
Improvement of Gait in Patients with Stroke Using Rhythmic Sensory Stimulation: A Case-Control Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Procedures
2.3. Extraction of Gait Parameters and Providing Rhythmic Sensory Stimulation
2.4. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dirnagl, U.; Iadecola, C.; Moskowitz, M.A. Pathobiology of ischaemic stroke: An integrated view. Trends Neurosci. 1999, 22, 391–397. [Google Scholar] [CrossRef]
- Lo, E.H.; Dalkara, T.; Moskowitz, M.A. Mechanisms, challenges and opportunities in stroke. Nat. Rev. Neurosci. 2003, 4, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Mackay, J.; Mensah, G.A. The Atlas of Heart Disease and Stroke; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Warlow, C.P.; Van Gijn, J.; Dennis, M.S.; Wardlaw, J.M.; Bamford, J.M.; Hankey, G.J.; Sandercock, P.A.; Rinkel, G.; Langhorne, P.; Sudlow, C. Stroke: Practical Management; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Maida, C.D.; Norrito, R.L.; Daidone, M.; Tuttolomondo, A.; Pinto, A. Neuroinflammatory mechanisms in ischemic stroke: Focus on cardioembolic stroke, background, and therapeutic approaches. Int. J. Mol. Sci. 2020, 21, 6454. [Google Scholar] [CrossRef]
- Handley, A.; Medcalf, P.; Hellier, K.; Dutta, D. Movement disorders after stroke. Age Ageing 2009, 38, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Thaut, M.H.; McIntosh, G.C.; Rice, R.R. Rhythmic facilitation of gait training in hemiparetic stroke rehabilitation. J. Neurol. Sci. 1997, 151, 207–212. [Google Scholar] [CrossRef]
- Gupta, N.; Pandey, S. Post-thalamic stroke movement disorders: A systematic review. Eur. Neurol. 2018, 79, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture 2010, 31, 241–246. [Google Scholar] [CrossRef]
- Wright, R.L.; Bevins, J.W.; Pratt, D.; Sackley, C.M.; Wing, A.M. Metronome cueing of walking reduces gait variability after a cerebellar stroke. Front. Neurol. 2016, 7, 84. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, M.; Hosseini, H.A. Investigating the relationship between spatiotemporal gait variability and falls self-efficacy in individuals with chronic stroke. Physiother. Theory Pract. 2020, 38, 1–9. [Google Scholar] [CrossRef]
- Balasubramanian, C.K.; Neptune, R.R.; Kautz, S.A. Variability in spatiotemporal step characteristics and its relationship to walking performance post-stroke. Gait Posture 2009, 29, 408–414. [Google Scholar] [CrossRef] [Green Version]
- Kao, P.-C.; Dingwell, J.B.; Higginson, J.S.; Binder-Macleod, S. Dynamic instability during post-stroke hemiparetic walking. Gait Posture 2014, 40, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Baetens, T.; De Kegel, A.; Palmans, T.; Oostra, K.; Vanderstraeten, G.; Cambier, D. Gait analysis with cognitive-motor dual tasks to distinguish fallers from nonfallers among rehabilitating stroke patients. Arch. Phys. Med. Rehabil. 2013, 94, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Soyuer, F.; Öztürk, A. The effect of spasticity, sense and walking aids in falls of people after chronic stroke. Disabil. Rehabil. 2007, 29, 679–687. [Google Scholar] [CrossRef]
- Toebes, M.J.; Hoozemans, M.J.; Furrer, R.; Dekker, J.; van Dieën, J.H. Local dynamic stability and variability of gait are associated with fall history in elderly subjects. Gait Posture 2012, 36, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Batchelor, F.A.; Mackintosh, S.F.; Said, C.M.; Hill, K.D. Falls after stroke. Int. J. Stroke 2012, 7, 482–490. [Google Scholar] [CrossRef]
- Hsu, A.-L.; Tang, P.-F.; Jan, M.-H. Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1185–1193. [Google Scholar] [CrossRef]
- Mizuike, C.; Ohgi, S.; Morita, S. Analysis of stroke patient walking dynamics using a tri-axial accelerometer. Gait Posture 2009, 30, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Titianova, E.B.; Tarkka, I.M. Asymmetry in walking performance and postural sway in patients with chronic unilateral cerebral infarction. J. Rehabil. Res. Dev. 1995, 32, 236–244. [Google Scholar] [PubMed]
- Muci, B.; Keser, I.; Meric, A.; Karatas, G.K. What are the factors affecting dual-task gait performance in people after stroke? Physiother. Theory Pract. 2020, 38, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Von Schroeder, H.P.; Coutts, R.D.; Lyden, P.D.; Billings, E.; Nickel, V.L. Gait parameters following stroke: A practical assessment. J. Rehabil. Res. Dev. 1995, 32, 25. [Google Scholar] [PubMed]
- Guzik, A.; Drużbicki, M. Application of the Gait Deviation Index in the analysis of post-stroke hemiparetic gait. J. Biomech. 2020, 99, 109575. [Google Scholar] [CrossRef]
- Wall, J.; Ashburn, A. Assessment of gait disability in hemiplegics. Hemiplegic gait. Scand. J. Rehabil. Med. 1979, 11, 95–103. [Google Scholar]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait characteristics of post-stroke hemiparetic patients with different walking speeds. Int. J. Rehabil. Research. Int. Z. Rehabilitationsforschung. Rev. Int. Rech. Readapt. 2020, 43, 69. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics, fractals and falls: Finding meaning in the stride-to-stride fluctuations of human walking. Hum. Mov. Sci. 2007, 26, 555–589. [Google Scholar] [CrossRef] [Green Version]
- Lord, S.; Howe, T.; Greenland, J.; Simpson, L.; Rochester, L. Gait variability in older adults: A structured review of testing protocol and clinimetric properties. Gait Posture 2011, 34, 443–450. [Google Scholar] [CrossRef]
- Nieuwboer, A.; Kwakkel, G.; Rochester, L.; Jones, D.; van Wegen, E.; Willems, A.M.; Chavret, F.; Hetherington, V.; Baker, K.; Lim, I. Cueing training in the home improves gait-related mobility in Parkinson’s disease: The RESCUE trial. J. Neurol. Neurosurg. Psychiatry 2007, 78, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Clements-Cortes, A.; Bartel, L.; Ahonen, H.; Freedman, M. The potential of rhythmic sensory stimulation treatments for persons with Alzheimer’s disease. Music Med. 2017, 9, 167–173. [Google Scholar] [CrossRef]
- Galica, A.M.; Kang, H.G.; Priplata, A.A.; D’Andrea, S.E.; Starobinets, O.V.; Sorond, F.A.; Cupples, L.A.; Lipsitz, L.A. Subsensory vibrations to the feet reduce gait variability in elderly fallers. Gait Posture 2009, 30, 383–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arias, P.; Cudeiro, J. Effects of rhythmic sensory stimulation (auditory, visual) on gait in Parkinson’s disease patients. Exp. Brain Res. 2008, 186, 589–601. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.H.; Han, S.J.; Jeon, S.Y.; Kim, H.J.; Lee, J.E.; Yoon, T.S.; Chong, H.J. Effect of rhythmic auditory stimulation on gait and balance in hemiplegic stroke patients. NeuroRehabilitation 2014, 34, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Song, G.-b.; Ryu, H.J. Effects of gait training with rhythmic auditory stimulation on gait ability in stroke patients. J. Phys. Ther. Sci. 2016, 28, 1403–1406. [Google Scholar] [CrossRef] [Green Version]
- Kobinata, N.; Ueno, M.; Imanishi, Y.; Yoshikawa, H. Immediate effects of rhythmic auditory stimulation on gait in stroke patients in relation to the lesion site. J. Phys. Ther. Sci. 2016, 28, 2441–2444. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H.; Abiru, M. Rhythmic auditory stimulation in rehabilitation of movement disorders: A review of current research. Music. Percept. 2010, 27, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Cha, Y.; Kim, Y.; Hwang, S.; Chung, Y. Intensive gait training with rhythmic auditory stimulation in individuals with chronic hemiparetic stroke: A pilot randomized controlled study. NeuroRehabilitation 2014, 35, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Mainka, S.; Wissel, J.; Völler, H.; Evers, S. The use of rhythmic auditory stimulation to optimize treadmill training for stroke patients: A randomized controlled trial. Front. Neurol. 2018, 9, 755. [Google Scholar] [CrossRef]
- Sejdić, E.; Fu, Y.; Pak, A.; Fairley, J.A.; Chau, T. The effects of rhythmic sensory cues on the temporal dynamics of human gait. PLoS ONE 2012, 7, e43104. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.; Leins, A.; Rice, R.; Argstatter, H.; Kenyon, G.; McIntosh, G.; Bolay, H.; Fetter, M. Rhythmic auditor y stimulation improves gait more than NDT/Bobath training in near-ambulatory patients early poststroke: A single-blind, randomized trial. Neurorehabil. Neural Repair 2007, 21, 455–459. [Google Scholar] [CrossRef]
- Hayden, R.; Clair, A.A.; Johnson, G.; Otto, D. The effect of rhythmic auditory stimulation (RAS) on physical therapy outcomes for patients in gait training following stroke: A feasibility study. Int. J. Neurosci. 2009, 119, 2183–2195. [Google Scholar] [CrossRef] [PubMed]
- Van Wegen, E.; de Goede, C.; Lim, I.; Rietberg, M.; Nieuwboer, A.; Willems, A.; Jones, D.; Rochester, L.; Hetherington, V.; Berendse, H. The effect of rhythmic somatosensory cueing on gait in patients with Parkinson’s disease. J. Neurol. Sci. 2006, 248, 210–214. [Google Scholar] [CrossRef]
- Pearson, K.G. Generating the walking gait: Role of sensory feedback. Prog. Brain Res. 2004, 143, 123–129. [Google Scholar]
- Nascimento, L.R.; de Oliveira, C.Q.; Ada, L.; Michaelsen, S.M.; Teixeira-Salmela, L.F. Walking training with cueing of cadence improves walking speed and stride length after stroke more than walking training alone: A systematic review. J. Physiother. 2015, 61, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prassas, S.; Thaut, M.; McIntosh, G.; Rice, R. Effect of auditory rhythmic cuing on gait kinematic parameters of stroke patients. Gait Posture 1997, 6, 218–223. [Google Scholar] [CrossRef]
- Park, J.; Park, S.-y.; Kim, Y.-w.; Woo, Y. Comparison between treadmill training with rhythmic auditory stimulation and ground walking with rhythmic auditory stimulation on gait ability in chronic stroke patients: A pilot study. NeuroRehabilitation 2015, 37, 193–202. [Google Scholar] [CrossRef]
- Cha, Y.; Kim, Y.; Chung, Y. Immediate effects of rhythmic auditory stimulation with tempo changes on gait in stroke patients. J. Phys. Ther. Sci. 2014, 26, 479–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, B.-W.; Lee, H.-Y.; Song, W.-K. Rhythmic auditory stimulation using a portable smart device: Short-term effects on gait in chronic hemiplegic stroke patients. J. Phys. Ther. Sci. 2016, 28, 1538–1543. [Google Scholar] [CrossRef] [Green Version]
- Elsner, B.; Schöler, A.; Kon, T.; Mehrholz, J. Walking with rhythmic auditory stimulation in chronic patients after stroke: A pilot randomized controlled trial. Physiother. Res. Int. 2020, 25, e1800. [Google Scholar] [CrossRef]
- Gonzalez-Hoelling, S.; Bertran-Noguer, C.; Reig-Garcia, G.; Suñer-Soler, R. Effects of a Music-Based Rhythmic Auditory Stimulation on Gait and Balance in Subacute Stroke. Int. J. Environ. Res. Public Health 2021, 18, 2032. [Google Scholar] [CrossRef]
- Lee, S.; Lee, K.; Song, C. Gait training with bilateral rhythmic auditory stimulation in stroke patients: A randomized controlled trial. Brain Sci. 2018, 8, 164. [Google Scholar] [CrossRef] [Green Version]
- Suteerawattananon, M.; Morris, G.; Etnyre, B.; Jankovic, J.; Protas, E. Effects of visual and auditory cues on gait in individuals with Parkinson’s disease. J. Neurol. Sci. 2004, 219, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Collen, F.M.; Wade, D.T.; Robb, G.; Bradshaw, C. The Rivermead mobility index: A further development of the Rivermead motor assessment. Int. Disabil. Stud. 1991, 13, 50–54. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Dadashi, F.; Mariani, B.; Rochat, S.; Büla, C.J.; Santos-Eggimann, B.; Aminian, K. Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sensors 2014, 14, 443–457. [Google Scholar] [CrossRef] [Green Version]
- Grzesiak, A.; Aminian, K.; Lécureux, E.; Jobin, F.; Jolles, B.M. Total hip replacement with a collarless polished cemented anatomic stem: Clinical and gait analysis results at ten years follow-up. Int. Orthop. 2014, 38, 717–724. [Google Scholar] [CrossRef] [Green Version]
- Malatesta, D.; Canepa, M.; Fernandez, A.M. The effect of treadmill and overground walking on preferred walking speed and gait kinematics in healthy, physically active older adults. Eur. J. Appl. Physiol. 2017, 117, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef]
- Wüest, S.; Masse, F.; Aminian, K.; Gonzenbach, R.; De Bruin, E.D. Reliability and validity of the inertial sensor-based Timed “Up and Go” test in individuals affected by stroke. J. Rehabil. Res. Dev. 2016, 53, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Cudkowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Islam, R.; Holland, S.; Price, B.; Georgiou, T.; Mulholland, P. Wearables for Long Term Gait Rehabilitation of Neurological Conditions. In Proceedings of the Short Workshop on Next Steps towards Long Term Self Tracking, CHI 2018: CHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 21–26 April 2018. [Google Scholar]
- Hausdorff, J.M.; Schweiger, A.; Herman, T.; Yogev-Seligmann, G.; Giladi, N. Dual-task decrements in gait: Contributing factors among healthy older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Pan, W.-Y.; Li, F.; Ge, J.-S.; Zhang, X.; Luo, X.; Wang, Y.-L. Effect of Rhythm of Music Therapy on Gait in Patients with Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105544. [Google Scholar] [CrossRef] [PubMed]
- Kandel, E.R.; Schwartz, J.H.; Jessell, T.M.; Siegelbaum, S.; Hudspeth, A.J.; Mack, S. Principles of Neural Science; McGraw-Hill: New York, NY, USA, 2000; Volume 4. [Google Scholar]
- Thaut, M.; Kenyon, G.; Schauer, M.; McIntosh, G. The connection between rhythmicity and brain function. IEEE Eng. Med. Biol. Mag. 1999, 18, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Judge, J.O.; King, M.B.; Whipple, R.; Clive, J.; Wolf son, L.I. Dynamic balance in older persons: Effects of reduced visual and proprioceptive input. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50, M263–M270. [Google Scholar] [CrossRef]
- Wuehr, M.; Schniepp, R.; Schlick, C.; Huth, S.; Pradhan, C.; Dieterich, M.; Brandt, T.; Jahn, K. Sensory loss and walking speed related factors for gait alterations in patients with peripheral neuropathy. Gait Posture 2014, 39, 852–858. [Google Scholar] [CrossRef]
- Vaney, C.; Blaurock, H.; Gattlen, B.; Meisels, C. Assessing mobility in multiple sclerosis using the Rivermead Mobility Index and gait speed. Clin. Rehabil. 1996, 10, 216–226. [Google Scholar] [CrossRef]
- Lim, J.Y.; An, S.H.; Park, D.-S. Walking velocity and modified rivermead mobility index as discriminatory measures for functional ambulation classification of chronic stroke patients. Hong Kong Physiother. J. 2019, 39, 125–132. [Google Scholar] [CrossRef]
- Maki, B.E. Gait changes in older adults: Predictors of falls or indicators of fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning. J. Neuroeng. Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef] [Green Version]
- Bonan, I.; Marquer, A.; Eskiizmirliler, S.; Yelnik, A.; Vidal, P.-P. Sensory reweighting in controls and stroke patients. Clin. Neurophysiol. 2013, 124, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Cirstea, C.; Ptito, A.; Levin, M. Feedback and cognition in arm motor skill reacquisition after stroke. Stroke 2006, 37, 1237–1242. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stroke (n = 20) | Control (n = 20) | p-Value | |
|---|---|---|---|
| Age (years) | 72.10 ± 7.15 | 72.65 ± 6.93 | NS |
| Height (cm) | 162.30 ± 8.65 | 163.60 ± 8.09 | NS |
| Weight (kg) | 63.55 ± 8.65 | 65.51 ± 10.04 | NS |
| Gender (female/male) | 8/12 | 8/12 | NS |
| BMI (kg/m2) | 23.97 ± 2.52 | 24.44 ± 2.89 | NS |
| WHR (waist/hip ratio) | 0.87 ± 0.05 | 0.89 ± 0.05 | NS |
| Education (years) | 16.50 ± 7.03 | 16.55 ± 5.24 | NS |
| MMSE † (Max score: 30) | 24.15 ± 4.90 | 28.45 ± 1.53 | <0.001 * |
| RMI ‡ (Max score: 15) | 11.85 ± 2.10 | 15.00 ± 0.00 | <0.001 * |
| Timed Up and Go test (s) | 17.32 ± 7.19 | 7.76 ± 1.13 | <0.001 * |
| No. of falls in previous year (No (%)) | 0.55 ± 0.99 (35%) | 0.05 ± 0.22 (5%) | 0.040 * |
| Period after stroke onset (months) | 114.95 ± 78.23 | ||
| Hemiparetic side (right/left) | 6/14 | ||
| Type of stroke (I/H) § | 16/4 | ||
| Use of walking aid (yes/no) | 7/13 |
| Walking Condition | |||||||
|---|---|---|---|---|---|---|---|
| Gait Variable | Group | Normal † | RAS ‡ | RSS § | RCS ¶ | p-Value | |
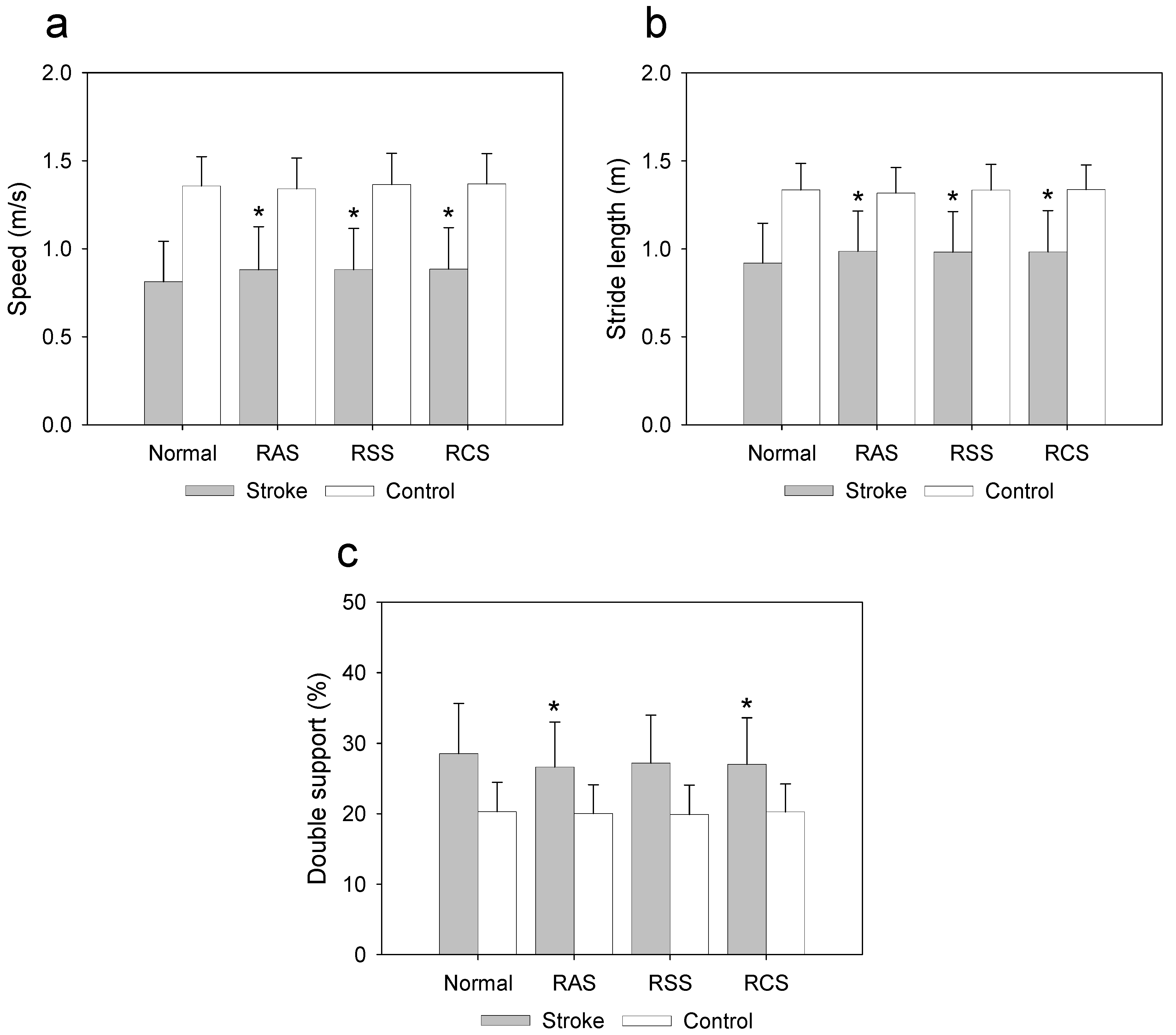
| Speed (m/s) | Stroke (n = 20) | 0.81 ± 0.23 | 0.88 ± 0.24 | 0.88 ± 0.23 | 0.88 ± 0.23 | Group < 0.001 * | 0.607 |
| Control (n = 20) | 1.35 ± 0.16 | 1.34 ± 0.17 | 1.36 ± 0.17 | 1.36 ± 0.17 | Condition < 0.001 * | 0.158 | |
| Interaction 0.002 * | 0.143 | ||||||
| Stride length (m) | Stroke (n = 20) | 0.91 ± 0.22 | 0.98 ± 0.22 | 0.98 ± 0.23 | 0.98 ± 0.23 | Group < 0.001 * | 0.490 |
| Control (n = 20) | 1.33 ± 0.14 | 1.31 ± 0.14 | 1.33 ± 0.14 | 1.33 ± 0.14 | Condition < 0.001 * | 0.163 | |
| Interaction < 0.001 * | 0.232 | ||||||
| Gait cycle (s) | Stroke (n = 20) | 1.18 ± 0.20 | 1.16 ± 0.20 | 1.16 ± 0.20 | 1.15 ± 0.19 | Group < 0.001 * | 0.260 |
| Control (n = 20) | 0.99 ± 0.06 | 0.99 ± 0.07 | 0.99 ± 0.07 | 0.98 ± 0.07 | Condition 0.023 * | 0.096 | |
| Interaction 0.257 | 0.035 | ||||||
| Cadence (steps/min) | Stroke (n = 20) | 104.10 ± 15.60 | 105.59 ± 15.37 | 105.95 ± 15.28 | 106.32 ± 14.95 | Group < 0.001 * | 0.305 |
| Control (n = 20) | 121.03 ± 8.17 | 121.33 ± 9.37 | 121.99 ± 9.68 | 122.22 ± 9.86 | Condition 0.014 * | 0.104 | |
| Interaction 0.581 | 0.015 | ||||||
| Stance (%) | Stroke (n = 20) | 63.19 ± 4.06 | 62.61 ± 3.52 | 62.58 ± 4.08 | 62.49 ± 3.80 | Group 0.010 * | 0.163 |
| Control (n = 20) | 60.11 ± 2.39 | 60.03 ± 2.16 | 59.89 ± 2.53 | 60.06 ± 2.35 | Condition 0.126 | 0.052 | |
| Interaction 0.326 | 0.029 | ||||||
| Swing (%) | Stroke (n = 20) | 36.80 ± 4.06 | 37.38 ± 3.52 | 37.41 ± 4.08 | 37.50 ± 3.80 | Group 0.010 * | 0.163 |
| Control (n = 20) | 39.88 ± 2.39 | 39.96 ± 2.16 | 40.10 ± 2.53 | 39.93 ± 2.35 | Condition 0.126 | 0.052 | |
| Interaction 0.326 | 0.029 | ||||||
| Double support (%) | Stroke (n = 20) | 28.54 ± 7.07 | 26.65 ± 6.36 | 27.20 ± 6.81 | 27.01 ± 6.61 | Group < 0.001 * | 0.314 |
| Control (n = 20) | 20.28 ± 4.18 | 20.03 ± 4.10 | 19.89 ± 4.19 | 20.27 ± 3.95 | Condition < 0.001 * | 0.157 | |
| Interaction 0.006 * | 0.106 | ||||||
| Stride length CV (%) | Stroke (n = 20) | 6.87 ± 2.92 | 5.13 ± 1.59 | 5.24 ± 1.75 | 5.14 ± 1.78 | Group < 0.001 * | 0.488 |
| Control (n = 20) | 2.60 ± 0.71 | 3.20 ± 0.95 | 3.10 ± 0.96 | 2.91 ± 0.59 | Condition 0.008 * | 0.119 | |
| Interaction < 0.001 * | 0.286 | ||||||
| Gait cycle CV (%) | Stroke (n = 20) | 4.69 ± 2.28 | 3.37 ± 1.25 | 3.54 ± 1.39 | 3.54 ± 1.41 | Group < 0.001 * | 0.357 |
| Control (n = 20) | 2.05 ± 0.87 | 2.23 ± 0.71 | 2.15 ± 0.63 | 2.14 ± 0.67 | Condition < 0.001 * | 0.151 | |
| Interaction < 0.001 * | 0.218 | ||||||
| Stance CV (%) | Stroke (n = 20) | 4.04 ± 1.42 | 3.16 ± 0.82 | 3.15 ± 1.05 | 3.12 ± 0.88 | Group 0.003 * | 0.213 |
| Control (n = 20) | 2.36 ± 1.09 | 2.50 ± 1.09 | 2.26 ± 1.24 | 2.37 ± 1.13 | Condition < 0.001 * | 0.129 | |
| Interaction < 0.001 * | 0.138 | ||||||
| Swing CV (%) | Stroke (n = 20) | 7.29 ± 3.73 | 5.40 ± 1.91 | 5.50 ± 2.63 | 5.39 ± 2.15 | Group < 0.001 * | 0.247 |
| Control (n = 20) | 3.56 ± 1.64 | 3.78 ± 1.64 | 3.41 ± 1.88 | 3.59 ± 1.71 | Condition < 0.001 * | 0.162 | |
| Interaction < 0.001 * | 0.177 | ||||||
| Double support CV (%) | Stroke (n = 20) | 11.16 ± 3.05 | 9.54 ± 2.43 | 9.65 ± 2.91 | 9.22 ± 2.85 | Group 0.575 | 0.008 |
| Control (n = 20) | 10.05 ± 5.03 | 11.24 ± 5.89 | 10.10 ± 4.92 | 10.92 ± 4.53 | Condition 0.280 | 0.033 | |
| Interaction 0.002 * | 0.124 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Shin, S. Improvement of Gait in Patients with Stroke Using Rhythmic Sensory Stimulation: A Case-Control Study. J. Clin. Med. 2022, 11, 425. https://doi.org/10.3390/jcm11020425
Lee Y, Shin S. Improvement of Gait in Patients with Stroke Using Rhythmic Sensory Stimulation: A Case-Control Study. Journal of Clinical Medicine. 2022; 11(2):425. https://doi.org/10.3390/jcm11020425
Chicago/Turabian StyleLee, Yungon, and Sunghoon Shin. 2022. "Improvement of Gait in Patients with Stroke Using Rhythmic Sensory Stimulation: A Case-Control Study" Journal of Clinical Medicine 11, no. 2: 425. https://doi.org/10.3390/jcm11020425