
Autoimmune Thyroid Disorders Are More Prevalent in Patients with Celiac Disease: A Retrospective Case-Control Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Eligibility
2.2. Data Collection
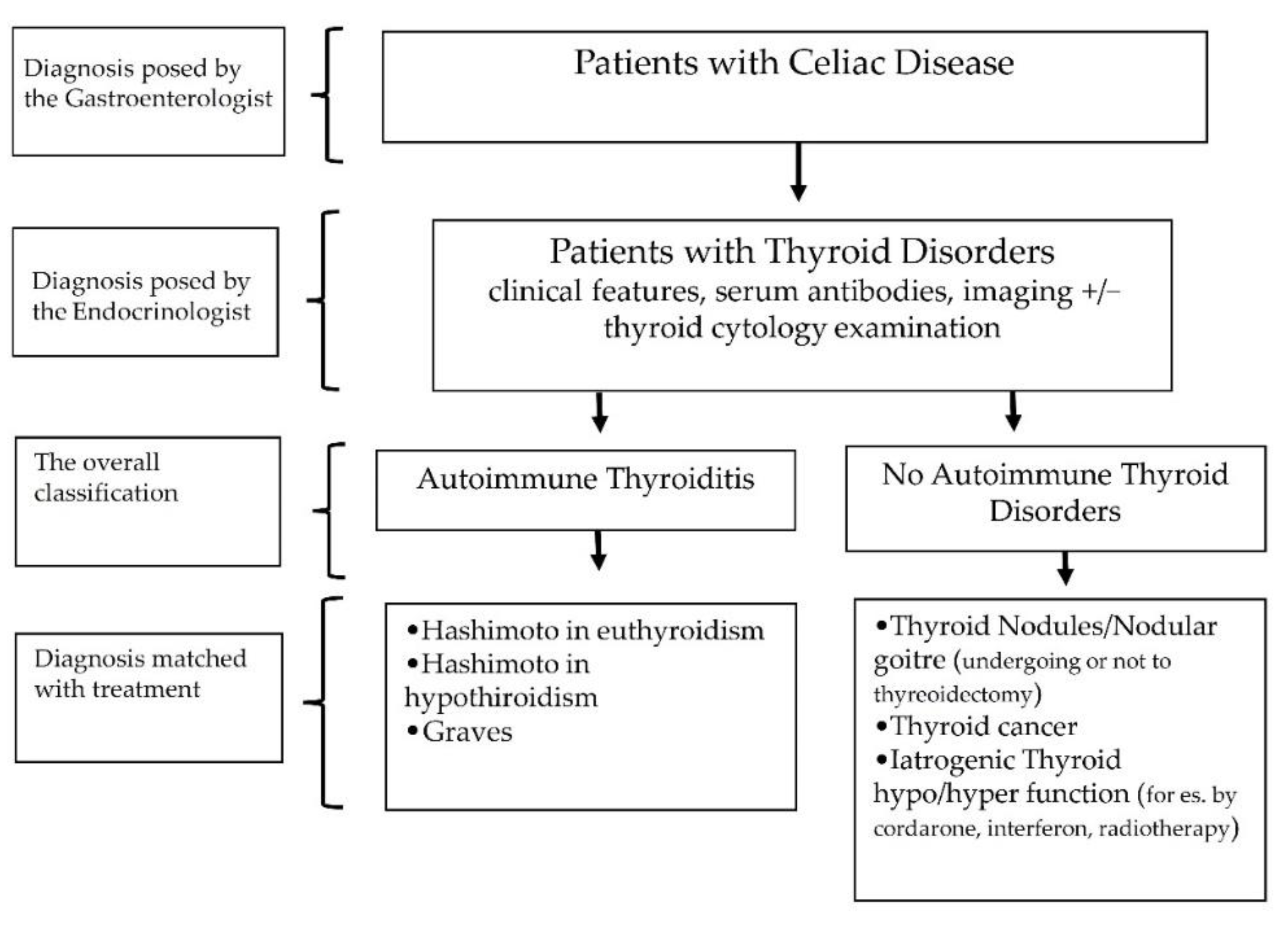
2.3. Diagnosis
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Green, P.H.; Lebwohl, B.; Greywoode, R. Celiac disease. J. Allergy Clin. Immunol. 2015, 135, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Sanders, D.S.; Green, P.H.R. Celiac disease. Lancet 2018, 391, 70–81. [Google Scholar] [CrossRef]
- Silano, M.; Agostoni, C.; Sanz, Y.; Guandalini, S. Infant feeding and risk of developing celiac disease: A systematic review. BMJ Open 2016, 6, e009163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbo, S.; Pes, G.M.; Dore, M.P. Coeliac disease from pathogenesis to clinical practice: Current concepts. Recenti Prog. Med. 2020, 111, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Green, P.H.; Murray, J.A.; Ludvigsson, J.F. Season of birth in a nationwide cohort of coeliac disease patients. Arch. Dis. Child. 2013, 98, 48–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pes, G.M.; Bibbo, S.; Dore, M.P. Coeliac disease: Beyond genetic susceptibility and gluten. A narrative review. Ann. Med. 2019, 51, 1–16. [Google Scholar] [CrossRef]
- Tanpowpong, P.; Camargo, C.A. Early-life vitamin D deficiency and childhood-onset coeliac disease. Public Health Nutr. 2014, 17, 823–826. [Google Scholar] [CrossRef] [Green Version]
- Crosby, W.H.; Kugler, H.W. Intraluminal biopsy of the small intestine; the intestinal biopsy capsule. Am. J. Dig. Dis. 1957, 2, 236–241. [Google Scholar] [CrossRef]
- Catassi, C.; Fabiani, E.; Ratsch, I.M.; Coppa, G.V.; Giorgi, P.L.; Pierdomenico, R.; Alessandrini, S.; Iwanejko, G.; Domenici, R.; Mei, E.; et al. The coeliac iceberg in Italy. A multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Acta Paediatr. Suppl. 1996, 412, 29–35. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e822. [Google Scholar] [CrossRef]
- Meloni, G.; Dore, A.; Fanciulli, G.; Tanda, F.; Bottazzo, G.F. Subclinical coeliac disease in schoolchildren from northern Sardinia. Lancet 1999, 353, 37. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dore, M.P.; Cuccu, M.; Pes, G.M.; Mameli, L.; Manca, A.; Vidili, G.; Togniotti, E. Clinical pattern of celiac disease in a population residing in North Sardinia (Italy). Recenti Prog. Med. 2012, 103, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Berti, I.; Gerarduzzi, T.; Not, T.; Colletti, R.B.; Drago, S.; Elitsur, Y.; Green, P.H.; Guandalini, S.; Hill, I.D.; et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch. Intern. Med. 2003, 163, 286–292. [Google Scholar] [CrossRef]
- Bibbo, S.; Pes, G.M.; Usai-Satta, P.; Salis, R.; Soro, S.; Quarta Colosso, B.M.; Dore, M.P. Chronic autoimmune disorders are increased in coeliac disease: A case-control study. Medicine 2017, 96, e8562. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; De Giorgio, R.; Granito, A.; Stanghellini, V.; Barbara, G.; Avoni, P.; Liguori, R.; Petrolini, N.; Fiorini, E.; Montagna, P.; et al. Anti-ganglioside antibodies in coeliac disease with neurological disorders. Dig. Liver Dis. 2006, 38, 183–187. [Google Scholar] [CrossRef]
- Zauli, D.; Grassi, A.; Granito, A.; Foderaro, S.; De Franceschi, L.; Ballardini, G.; Bianchi, F.B.; Volta, U. Prevalence of silent coeliac disease in atopics. Dig. Liver Dis. 2000, 32, 775–779. [Google Scholar] [CrossRef]
- Badenhoop, K.; Dieterich, W.; Segni, M.; Hofmann, S.; Hufner, M.; Usadel, K.H.; Hahn, E.G.; Schuppan, D. HLA DQ2 and/or DQ8 is associated with celiac disease-specific autoantibodies to tissue transglutaminase in families with thyroid autoimmunity. Am. J. Gastroenterol. 2001, 96, 1648–1649. [Google Scholar] [CrossRef]
- Kaukinen, K.; Collin, P.; Mykkanen, A.H.; Partanen, J.; Maki, M.; Salmi, J. Celiac disease and autoimmune endocrinologic disorders. Dig. Dis. Sci. 1999, 44, 1428–1433. [Google Scholar] [CrossRef]
- Lorini, R.; Larizza, D.; Scotta, M.S.; Severi, F. HLA in Graves’ disease coexistent with coeliac disease. Eur. J. Pediatr. 1986, 145, 241. [Google Scholar] [CrossRef]
- Vanderpump, M.P.; Tunbridge, W.M.; French, J.M.; Appleton, D.; Bates, D.; Clark, F.; Grimley Evans, J.; Hasan, D.M.; Rodgers, H.; Tunbridge, F.; et al. The incidence of thyroid disorders in the community: A twenty-year follow-up of the Whickham Survey. Clin. Endocrinol. 1995, 43, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.L.; Gange, S.J.; Rose, N.R.; Graham, N.M. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin. Immunol. Immunopathol. 1997, 84, 223–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Lu, L.; Yang, R.; Li, Y.; Shan, L.; Wang, Y. Increased Incidence of Thyroid Disease in Patients with Celiac Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0168708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current guidelines for the management of celiac disease: A systematic review with comparative analysis. World J. Gastroenterol. 2022, 28, 154–175. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Cocco, E.; Mereu, A.; Massa, R.; Cuccu, A.; Marrosu, M.G.; Contu, P. Population based study of 12 autoimmune diseases in Sardinia, Italy: Prevalence and comorbidity. PLoS ONE 2012, 7, e32487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assa, A.; Frenkel-Nir, Y.; Tzur, D.; Katz, L.H.; Shamir, R. Large population study shows that adolescents with celiac disease have an increased risk of multiple autoimmune and nonautoimmune comorbidities. Acta Paediatr. 2017, 106, 967–972. [Google Scholar] [CrossRef]
- Guariso, G.; Plebani, M.; Signorini, R.; Brigato, L.; Nichetti, C.; Celadin, M.; Gobber, D.; Pittoni, M.; Zacchello, F. Silent celiac disease: Results of a study in secondary schools of Padua. Pediatr. Med. Chir. 1997, 19, 95–98. [Google Scholar]
- Meloni, A.; Mandas, C.; Jores, R.D.; Congia, M. Prevalence of autoimmune thyroiditis in children with celiac disease and effect of gluten withdrawal. J. Pediatr. 2009, 155, 51–55.e51. [Google Scholar] [CrossRef]
- Dore, M.P.; Soro, S.; Niolu, C.; Longo, N.P.; Bibbo, S.; Manca, A.; Pes, G.M. Clinical features and natural history of idiopathic peptic ulcers: A retrospective case-control study. Scand. J. Gastroenterol. 2019, 54, 1315–1321. [Google Scholar] [CrossRef]
- Pes, G.M.; Ganau, A.; Tognotti, E.; Errigo, A.; Rocchi, C.; Dore, M.P. The association of adult height with the risk of cardiovascular disease and cancer in the population of Sardinia. PLoS ONE 2018, 13, e0190888. [Google Scholar] [CrossRef] [PubMed]
- Bibbo, S.; Fozza, C.; Pes, G.M.; Rojas, R.; Manetti, R.; Dore, M.P. Increased Frequency of Immune Thrombocytopenic Purpura in Coeliac Disease and Vice Versa: A Prospective Observational Study. Gastroenterol. Res. Pract. 2018, 2018, 4138434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lampis, R.; Morelli, L.; De Virgiliis, S.; Congia, M.; Cucca, F. The distribution of HLA class II haplotypes reveals that the Sardinian population is genetically differentiated from the other Caucasian populations. Tissue Antigens 2000, 56, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Congia, M.; Clemente, M.G.; Dessi, C.; Cucca, F.; Mazzoleni, A.P.; Frau, F.; Lampis, R.; Cao, A.; Lai, M.E.; De Virgiliis, S. HLA class II genes in chronic hepatitis C virus-infection and associated immunological disorders. Hepatology 1996, 24, 1338–1341. [Google Scholar] [CrossRef] [PubMed]
- Viljamaa, M.; Collin, P.; Huhtala, H.; Sievanen, H.; Maki, M.; Kaukinen, K. Is coeliac disease screening in risk groups justified? A fourteen-year follow-up with special focus on compliance and quality of life. Aliment. Pharmacol. Ther. 2005, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Shin, S.W. Overdiagnosis and screening for thyroid cancer in Korea. Lancet 2014, 384, 1848. [Google Scholar] [CrossRef] [Green Version]
- Sategna-Guidetti, C.; Volta, U.; Ciacci, C.; Usai, P.; Carlino, A.; De Franceschi, L.; Camera, A.; Pelli, A.; Brossa, C. Prevalence of thyroid disorders in untreated adult celiac disease patients and effect of gluten withdrawal: An Italian multicenter study. Am. J. Gastroenterol. 2001, 96, 751–757. [Google Scholar] [CrossRef]
- Fasano, A. Systemic autoimmune disorders in celiac disease. Curr. Opin. Gastroenterol. 2006, 22, 674–679. [Google Scholar] [CrossRef]
- Beyi, A.F.; Hassall, A.; Phillips, G.J.; Plummer, P.J. Tracking Reservoirs of Antimicrobial Resistance Genes in a Complex Microbial Community Using Metagenomic Hi-C: The Case of Bovine Digital Dermatitis. Antibiotics 2021, 10, 221. [Google Scholar] [CrossRef]
- Illiano, P.; Brambilla, R.; Parolini, C. The mutual interplay of gut microbiota, diet and human disease. FEBS J. 2020, 287, 833–855. [Google Scholar] [CrossRef] [Green Version]
- Lundin, K.E.; Kelly, C.P.; Sanders, D.S.; Chen, K.; Kayaniyil, S.; Wang, S.; Wani, R.J.; Barrett, C.; Yoosuf, S.; Pettersen, E.S.; et al. Understanding celiac disease monitoring patterns and outcomes after diagnosis: A multinational, retrospective chart review study. World J. Gastroenterol. 2021, 27, 2603–2614. [Google Scholar] [CrossRef]
- Ventura, A.; Magazzu, G.; Greco, L. Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. SIGEP Study Group for Autoimmune Disorders in Celiac Disease. Gastroenterology 1999, 117, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Schuppan, D. Current concepts of celiac disease pathogenesis. Gastroenterology 2000, 119, 234–242. [Google Scholar] [CrossRef]
- Lehmann, D.; Ben-Nun, A. Bacterial agents protect against autoimmune disease. I. Mice pre-exposed to Bordetella pertussis or Mycobacterium tuberculosis are highly refractory to induction of experimental autoimmune encephalomyelitis. J. Autoimmun. 1992, 5, 675–690. [Google Scholar] [CrossRef]
- Di Mario, U.; Anastasi, E.; Mariani, P.; Ballati, G.; Perfetti, R.; Triglione, P.; Morellini, M.; Bonamico, M. Diabetes-related autoantibodies do appear in children with coeliac disease. Acta Paediatr. 1992, 81, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Toscano, V.; Conti, F.G.; Anastasi, E.; Mariani, P.; Tiberti, C.; Poggi, M.; Montuori, M.; Monti, S.; Laureti, S.; Cipolletta, E.; et al. Importance of gluten in the induction of endocrine autoantibodies and organ dysfunction in adolescent celiac patients. Am. J. Gastroenterol. 2000, 95, 1742–1748. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | No Thyroid Disease (n = 7312) | Thyroid Disease (n = 1177) |
|---|---|---|
| Sex, n (%) | ||
| Female | 4437 (80.8) | 1053 (19.2) ** |
| Male | 2875 (95.9) | 124 (4.1) |
| Age, mean ± SD | 51.67 ± 17.52 | 54.78 ± 15.23 |
| Area, n (%) | ||
| Urban | 3705 (86.5) | 580 (13.5) |
| Rural | 3607 (85.8) | 597 (14.2) |
| Occupation, n (%) | ||
| I | 593 (85.7) | 103 (14.3) |
| II | 1725 (86.3) | 281 (13.7) |
| III | 2296 (90.9) | 237 (9.1) |
| IV | 2698 (83.0) | 556 (17.0) * |
| BMI, n (%) | ||
| 18–24 kg/m2 | 4197 (86.6) | 651 (13.4) |
| 25–29 kg/m2 | 2266 (85.6) | 380 (14.4) |
| ≥30 kg/m2 | 849 (85.3) | 146 (14.7) |
| Smoke, n (%) | ||
| No | 3876 (85.5) | 655 (14.5) |
| Yes | 3436 (86.8) | 522 (13.2) |
| Celiac disease, n (%) | ||
| No | 6851 (87.1) | 1015 (12.9) |
| Yes | 461 (74.0) | 162 (26.0) ** |
| Variables | No Celiac Disease (n = 7866) | Celiac Disease (n = 623) |
|---|---|---|
| Thyroid disorders total no. (%) | ||
| No Thyroid Disorders | 6851 (93.7) | 461 (74.0) |
| Autoimmune Thyroid Disorders | 594 (7.5) | 96 (15.4) ** |
| Hashimoto’s in euthyroidism | 84 (1.1) | 17 (2.7) ** |
| Hashimoto’s with hypofunction § | 443 (5.6) | 71 (11.4) ** |
| Graves’ disease | 67 (0.8) | 8 (1.3) |
| No Autoimmune Thyroid Disorders | 421 (5.1) | 66 (10.6) ** |
| Thyroid nodules/goiter | 141 (1.8) | 6 (0.9) |
| Iatrogenic thyroid hypo/hyperfunction | 25 (0.3) | 1 (0.2) |
| Thyroidectomy # | 255 (3.2) | 59 (9.5) ** |
| Variables | Unadjusted OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|
| Sex | ||
| Male | Ref. | Ref. |
| Female | 6.031 (4.663–7.800) ** | 5.855 (4.434–7.731) ** |
| Age | 1.006 (1.001–1.010) * | 1.012 (1.007–1.017) ** |
| Area | ||
| Urban | Ref. | Ref. |
| Rural | 0.997 (0.856–1.161) | 1.100 (0.937–1.291) |
| Occupation | ||
| I | Ref. | Ref. |
| II | 0.879 (0.641–1.205) | 0.999 (0.723–1.379) |
| III | 0.583 (0.423–0.804) ** | 0.837 (0.600–1.167) |
| IV | 1.311 (0.980–1.754) | 1.028 (0.763–1.387) |
| Body mass index | 0.995 (0.976–1.014) | 1.004 (0.984–1.024) |
| Smoke | ||
| No | Ref. | Ref. |
| Yes | 0.978 (0.839–1.140) | 1.135 (0.932–1.382) |
| Celiac disease | ||
| No | Ref. | Ref. |
| Yes | 2.382 (1.901–2.983) ** | 2.387 (1.857–3.068) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dore, M.P.; Fanciulli, G.; Rouatbi, M.; Mereu, S.; Pes, G.M. Autoimmune Thyroid Disorders Are More Prevalent in Patients with Celiac Disease: A Retrospective Case-Control Study. J. Clin. Med. 2022, 11, 6027. https://doi.org/10.3390/jcm11206027
Dore MP, Fanciulli G, Rouatbi M, Mereu S, Pes GM. Autoimmune Thyroid Disorders Are More Prevalent in Patients with Celiac Disease: A Retrospective Case-Control Study. Journal of Clinical Medicine. 2022; 11(20):6027. https://doi.org/10.3390/jcm11206027
Chicago/Turabian StyleDore, Maria Pina, Giuseppe Fanciulli, Malik Rouatbi, Sandro Mereu, and Giovanni Mario Pes. 2022. "Autoimmune Thyroid Disorders Are More Prevalent in Patients with Celiac Disease: A Retrospective Case-Control Study" Journal of Clinical Medicine 11, no. 20: 6027. https://doi.org/10.3390/jcm11206027