
Custom-Made 3D-Printed Implants for Anterior Column Reconstruction in the Upper Cervical Spine after Intralesional Extracapsular Excision—Report of 2 Cases and Literature Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Design of the Implant
3. Results
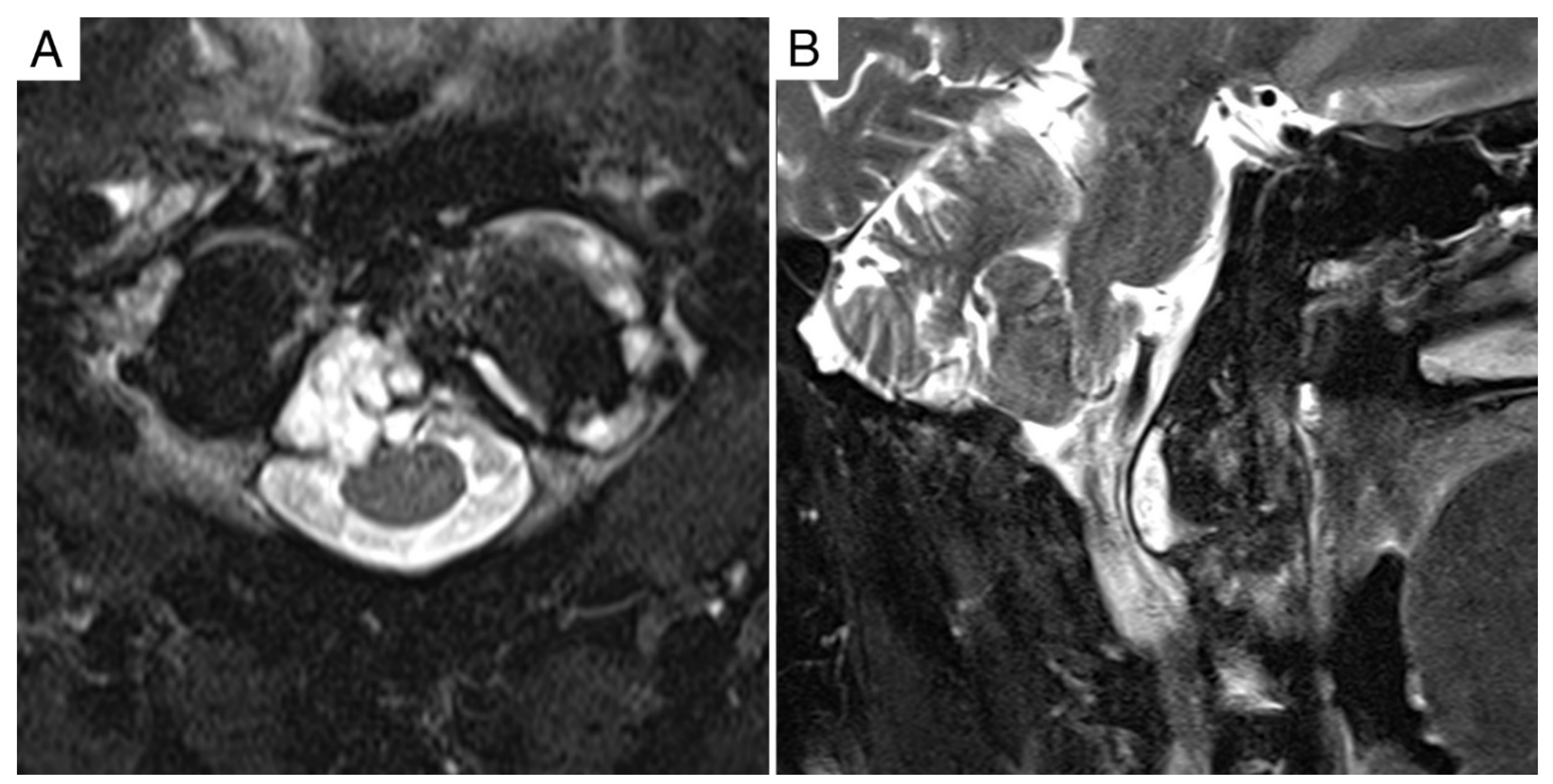
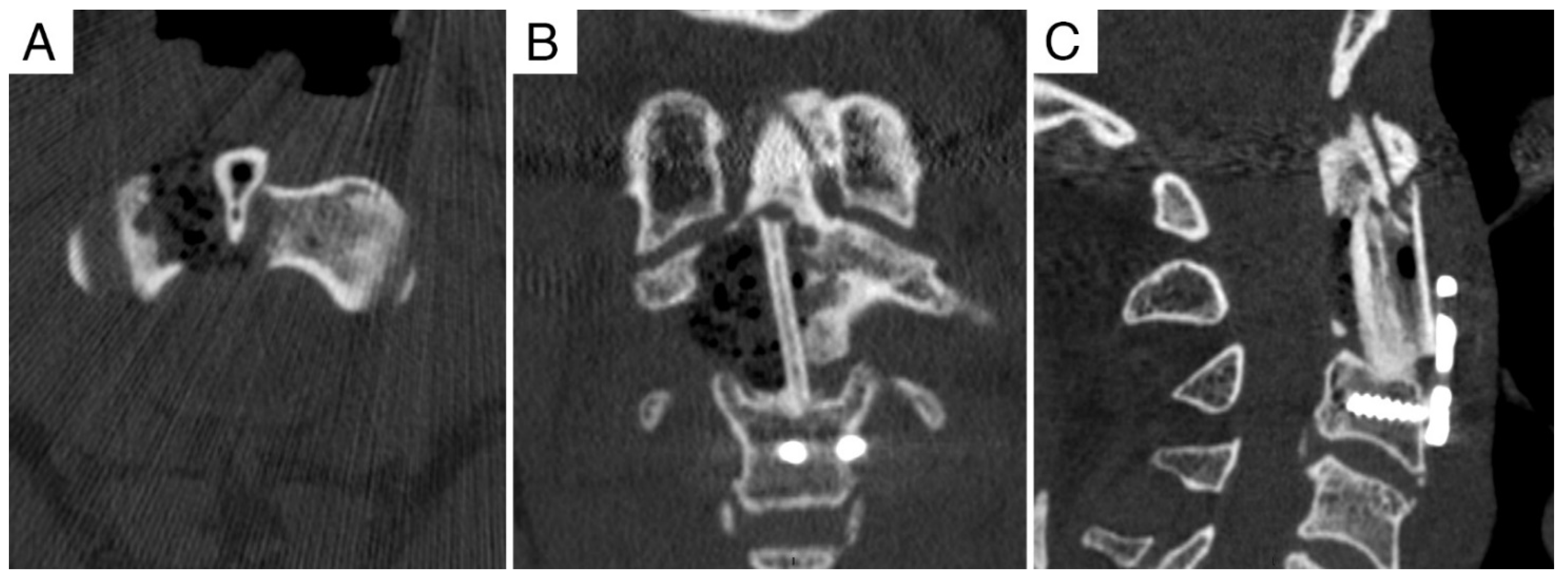
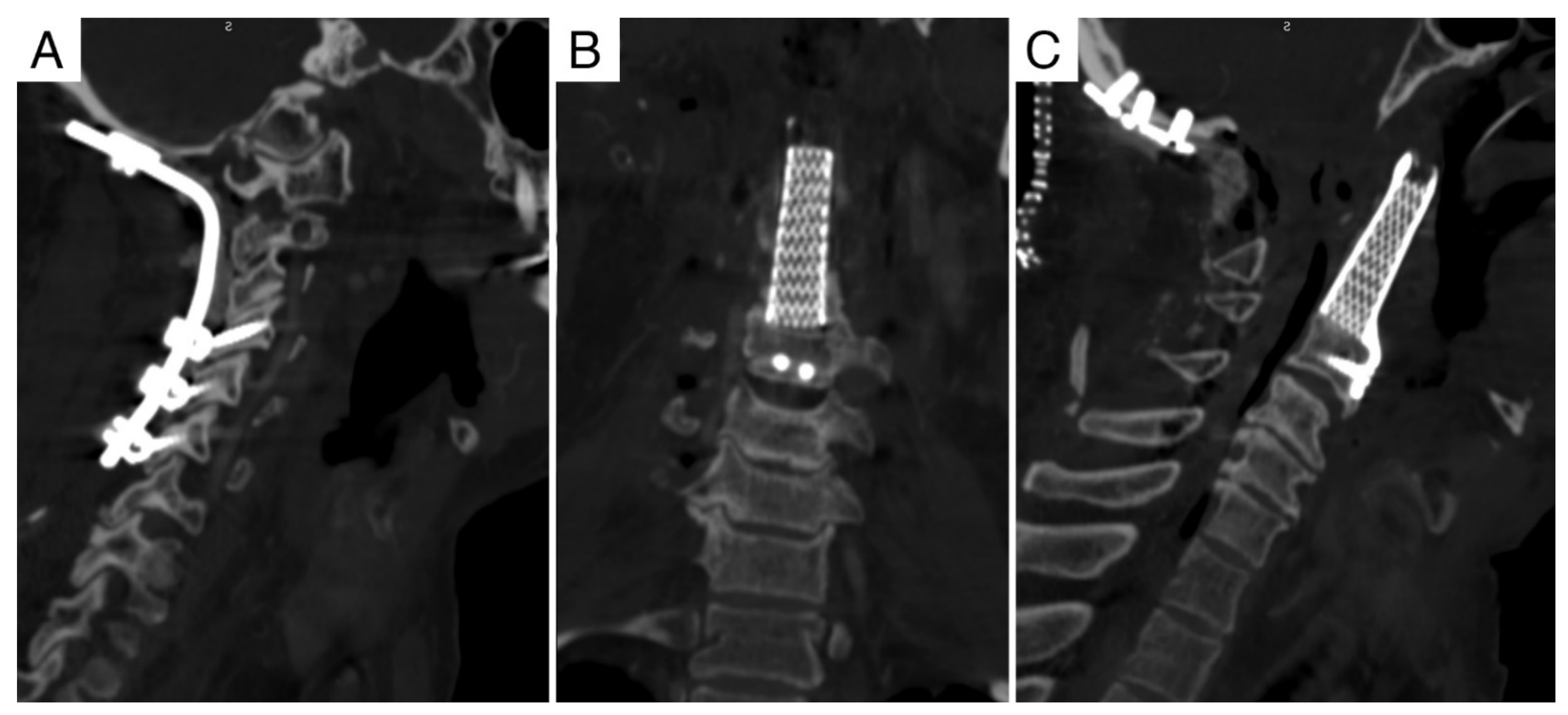
3.1. Case Report 1
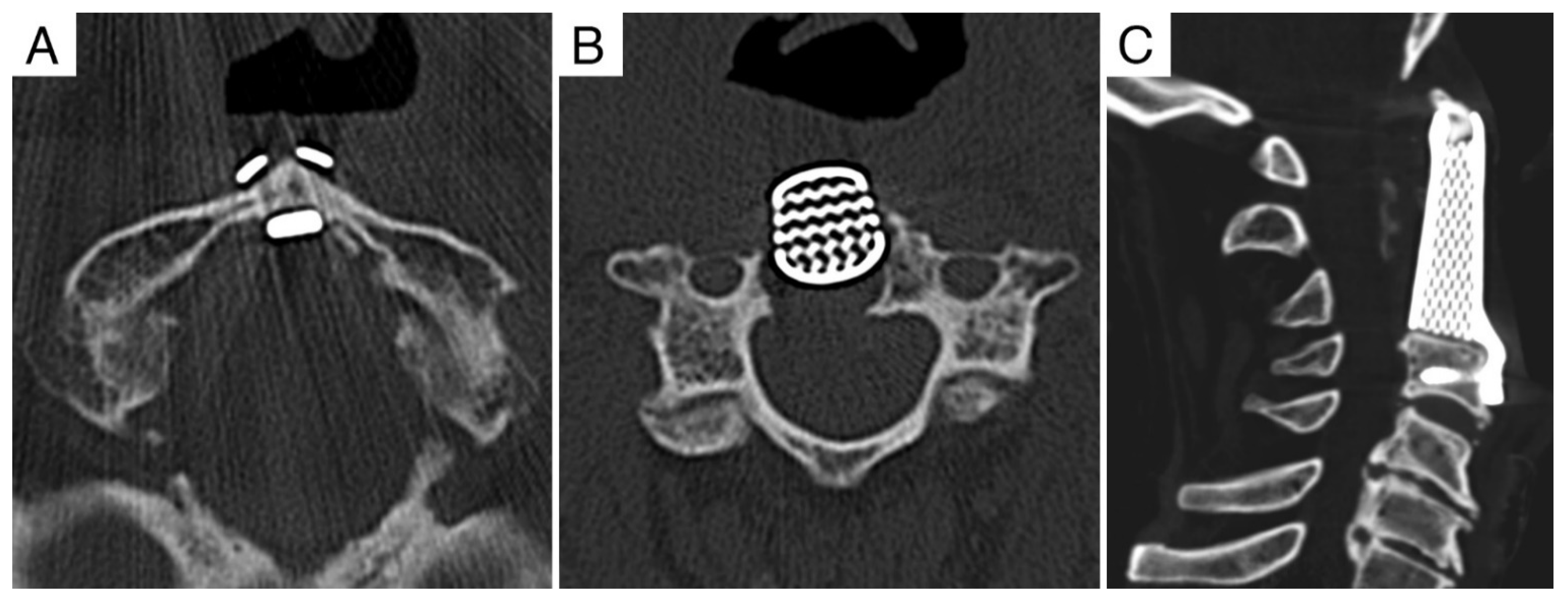
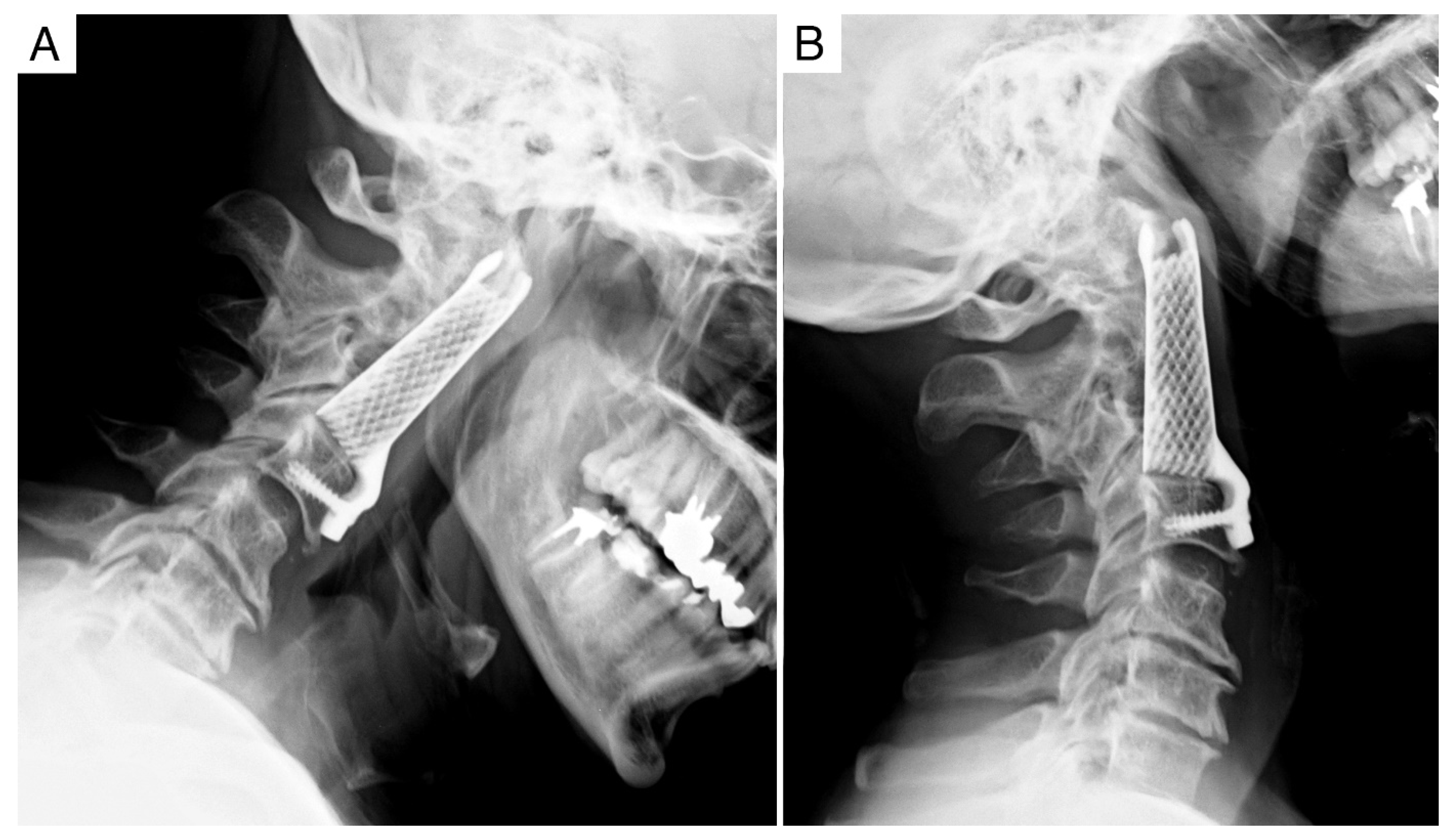
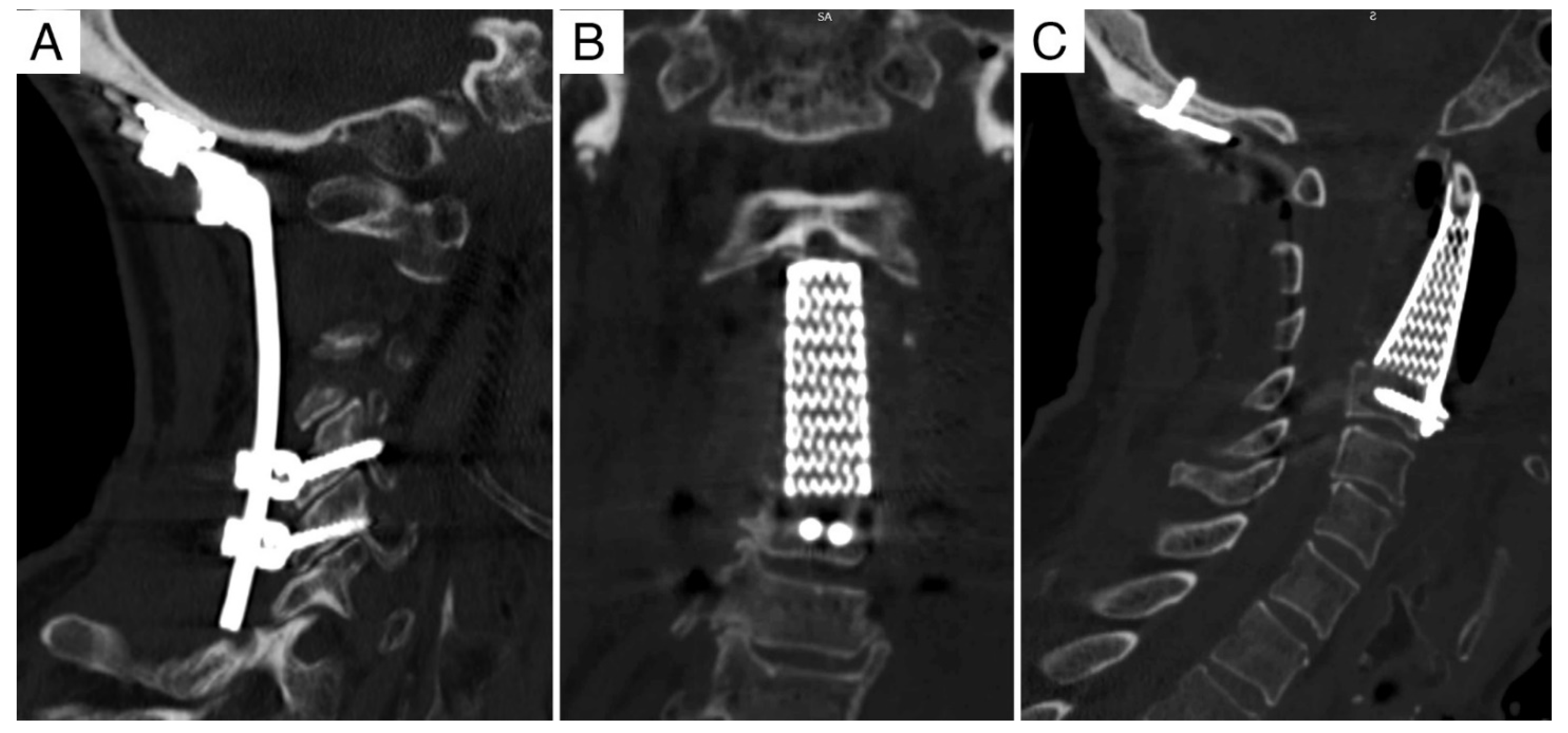
3.2. Case Report 2
3.3. Reconstruction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Girolami, M.; Sartori, M.; Bandiera, S.; Barbanti-Brodano, G.; Evangelisti, G.; Ghermandi, R.; Pipola, V.; Tedesco, G.; Terzi, S.; Asunis, E.; et al. 3D Vertebral Prosthesis. In 3D Printing in Bone Surgery; Zoccali, C., Ruggeri, P., Benazzo, F., Eds.; Springer Nature: Basel, Switzerland, 2022; pp. 97–104. [Google Scholar]
- Girolami, M.; Boriani, S.; Bandiera, S.; Barbanti-Bródano, G.; Ghermandi, R.; Terzi, S.; Tedesco, G.; Evangelisti, G.; Pipola, V.; Gasbarrini, A. Biomimetic 3D-printed custom-made prosthesis for anterior column reconstruction in the thoracolumbar spine: A tailored option following en bloc resection for spinal tumors: Preliminary results on a case-series of 13 patients. Eur. Spine J. 2018, 27, 3073–3083. [Google Scholar] [CrossRef]
- Tenny, S.; Varacallo, M. Chordoma. In WHO Classification of Tumours, Soft Tissue and Bone Tumours, 5th ed.; Statpearls Publishing: Tampa, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430846/ (accessed on 12 February 2022).
- McAfee, P.C.; Bohlman, H.H.; Riley, L.H., Jr.; Robinson, R.A.; Southwick, W.O.; Nachlas, N.E. The anterior retropharyngeal approach to the upper part of the cervical spine. J. Bone Jt. Surg. Am. 1987, 69, 1371–1383. [Google Scholar]
- Singh, P.K.; Agrawal, M.; Mishra, S.; Agrawal, D.; Sawarkar, D.; Jagdevan, A.; Verma, S.; Doddamani, R.; Meena, R.; Garg, K.; et al. Management of C2 Body Giant Cell Tumor by Innovatively Fashioned Iliac Crest Graft and Modified Cervical Mesh Cage Used as Plate. World Neurosurg. 2020, 140, 241–246. [Google Scholar] [CrossRef]
- Yang, J.; Yang, X.H.; He, S.H.; Jiao, J.; Jia, Q.; Hu, J.B.; Xiao, J.R. A Novel Reconstruction Using a Combined Anterior and Posterior Approach After Axis Tumor Spondylectomy. Clin. Spine Surg. 2020, 33, E299–E306. [Google Scholar] [CrossRef]
- Suchomel, P.; Buchvald, P.; Barsa, P.; Froehlich, R.; Choutka, O.; Krejzar, Z.; Sourkova, P.; Endrych, L.; Dzan, L. Single-stage total C-2 intralesional spondylectomy for chordoma with three-column reconstruction. Technical note. J. Neurosurg. Spine 2007, 6, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Kaltoft, B.; Kruse, A.; Jensen, L.T.; Elberg, J.J. Reconstruction of the cervical spine with two osteocutaneous fibular flap after radiotherapy and resection of osteoclastoma: A case report. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1262–1264. [Google Scholar] [CrossRef]
- Xu, N.; Wei, F.; Liu, X.; Jiang, L.; Cai, H.; Li, Z.; Yu, M.; Wu, F.; Liu, Z. Reconstruction of the Upper Cervical Spine Using a Personalized 3D-Printed Vertebral Body in an Adolescent with Ewing Sarcoma. Spine 2016, 41, E50–E54. [Google Scholar] [CrossRef]
- Li, X.; Wang, Y.; Zhao, Y.; Liu, J.; Xiao, S.; Mao, K. Multilevel 3D Printing Implant for Reconstructing Cervical Spine with Metastatic Papillary Thyroid Carcinoma. Spine 2017, 42, E1326–E1330. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Thompson, R.; Sutterlin, I.I.I.C.E.; Phan, K. The utility of 3D printing for surgical planning and patient-specific implant design for complex spinal pathologies: Case report. J. Neurosurg. Spine 2017, 26, 513–518. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Yang, X.; Yang, J.; Ye, C.; Liu, W.; Wei, H.; Xiao, J. Customized “Whole-Cervical-Vertebral-Body” Reconstruction After Modified Subtotal Spondylectomy of C2-C7 Spinal Tumor Via Piezoelectric Surgery. Oper. Neurosurg. 2019, 17, 580–587. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Ye, C.; Zhong, N.; Yang, M.; Yang, X.; Xiao, J. Customized anterior craniocervical reconstruction via a modified high-cervical retropharyngeal approach following resection of a spinal tumor involving C1-2/C1-3. J. Neurosurg. Spine 2019, 32, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Parr, W.C.H.; Burnard, J.L.; Singh, T.; McEvoy, A.; Walsh, W.R.; Mobbs, R.J. C3-C5 Chordoma Resection and Reconstruction with a Three-Dimensional Printed Titanium Patient-Specific Implant. World Neurosurg. 2020, 136, 226–233. [Google Scholar] [CrossRef]
- Li, Y.; Zheng, G.; Liu, T.; Liang, Y.; Huang, J.; Liu, X.; Huang, J.; Cheng, Z.; Lu, S.; Huang, L. Surgical Resection of Solitary Bone Plasmacytoma of Atlas and Reconstruction with 3-Dimensional-Printed Titanium Patient-Specific Implant. World Neurosurg. 2020, 139, 322–329. [Google Scholar] [CrossRef]
- Wei, F.; Li, Z.; Liu, Z.; Liu, X.; Jiang, L.; Yu, M.; Xu, N.; Wu, F.; Dang, L.; Zhou, H.; et al. Upper cervical spine reconstruction using customized 3D-printed vertebral body in 9 patients with primary tumors involving C2. Ann. Transl. Med. 2020, 8, 332. [Google Scholar] [CrossRef]
- Yang, X.; Wan, W.; Gong, H.; Xiao, J. Application of Individualized 3D-Printed Artificial Vertebral Body for Cervicothoracic Reconstruction in a Six-Level Recurrent Chordoma. Turk. Neurosurg. 2020, 30, 149–155. [Google Scholar] [CrossRef]
- Hunn, S.A.M.; Koefman, A.J.; Hunn, A.W.M. AWM. 3D-printed Titanium Prosthetic Reconstruction of the C2 Vertebra: Techniques and Outcomes of Three Consecutive Cases. Spine 2020, 45, 667–672. [Google Scholar] [CrossRef]
- Baldassarre, B.M.; Di Perna, G.; Portonero, I.; Penner, F.; Cofano, F.; Marco, R.; Marengo, N.; Garbossa, D.; Pecorari, G.; Zenga, F. Craniovertebral junction chordomas: Case series and strategies to overcome the surgical challenge. J. Craniovertebr. Junction Spine 2021, 12, 420–431. [Google Scholar]
- Lannon, M.; Algird, A.; Alsunbul, W.; Wang, B.H. Cost-Effective Cranioplasty Utilizing 3D Printed Molds: A Canadian Single-Center Experience. Can. J. Neurol. Sci. 2022, 49, 196–202. [Google Scholar] [CrossRef]
- Czyżewski, W.; Jachimczyk, J.; Hoffman, Z.; Szymoniuk, M.; Litak, J.; Maciejewski, M.; Kura, K.; Rola, R.; Torres, K. Low-Cost Cranioplasty-A Systematic Review of 3D Printing in Medicine. Materials 2022, 15, 4731. [Google Scholar] [CrossRef]
- Park, C.K. 3D-Printed Disease Models for Neurosurgical Planning, Simulation, and Training. J. Korean Neurosurg. Soc. 2022, 65, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Błaszczyk, M.; Jabbar, R.; Szmyd, B.; Radek, M. 3D Printing of Rapid, Low-Cost and Patient-Specific Models of Brain Vasculature for Use in Preoperative Planning in Clipping of Intracranial Aneurysms. J. Clin. Med. 2021, 10, 1201. [Google Scholar] [CrossRef]
- Garcia, J.; Yang, Z.; Mongrain, R.; Leask, R.L.; Lachapelle, K. 3D printing materials and their use in medical education: A review of current technology and trends for the future. BMJ Simul. Technol. Enhanc. Learn. 2018, 4, 27–40. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years), Sex | Diagnosis | Enneking | WBB | Previous Treatments | Approach | Margin | Local Control (Months) | Overall Survival (Months) | Oncological Status |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 65, M | Recurrent chordoma C2 | IB | 8-5/A-D | RT (70.4 Gy carbon-ion, Δt = 4 y) Extracapsular debulking and reconstruction w/ allograft and carbon-fiber buttress plate (Δt = 2 y) | A | Intralesional | 18 | 20 | DOC |
| 2 | 75, M | Recurrent chordoma C2 | IB | 8-3/A-D | Extracapsular debulking (Δt = 8 m) RT (74 Gy proton-ion, Δt = 2 m) | A+P | Intralesional | 12 | 32 | DOD |
| Authors | Year | Article Type | n | Diagnosis | Age, Sex | Previous Treatments | Surgical Treatment | Approach | Adjuvant Treatments | Proximal Fixation | Distal Fixation | Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Xu N et al. [9] | 2016 | Case report | 1 | C2 Ewing sarcoma | 12, M | None | Single-level (C2) IL spondylectomy | P (C0-C6) + A (extraoral retropharyngeal) staged (2 weeks) | CHT + RT | Divergent TI-screws in C1 lateral masses | Titanium wiring in DVB (C3; TI-screws insertion not possible) | 1 year | |
| Li X et al. [10] | 2017 | Case report | 1 | C2-C3-C4 thyroid ca. metastasis | 53, F | None | 3-level (C2-C4) IL corpectomy + thyroidectomy and lateral lymph nodes dissection | A and P (C1-C6) | Radioiodine I131 | Divergent TI-screws in C1 lateral masses | 2 TI-screws in DVB (C5) | 1 year | |
| Mobbs RJ et al. [11] | 2017 | Case report | 1 | C1-C2 chordoma | 63, M | CT-guided transoral biopsy | 2-level (C1-C2) IL excision | P (C0-C3) and A (transoral) | RT | 2 TiP-screws in the clivus | 2 TI-screws in DVB (C3) | 9 months | |
| He S et al. [12] | 2019 | Case report | 1 | C2-C7 chondrosarcoma | 27 | Posterior open biopsy | 6-level (C2-C7) IL en bloc resection | P (C0-T2) and A (retropharyngeal) staged (1 week) | Local cisplatinum intra-op. | Divergent TI-screws in C1 lateral masses | 2 TiP-screws in DVB (T1) | 14 months | |
| He S et al. [13] | 2019 | Case series | 7 | C1-C3 (4 patients) C1-C2 (3 patients) | Average 47.6 ± 19.0 (range 12–72) | - - - | Multi-level IL spondylectomy (4 3-level, 3 2-level) | P and A (retropharyngeal) staged | - - - | TI-screws in occipital condyles | 2 TiP-screws in DVB | Average 14.8 (range 7.3–24.2) | |
| |||||||||||||
| Parr WHC et al. [14] | 2020 | Case report | 1 | C3-C4-C5 chordoma | 45, M | CT-guided biopsy | 3-level IL spondylectomy | P (C2-C6) and A staged (3 days) | RT (proton-beam) | 2 TI-screws in C2 | 2 TI-screws in DVB (C6) | 17 months | |
| Li Y et al. [15] | 2020 | Case report | 1 | C1 plasmocytoma | 57, M | CT-guided transoral biopsy | IL tumor debulking | A (retropharyngeal) and P (C0-C3) | RT (57 Gy/27 ft.) | 1 TI-screw in occipital condyle | 1 TI- and 1 TiP-screw in DVB (C2) | (Not reported) | |
| Wei F et al. [16] | 2020 | Case series | 9 | 7 C2 2 C2-C3 | Average 31.4 (range 12–59) | CT-guided biopsy | Single- and multi-level IL spondylectomy | P (4 cases to C0, 5 to C1) and A (retropharyngeal) staged (average 14.4 days) | RT, CHT (in 2 cases) | Divergent TI-screws in C1 lateral masses | 2 TiP-screws in DVB (not possible in 2 cases) | Average 28.6 (range 12–42) | |
| |||||||||||||
| Yang X et al. [17] | 2020 | Case report | 1 | C3-C4-C5-C6-C7-T1 chordoma | 40, F | 2 tumor debulkings | 6-level IL extracapsular excision | A (retropharyngeal) and P (C1-T3) | None | 3 TiP-screws in vertebral body of C2 | 3 TiP-screws in DVB (T2) | 9 months | |
| Hunn SAM et al. [18] | 2020 | Case report | 2 | C2 thyroid ca. metastasis | 56, F | None | Single-level (C2) IL corpectomy | A (retropharyngeal) | and P (C1-C3) | RT and CHT | 2 TiP-screws in C1 lateral masses | 3 TiP-screws in DVB (C3) | 14 months |
| C2-C3 myeloma | 63, M | None | 2-level (C2-C3) IL corpectomy | and P (C1-C4) | (Not reported) | 3 TiP-screws in DVB (C4) | 4 months | ||||||
| Baldassarre BM et al. [19] | 2021 | Case report | 1 | C1-C2 chordoma | 45 | Biopsy | IL excision | P (C0-C4) and A (retropharyngeal) staged (1 day) | RT (proton beam) | Saddle for anterior arch of C1 | 2 TiP-screws in DVB (C3) | 12 months | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girolami, M.; Griffoni, C.; Asunis, E.; Falzetti, L.; Bandiera, S.; Barbanti Brodano, G.; Ghermandi, R.; Pipola, V.; Terzi, S.; Pesce, E.; et al. Custom-Made 3D-Printed Implants for Anterior Column Reconstruction in the Upper Cervical Spine after Intralesional Extracapsular Excision—Report of 2 Cases and Literature Review. J. Clin. Med. 2022, 11, 6058. https://doi.org/10.3390/jcm11206058
Girolami M, Griffoni C, Asunis E, Falzetti L, Bandiera S, Barbanti Brodano G, Ghermandi R, Pipola V, Terzi S, Pesce E, et al. Custom-Made 3D-Printed Implants for Anterior Column Reconstruction in the Upper Cervical Spine after Intralesional Extracapsular Excision—Report of 2 Cases and Literature Review. Journal of Clinical Medicine. 2022; 11(20):6058. https://doi.org/10.3390/jcm11206058
Chicago/Turabian StyleGirolami, Marco, Cristiana Griffoni, Emanuela Asunis, Luigi Falzetti, Stefano Bandiera, Giovanni Barbanti Brodano, Riccardo Ghermandi, Valerio Pipola, Silvia Terzi, Eleonora Pesce, and et al. 2022. "Custom-Made 3D-Printed Implants for Anterior Column Reconstruction in the Upper Cervical Spine after Intralesional Extracapsular Excision—Report of 2 Cases and Literature Review" Journal of Clinical Medicine 11, no. 20: 6058. https://doi.org/10.3390/jcm11206058