| Stroke | 9 | 7.0 | 3 | 4.29 | 6 | 13.04 | 0 | 0.00 | 0.11 |
| Coronary Artery Disease | 57 | 44.5 | 37 | 52.86 | 16 | 34.78 | 4 | 33.33 | 0.11 |
| CABG | 18 | 14.1 | 11 | 15.71 | 5 | 10.87 | 2 | 16.67 | 0.73 |
| PCI | 40 | 31.3 | 28 | 40.00 | 11 | 23.91 | 1 | 8.33 | 0.03 |
| Peripheral Vascular Disease | 6 | 4.7 | 3 | 4.29 | 3 | 6.52 | 0 | 0.00 | 0.61 |
| VF/VT | 53 | 41.4 | 28 | 40.00 | 21 | 45.65 | 4 | 33.33 | 0.69 |
| AFib/Aflutter | 49 | 38.3 | 25 | 35.71 | 20 | 43.48 | 4 | 33.33 | 0.65 |
| ICD | 104 | 81.3 | 58 | 82.86 | 37 | 80.43 | 9 | 75 | 0.8 |
| Laboratory | |||||||||
| Hemoglobin | 11.32 | 1.93 | 11.4 | 1.87 | 11.2 | 2.08 | 10.87 | 1.78 | 0.63 |
| WBC | 8.46 | 3.17 | 8.2 | 2.87 | 8.8 | 3.44 | 8.5 | 3.91 | 0.59 |
| Platelets | 199.7 | 70.14 | 198 | 68.48 | 204 | 75.12 | 186 | 63.28 | 0.73 |
| Na+ | 135.5 | 4.77 | 136 | 4.38 | 134 | 4.9 | 135 | 5.64 | 0.05 |
| K+ | 4.02 | 0.51 | 3.9 | 0.48 | 4 | 0.57 | 4.2 | 0.31 | 0.28 |
| Creatinine | 1.42 | 0.53 | 1.3 | 0.46 | 1.5 | 0.59 | 1.6 | 0.55 | 0.02 |
| BUN | 29.81 | 17.21 | 27.5 | 13.78 | 30.3 | 17.11 | 41 | 29.28 | 0.03 |
| AST | 62.93 | 208 | 30 | 27.82 | 117 | 340.2 | 38 | 35.76 | 0.08 |
| ALT | 84.71 | 299 | 51 | 171 | 142 | 447.3 | 54 | 66.78 | 0.26 |
| Total Bilirubin | 1.03 | 0.66 | 0.95 | 0.66 | 1.15 | 0.68 | 1.6 | 0.6 | 0.27 |
| Albumin | 3.59 | 0.5 | 3.6 | 0.49 | 3.4 | 0.48 | 3.5 | 0.52 | 0.09 |
| INR | 1.61 | 1.09 | 1.5 | 0.92 | 1.7 | 1.41 | 1.4 | 0.45 | 0.47 |
| Echocardiogram | |||||||||
| LVEF mean (SD) | 13.2 | 10.43 | 12 | 11.66 | 14 | 8.93 | 17 | 6.89 | 0.23 |
| LVEDd mean (SD) | 6.41 | 1.7 | 6.21 | 1.82 | 6.6 | 1.42 | 6.6 | 1.35 | 0.3 |
| Mitral Regurgitation (MR) | 0.78 | ||||||||
| No MR | 15 | 11.7 | 9 | 12.86 | 4 | 8.70 | 2 | 16.67 | 0.68 |
| Mild MR | 48 | 37.5 | 27 | 38.57 | 16 | 34.78 | 5 | 41.67 | 0.87 |
| Moderate MR | 48 | 37.5 | 25 | 35.71 | 18 | 39.13 | 5 | 41.67 | 0.89 |
| Severe MR | 17 | 13.3 | 9 | 12.86 | 8 | 17.39 | 0 | 0.00 | 0.28 |
| Tricuspid Regurgitation (TR) | 0.5 | ||||||||
| No TR | 14 | 10.9 | 9 | 12.86 | 5 | 10.87 | 0 | 0.00 | 0.42 |
| Mild TR | 83 | 64.8 | 48 | 68.57 | 28 | 60.87 | 7 | 58.33 | 0.62 |
| Moderate TR | 29 | 22.7 | 12 | 17.14 | 12 | 26.09 | 5 | 41.67 | 0.13 |
| Severe TR | 2 | 1.6 | 1 | 1.43 | 1 | 2.17 | 0 | 0.00 | 0.85 |
| LVAD Brand | 0.76 | ||||||||
| HVAD | 11 | 8.6 | 7 | 10.00 | 3 | 6.52 | 1 | 8.33 | |
| HeartMate2 | 78 | 60.9 | 40 | 57.14 | 29 | 63.04 | 9 | 75.00 | |
| HeartMate3 | 39 | 30.5 | 23 | 32.86 | 14 | 30.43 | 2 | 16.67 | |
| LVAD Indication | 0.61 | ||||||||
| Bridge to Transplant | 73 | 57.0 | 41 | 58.57 | 24 | 52.17 | 8 | 66.67 | |
| Destination Therapy | 55 | 43.0 | 29 | 41.43 | 22 | 47.83 | 4 | 33.33 | |
| INTERMACS | |||||||||
| INTERMACS 2 | 51 | 39.8 | 19 | 27.14 | 27 | 58.70 | 5 | 41.67 | 0.002 |
| INTERMACS 3 | 64 | 50.0 | 40 | 57.14 | 18 | 39.13 | 6 | 50.00 | 0.16 |
| INTERMACS 4 | 10 | 7.8 | 9 | 12.86 | 0 | 0.00 | 1 | 8.33 | 0.04 |
| INTERMACS 5 | 3 | 2.3 | 2 | 2.86 | 1 | 2.17 | 0 | 0.00 | 0.83 |
| Home Inotrope Pre-LVAD | 59 | 46.1 | 29 | 41.43 | 23 | 50.0 | 7 | 58.33 | 0.44 |
| IABP pre-LVAD | 63 | 49.2 | 25 | 35.71 | 31 | 67.4 | 7 | 58.33 | <0.01 |
| IMPELLA pre-LVAD | 4 | 3.1 | 2 | 2.86 | 2 | 4.3 | 0 | 0.00 | 0.72 |
| Post-Surgery | |||||||||
| Chest open | 20 | 15.6 | 8 | 11.43 | 10 | 21.74 | 2 | 16.67 | 0.32 |
| ECMO post LVAD | 1 | 0.8 | 1 | 1.43 | 0.00 | 0.00 | 0.65 | ||
| Tracheostomy post LVAD | 7 | 5.5 | 3 | 4.29 | 1 | 2.17 | 3 | 25.00 | <0.01 |
| CRRT post LVAD | 7 | 5.5 | 1 | 1.43 | 4 | 8.70 | 2 | 16.67 | 0.04 |
| Optimized Hemodynamic | Total | SD | No RV Dysfunction | SD | RV Dysfunction Optimized | SD | RV Dysfunction Non-Optimized | SD | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| RA mean | 8.82 | 5.35 | 6.98 | 4.16 | 8.73 | 3.67 | 19.83 | 3.66 | <0.01 |
| Delta RA mean | 6.67 | 6.2 | 4.51 | 5.1 | 11.32 | 5.09 | 1.5 | 5.05 | <0.01 |
| PCWP | 20.87 | 6.71 | 21.02 | 7.16 | 19.89 | 6.17 | 23.75 | 5.42 | 0.2 |
| PVR | 2.6 | 1.68 | 2.67 | 1.98 | 2.36 | 1.11 | 3.11 | 1.56 | 0.34 |
| CI Thermo | 2.37 | 0.55 | 2.35 | 0.47 | 2.44 | 0.66 | 2.36 | 0.51 | 0.5 |
| PAPI | 5.09 | 5.58 | 6.38 | 8.87 | 4,14 | 5.26 | 1.25 | 0.35 | <0.01 |
| Delta PAPI | 2.97 | 5.46 | 3.53 | 6.01 | 2.86 | 5.09 | 0.08 | 0.22 | 0.12 |
| RA/PCWP | 0.43 | 0.25 | 0.34 | 0.19 | 0.44 | 0.15 | 0.9 | 0.37 | <0.01 |
| Delta RA/PCWP | 0.11 | 0.24 | 0.1 | 0.19 | 0.2 | 0.18 | −0.16 | 0.4 | <0.01 |
| RVSWI | 657 | 298 | 730 | 315 | 608 | 258 | 416 | 152 | <0.01 |
| Delta RVSWI | 35.36 | 277 | 12.5 | 298 | 132 | 243 | 57 | 157 | 0.01 |
| TPG | 11.81 | 6.61 | 11.9 | 7.71 | 11.2 | 5.12 | 13 | 4.47 | 0.67 |
| DPG | 1.66 | 5.06 | 1.24 | 5.66 | 1.93 | 4.23 | 3 | 4.23 | 0.46 |
| Total | % | Non-RV Dysfunction | % | RV Dysfunction Optimized | % | RV Dysfunction Non-Optimized | % | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Right Ventricular Failure | 51 | 39.8 | 21 | 30.00 | 22 | 47.8 | 8 | 66.67 | 0.02 |
| RVAD | 16 | 12.5 | 6 | 8.57 | 8 | 17.4 | 2 | 16.67 | 0.34 |
| Inotrope > 14 days | 48 | 37.5 | 20 | 28.57 | 21 | 45.7 | 7 | 58.33 | 0.05 |
| Inotrope > 21 days | 31 | 24.2 | 15 | 21.43 | 12 | 26.1 | 4 | 33.33 | 0.63 |
| 12 Months Mortality | 17 | 13.3 | 8 | 11.43 | 4 | 8.7 | 5 | 41.67 | <0.01 |
| 24 Months Mortality | 28 | 21.9 | 17 | 24.29 | 6 | 13.0 | 5 | 41.67 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duque, E.R.; Alvarez, P.; Yang, Y.; Khalid, M.; Kshetri, R.; Doulamis, I.P.; Panos, A.; Briasoulis, A. Impact of Pre-Operative Right Ventricular Response to Hemodynamic Optimization on Outcomes in Patients with LVADs. J. Clin. Med. 2022, 11, 6111. https://doi.org/10.3390/jcm11206111
Duque ER, Alvarez P, Yang Y, Khalid M, Kshetri R, Doulamis IP, Panos A, Briasoulis A. Impact of Pre-Operative Right Ventricular Response to Hemodynamic Optimization on Outcomes in Patients with LVADs. Journal of Clinical Medicine. 2022; 11(20):6111. https://doi.org/10.3390/jcm11206111
Chicago/Turabian StyleDuque, Ernesto Ruiz, Paulino Alvarez, Yingchi Yang, Muhammad Khalid, Rupesh Kshetri, Ilias P. Doulamis, Anthony Panos, and Alexandros Briasoulis. 2022. "Impact of Pre-Operative Right Ventricular Response to Hemodynamic Optimization on Outcomes in Patients with LVADs" Journal of Clinical Medicine 11, no. 20: 6111. https://doi.org/10.3390/jcm11206111