
The Time-Based Effects of Kinesio Taping on Acute-Onset Muscle Soreness and Calf Muscle Extensibility among Endurance Athletes: A Randomized Cross-Over Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Sample Size
2.1.2. Ethical Consideration
2.1.3. Participants and Setting
2.1.4. Outcomes Measures
2.1.5. Procedure
2.1.6. Interventions
Kinesio Tape Application
Sham Tape Application
3. Data Analysis
4. Results
4.1. Pain
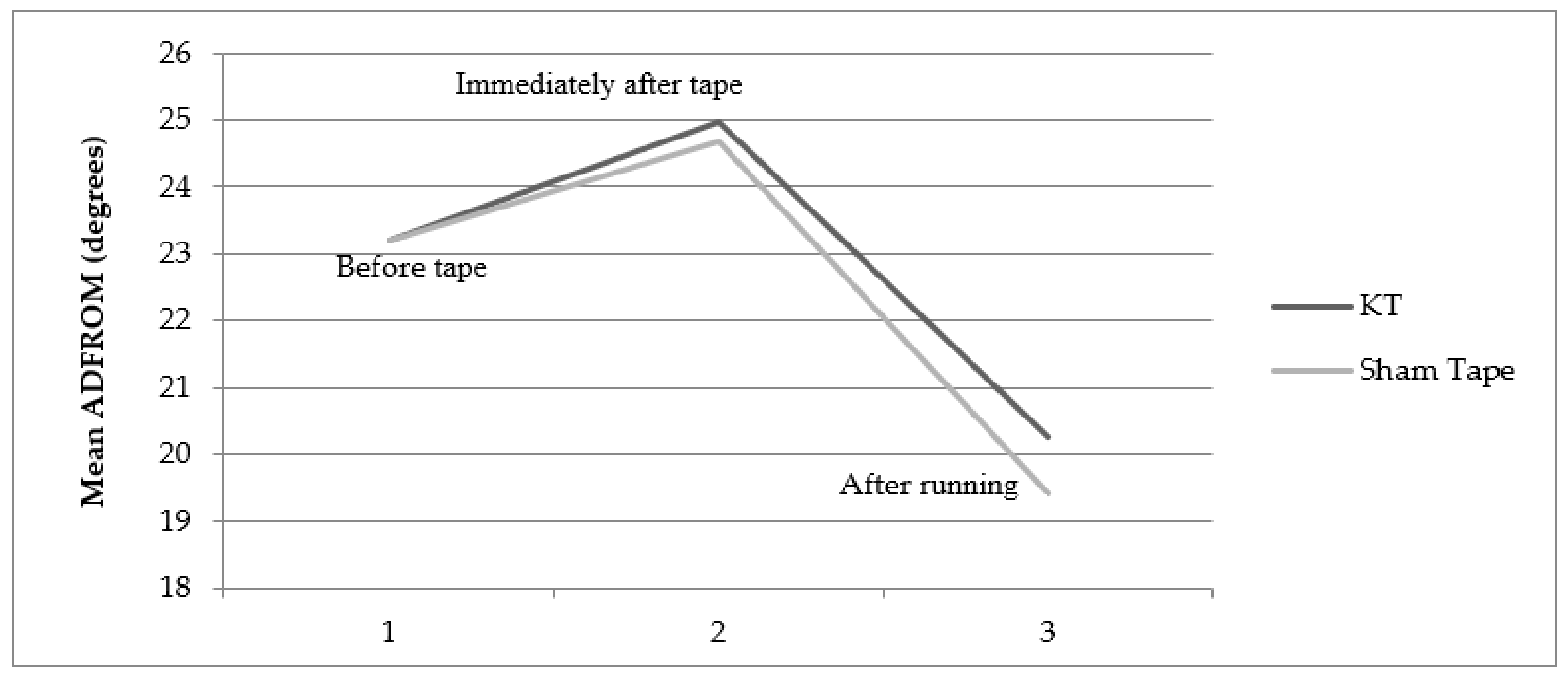
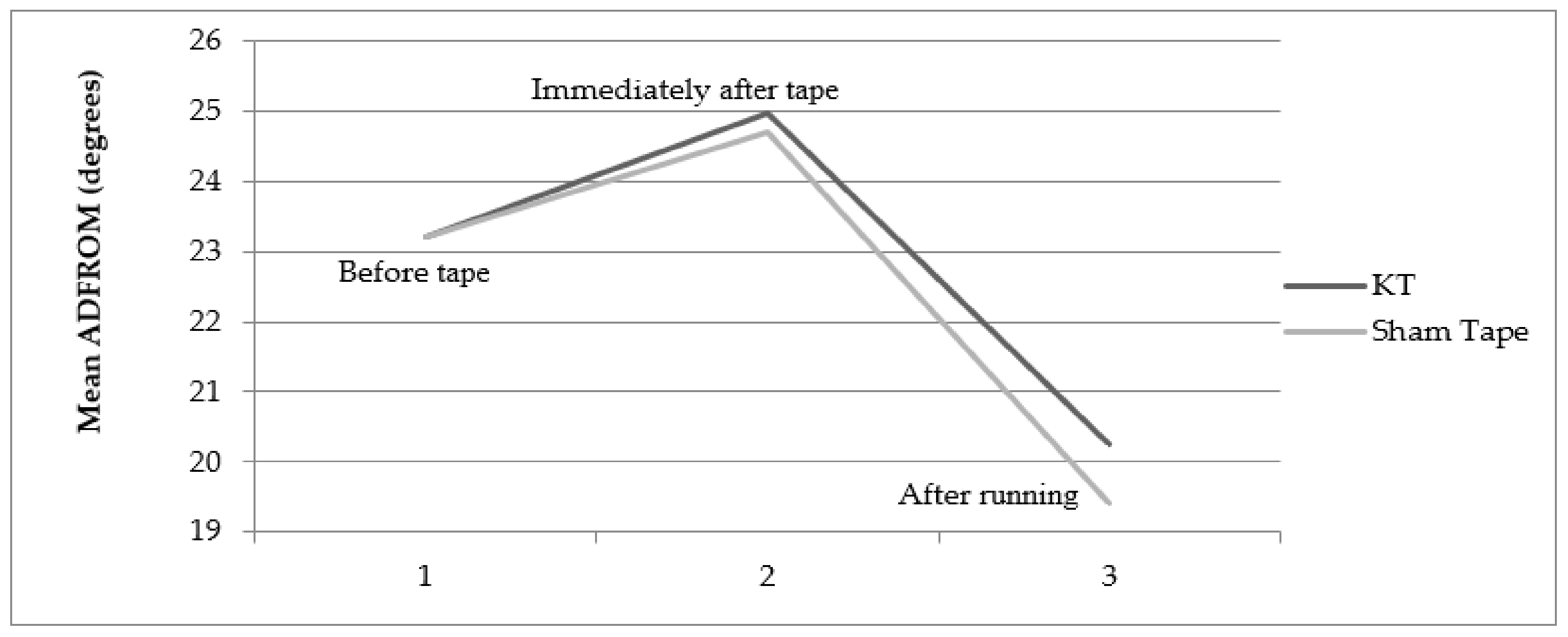
4.2. Extensibility
4.3. Time
5. Discussion
6. Limitations
7. Practical Application of the Study
8. Scope for Future Studies
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- González-Iglesias, J.; Fernández-de-las-Peñas, C.; Cleland, J.; Huijbregts, P.; Gutiérrez-Vega, M.D.R. Short-Term Effects of Cervical Kinesio Taping on Pain and Cervical Range of Motion in Patients with Acute Whiplash Injury: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2009, 39, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoloni, M.; Bernetti, A.; Fratocchi, G.; Mangone, M.; Parrinello, L.; Cooper, M.D.P.; Sesto, L. Kinesio Taping applied to lumbar muscles influences clinical and electromyographic characteristics in chronic low back pain patients. Eur. J. Phys. Rehabil. Med. 2011, 47, 9. [Google Scholar]
- Hammer, W.I. Functional Soft-Tissue Examination and Treatment by Manual Methods; Jones & Bartlett Learning: Burlington, MA, USA, 2007. [Google Scholar]
- Jaraczewska, E.; Long, C. Kinesio® Taping in Stroke: Improving Functional Use of the Upper Extremity in Hemiplegia. Top. Stroke Rehabil. 2006, 13, 31–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschalis, V.; Giakas, G.; Baltzopoulos, V.; Jamurtas, A.Z.; Theoharis, V.; Kotzamanidis, C.; Koutedakis, Y. The effects of muscle damage following eccentric exercise on gait biomechanics. Gait Posture 2007, 25, 236–242. [Google Scholar] [CrossRef]
- Kellis, E.; Liassou, C. The Effect of Selective Muscle Fatigue on Sagittal Lower Limb Kinematics and Muscle Activity during Level Running. J. Orthop. Sport. Phys. Ther. 2009, 39, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.Y.; Hsieh, T.H.; Lu, S.C.; Su, F.C. Effect of kinesiotape to muscle activity and vertical jump performance in healthy inactive people. Biomed. Eng. Online 2010, 10, 70. [Google Scholar] [CrossRef] [Green Version]
- Wallis, J.; Kase, T.; Kase, K. Clinical Therapeutic Applications of the Kinesio Taping Method; Ken Ikai Co.: Tokyo, Japan, 2003. [Google Scholar]
- Vithoulk, I.; Beneka, A.; Malliou, P.; Aggelousis, N.; Karatsolis, K.; Diamantopoulos, K. The Effects of Kinesio Taping on Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete Women. Isokinet. Exerc. Sci. 2010, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, A.; Kahanov, L. The Effect of Kinesio Taping on Lower Trunk Range of Motions. Res. Sport. Med. 2007, 15, 103–112. [Google Scholar] [CrossRef]
- Halseth, T.; McChesney, J.W.; DeBeliso, M.; Vaughn, R. The Effects of Kinesio™ Taping on Proprioception at the Ankle. J. Sport. Sci. Med. 2004, 3, 1–7. [Google Scholar]
- Adler, G.; Kruszyniewicz, J.; Skonieczna-Żydecka, K.; Sroka, R. The Analgesic Efficacy of Kinesiology Taping in Delayed Onset Muscle Soreness (DOMS). Cent. Eur. J. Sport Sci. Med. 2016, 13, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Szymura, J.; Maciejczyk, M.; Wiecek, M.; Maciejczyk, G.; Wiecha, S.; Ochalek, K.; Kepinska, M.; Szygula, Z. Effects of kinesio taping on anaerobic power recovery after eccentric exercise. Res. Sport. Med. 2016, 24, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Zhou, S.; Crowley-McHattan, Z.J.; Bezerra, P.; Tseng, W.C.; Chen, C.H.; Ye, X. Acute effects of kinesiology taping stretch tensions on soleus and gastrocnemius H-Reflex modulations. Int. J. Environ. Res. Public Health 2021, 18, 4411. [Google Scholar] [CrossRef]
- Chen, Y.S.; Tseng, W.C.; Chen, C.H.; Bezerra, P.; Ye, X. Acute effects of kinesiology tape tension on soleus muscle h-reflex modulations during lying and standing postures. PLoS ONE 2020, 15, e0236587. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.; Brukner, P. Clinical Sports Medicine, 3rd ed.; Tata McGraw Hill: New York, NY, USA, 2008; 970p. [Google Scholar]
- Reneker, J.C.; Latham, L.; McGlawn, R.; Reneker, M.R. Effectiveness of kinesiology tape on sports performance abilities in athletes: A systematic review. Phys. Ther. Sport 2018, 31, 83–98. [Google Scholar] [CrossRef]
- Chang, H.Y.; Cheng, S.C.; Lin, C.C.; Chou, K.Y.; Gan, S.M.; Wang, C.H. The effectiveness of kinesio taping for athletes with medial elbow epicondylar tendinopathy. Int. J. Sport. Med. 2013, 34, 1003–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biz, C.; Nicoletti, P.; Tomasin, M.; Bragazzi, N.L.; Di Rubbo, G.; Ruggieri, P. Is Kinesio Taping Effective for Sport Performance and Ankle Function of Athletes with Chronic Ankle Instability (CAI)? A Systematic Review and Meta-Analysis. Medicina 2022, 58, 620. [Google Scholar] [CrossRef]
- Artioli, D.P.; Bertolini, G.R. Kinesio taping: Application and results on pain: Systematic review. Fisioter. Pesqui. 2014, 21, 94–99. [Google Scholar] [CrossRef]
- Merino-Marban, R.; Fernandez-Rodriguez, E.; Lopez-Fernandez, I.; Mayorga-Vega, D. The acute effect of Kinesio taping on hamstring extensibility in university students. J. Phys. Educ. Sport 2011, 11, 23–27. [Google Scholar]
- Salvat Salvat, I.; Alonso Salvat, A. Efectos inmediatos del kinesio taping en la flexión lumbar. Fisioterapia 2010, 32, 57–65. [Google Scholar] [CrossRef]
- Merino-Marban, R.; Fernandez-Rodriguez, E.; Mayorga-Vega, D. The Effect of Kinesio Taping on Calf Pain and Extensibility Immediately After Its Application and After a Duathlon Competition. Res. Sport. Med. 2014, 22, 1–11. [Google Scholar] [CrossRef]
- Shoger, M.; Nishi, Y.; Merrick, M.A.; Ingersoll, C.D.; Edwards, J.E. Kinesiotape does not reduce the pain or swelling associated with delayed onset muscle soreness. J. Athl. Train. 2000, 35, 44. [Google Scholar]
- Espejo-Antúnez, L.; López-Miñarro, P.A.; Garrido-Ardila, E.M.; Castillo-Lozano, R.; Domínguez-Vera, P.; Maya-Martín, J.; Albornoz-Cabello, M. A comparison of acute effects between Kinesio tape and electrical muscle elongation in hamstring extensibility. J. Back Musculoskelet. Rehabil. 2015, 28, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, L.A. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription, 5th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2006. [Google Scholar]
- Roitman, J.L.; LaFontaine, T. Modified protocols for cardiovascular rehabilitation and program efficacy. J. Cardiopulm. Rehabil. 2001, 21, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Ding, F. Progress in application of Kinesio Taping in Knee Osteoarthritis. Chin. J. Conval. Med. 2022, 31, 687. [Google Scholar]
- Hazar, Z.; Çitaker, S.; Demirtaş, C.Y.; Bukan, N.Ç.; Kafa, N.; Çelik, B. Effects of kinesiology taping on delayed onset muscle soreness: A randomized controlled pilot study. J. Exerc. Ther. Rehabil. 2014, 1, 49–54. [Google Scholar]
- Kaya, E.; Zinnuroglu, M.; Tugcu, I. Kinesio taping compared to physical therapy modalities for the treatment of shoulder impingement syndrome. Clin. Rheumatol. 2011, 30, 201–207. [Google Scholar] [CrossRef]
- García-Muro, F.; Rodríguez-Fernández, Á.L.; Herrero-de-Lucas, Á. Treatment of myofascial pain in the shoulder with Kinesio Taping. A case reports. Man. Ther. 2010, 15, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Thelen, M.D.; Dauber, J.A.; Stoneman, P.D. The Clinical Efficacy of Kinesio Tape for Shoulder Pain: A Randomized, Double-Blinded, Clinical Trial. J. Orthop. Sports Phys. Ther. 2008, 38, 389–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakeri, H.; Keshavarz, R.; Arab, A.M.; Ebrahimi, I. Clinical effectiveness of kinesiological taping on pain and pain free shoulder range of motion in patients with shoulder impingement syndrome: A randomized, double blinded, placebo-controlled trial. Int. J. Sport. Phys. Ther. 2013, 8, 800–810. [Google Scholar]
- Kneeshaw, D. Shoulder taping in the clinical setting. J. Bodyw. Mov. Ther. 2002, 6, 2–8. [Google Scholar] [CrossRef]
- Banerjee, G.; Briggs, M.; Johnson, M.I. Kinesiology taping as an adjunct for pain management: A review of literature and evidence. Indian J. Pain 2016, 30, 151. [Google Scholar] [CrossRef]
- Findley, T.; Chaudhry, H.; Stecco, A.; Roman, M. Fascia research—A narrative review. J. Bodyw. Mov. Ther. 2012, 16, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Álvarez, S.; San José, F.; Rodríguez-Fernández, A.L.; Güeita-Rodríguez, J.; Waller, B.J. Effects of Kinesio® Tape in low back muscle fatigue: Randomized, controlled, doubled-blinded clinical trial on healthy subjects. J. Back Musculoskelet. Rehabil. 2014, 27, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagen, L.; Hebert, J.J.; Dekanich, J.; Koppenhaver, S. The Effect of Elastic Therapeutic Taping on Back Extensor Muscle Endurance in Patients with Low Back Pain: A Randomized, Controlled, Crossover Trial. J. Orthop. Sports Phys. Ther. 2015, 45, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Osorio, J.A.; Vairo, G.L.; Rozea, G.D.; Bosha, P.J.; Millard, R.L.; Aukerman, D.F.; Sebastianelli, W.J. The effects of two therapeutic patellofemoral taping techniques on strength, endurance, and pain responses. Phys. Ther. Sport 2013, 14, 199–206. [Google Scholar] [CrossRef]
- Cowan, S.M.; Bennell, K.L.; Hodges, P.W. Therapeutic Patellar Taping Changes the Timing of Vasti Muscle Activation in People with Patellofemoral Pain Syndrome. Clin. J. Sport Med. 2002, 12, 339–347. [Google Scholar] [CrossRef]
- Kumbrink, B. K-Taping: An Illustrated Guide—Basics—Techniques—Indications; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Hausswirth, C.; Louis, J.; Bieuzen, F.; Pournot, H.; Fournier, J.; Filliard, J.-R.; Brisswalter, J. Effects of Whole-Body Cryotherapy vs. Far-Infrared vs. Passive Modalities on Recovery from Exercise-Induced Muscle Damage in Highly-Trained Runners. PLoS ONE 2011, 6, e27749. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Yoo, W. Treatment of chronic Achilles tendon pain by Kinesio taping in an amateur badminton player. Phys. Ther. Sport 2012, 13, 115–119. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD | Minimum | Maximum | |
|---|---|---|---|---|
| Age (years) | 16.36 ± 2.69 | 10 | 20 | |
| Gender | Male | 31 | n/a | n/a |
| Female | 24 | n/a | n/a | |
| BMI | 19.44 ± 1.14 | 16.40 | 21.39 | |
| ETE (years) | 1.95 ± 0.91 | 1 | 5 | |
| FT (min.) | KT | 11.74 ± 7.01 | 4.20 | 30 |
| ST | 11.14 ± 6.11 | 4.34 | 30 | |
| ADFROM (°) | KT (Lt/Rt) | 23.20° ± 4.057°/23.20° ± 3.75° | 15°/18° | 42°/40° |
| ST(Lt/Rt) | 23.20° ± 4.057°/23.22° ± 3.75° | 15°/18° | 42°/40° | |
| Variables | With Kinesio Tape | With Sham Tape | Paired t-Test | |||
|---|---|---|---|---|---|---|
| Mean (cm) | SD | Mean (cm) | SD | t value | p-Value | |
| NPRS0 | 3.28 | 1.257 | 3.89 | 1.165 | 2.388 * | 0.020 * |
| NPRS10 | 1.04 | 1.071 | 1.24 | 0.922 | 1.466 | 0.154 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malhotra, D.; Sharma, S.; Chachra, A.; Dhingra, M.; Alghadir, A.H.; Nuhmani, S.; Jaleel, G.; Alqhtani, R.S.; Alshehri, M.M.; Beg, R.A.; et al. The Time-Based Effects of Kinesio Taping on Acute-Onset Muscle Soreness and Calf Muscle Extensibility among Endurance Athletes: A Randomized Cross-Over Trial. J. Clin. Med. 2022, 11, 5996. https://doi.org/10.3390/jcm11205996
Malhotra D, Sharma S, Chachra A, Dhingra M, Alghadir AH, Nuhmani S, Jaleel G, Alqhtani RS, Alshehri MM, Beg RA, et al. The Time-Based Effects of Kinesio Taping on Acute-Onset Muscle Soreness and Calf Muscle Extensibility among Endurance Athletes: A Randomized Cross-Over Trial. Journal of Clinical Medicine. 2022; 11(20):5996. https://doi.org/10.3390/jcm11205996
Chicago/Turabian StyleMalhotra, Deepak, Shruti Sharma, Ashima Chachra, Meenu Dhingra, Ahmad H. Alghadir, Shibili Nuhmani, Ghufran Jaleel, Raee S. Alqhtani, Mohammed M. Alshehri, Rashid Ali Beg, and et al. 2022. "The Time-Based Effects of Kinesio Taping on Acute-Onset Muscle Soreness and Calf Muscle Extensibility among Endurance Athletes: A Randomized Cross-Over Trial" Journal of Clinical Medicine 11, no. 20: 5996. https://doi.org/10.3390/jcm11205996