
A Systematic Review of Nutritional Lab Correlates with Chemotherapy Induced Peripheral Neuropathy

Abstract
:1. Introduction
2. Methods
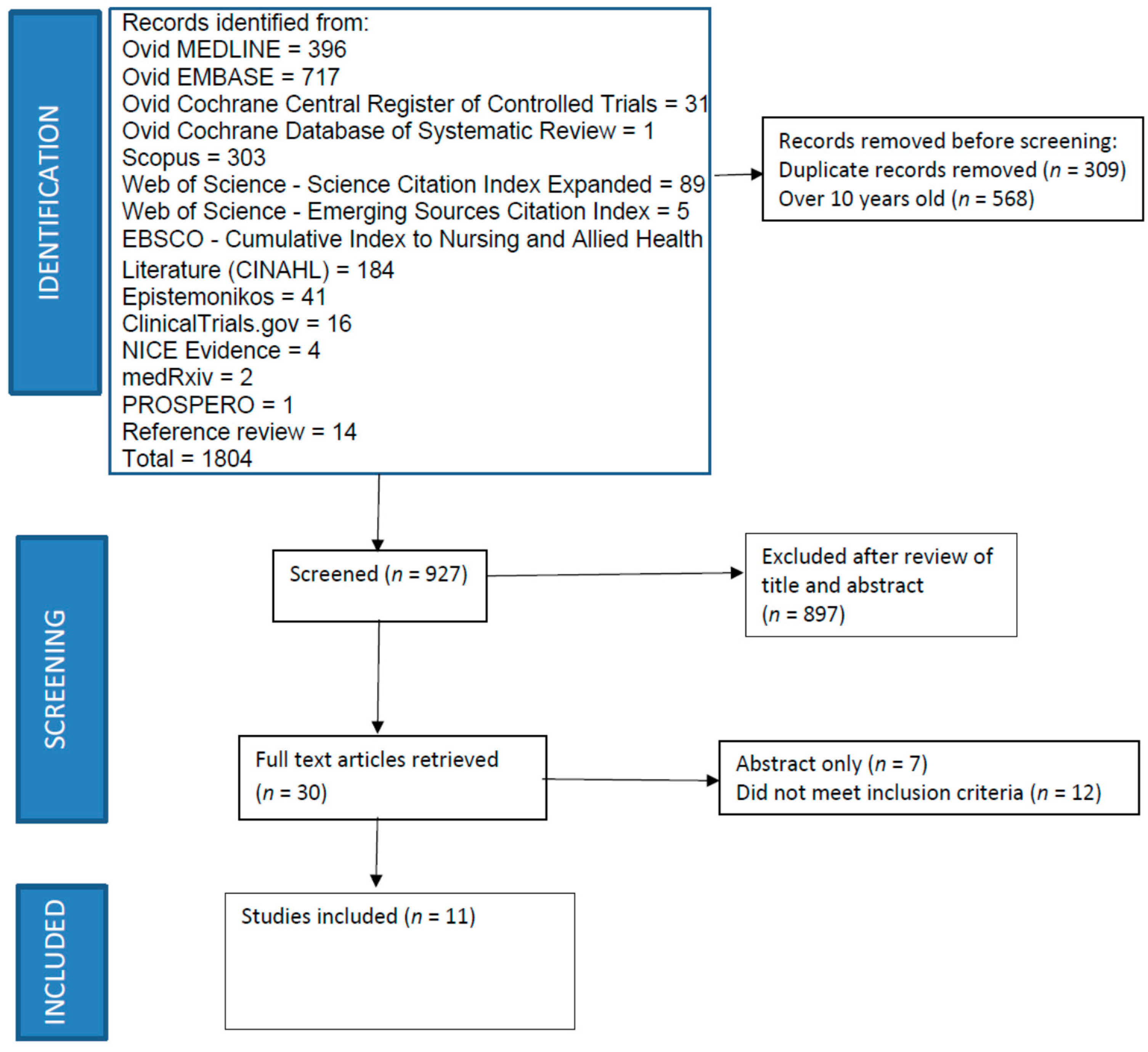
Search Strategy
3. Results
3.1. Methodological Quality
3.2. Study Characteristics
3.3. Results by Chemotherapy Type
3.3.1. Platinum-Based Chemotherapies
3.3.2. Taxanes
3.3.3. Taxanes or Platinums
3.3.4. Other Agents
3.4. Results by Laboratory Parameter
3.4.1. Hemoglobin
3.4.2. Vitamin D Levels
3.4.3. Magnesium Levels
3.4.4. Albumin and Prealbumin
3.4.5. Glucose/Glycosylated Hemoglobin
3.4.6. Vitamin E
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sałat, K. Chemotherapy-induced peripheral neuropathy: Part 1-current state of knowledge and perspectives for pharmacotherapy. Pharmacol. Rep. 2020, 72, 486–507. [Google Scholar] [CrossRef]
- Ewertz, M.; Qvortrup, C.; Eckhoff, L. Chemotherapy-induced peripheral neuropathy in patients treated with taxanes and platinum derivatives. Acta Oncol. 2015, 54, 587–591. [Google Scholar] [CrossRef]
- Zajączkowska, R.; Kocot-Kępska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Hsu, H.T.; Wu, L.M.; Lin, P.C.; Juan, C.H.; Huang, Y.Y.; Chou, P.L.; Chen, J.L. Emotional distress and quality of life during folinic acid, fluorouracil, and oxaliplatin in colorectal cancer patients with and without chemotherapy-induced peripheral neuropathy: A cross-sectional study. Medicine 2020, 99, e19029. [Google Scholar] [CrossRef]
- Soveri, L.M.; Lamminmäki, A.; Hänninen, U.A.; Karhunen, M.; Bono, P.; Osterlund, P. Long-term neuropathy and quality of life in colorectal cancer patients treated with oxaliplatin containing adjuvant chemotherapy. Acta Oncol. 2019, 58, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Timmins, H.C.; Mizrahi, D.; Li, T.; Kiernan, M.C.; Goldstein, D.; Park, S.B. Metabolic and lifestyle risk factors for chemotherapy-induced peripheral neuropathy in taxane and platinum-treated patients: A systematic review. J. Cancer Surviv. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gwathmey, K.G.; Grogan, J. Nutritional neuropathies. Muscle Nerve 2020, 62, 13–29. [Google Scholar] [CrossRef]
- Saboor, M.; Zehra, A.; Qamar, K. Moinuddin Disorders associated with malabsorption of iron: A critical review. Pak. J. Med. Sci. 2015, 31, 1549–1553. [Google Scholar] [PubMed]
- Jennaro, T.S.; Fang, F.; Kidwell, K.M.; Smith, E.M.L.; Vangipuram, K.; Burness, M.L.; Griggs, J.J.; Van Poznak, C.; Hayes, D.F.; Henry, N.L.; et al. Vitamin D deficiency increases severity of paclitaxel-induced peripheral neuropathy. Breast Cancer Res. Treat. 2020, 180, 707–714. [Google Scholar] [CrossRef]
- Robertson, J.; Raizer, J.; Hodges, J.S.; Gradishar, W.; Allen, J.A. Risk factors for the development of paclitaxel-induced neuropathy in breast cancer patients. J. Peripher. Nerv. Syst. 2018, 23, 129–133. [Google Scholar] [CrossRef]
- Grim, J.; Ticha, A.; Hyspler, R.; Valis, M.; Zadak, Z. Selected Risk Nutritional Factors for Chemotherapy-Induced Polyneuropathy. Nutrients 2017, 9, 535. [Google Scholar] [CrossRef] [Green Version]
- Ottaiano, A.; Nappi, A.; Tafuto, S.; Nasti, G.; De Divitiis, C.; Romano, C.; Cassata, A.; Casaretti, R.; Silvestro, L.; Avallone, A.; et al. Diabetes and Body Mass Index Are Associated with Neuropathy and Prognosis in Colon Cancer Patients Treated with Capecitabine and Oxaliplatin Adjuvant Chemotherapy. Oncology 2016, 90, 36–42. [Google Scholar] [CrossRef]
- Shahriari-Ahmadi, A.; Fahimi, A.; Payandeh, M.; Sadeghi, M. Prevalence of Oxaliplatin-induced Chronic Neuropathy and Influencing Factors in Patients with Colorectal Cancer in Iran. Asian Pac. J. Cancer Prev. 2015, 16, 7603–7606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincenzi, B.; Frezza, A.M.; Schiavon, G.; Spoto, C.; Silvestris, N.; Addeo, R.; Catalano, V.; Graziano, F.; Santini, D.; Tonini, G. Identification of clinical predictive factors of oxaliplatin-induced chronic peripheral neuropathy in colorectal cancer patients treated with adjuvant Folfox IV. Support. Care Cancer 2013, 21, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Winkels, R.M.; van Brakel, L.; van Baar, H.; Beelman, R.B.; van Duijnhoven, F.J.B.; Geijsen, A.; van Halteren, H.K.; Hansson, B.M.E.; Richie, J.P.; Sun, D.; et al. Are Ergothioneine Levels in Blood Associated with Chronic Peripheral Neuropathy in Colorectal Cancer Patients Who Underwent Chemotherapy? Nutr. Cancer 2020, 72, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Saito, T.; Okamura, A.; Inoue, J.; Makiura, D.; Doi, H.; Yakushijin, K.; Matsuoka, H.; Sakai, Y.; Ono, R. Anemia Is a Novel Predictive Factor for the Onset of Severe Chemotherapy-Induced Peripheral Neuropathy in Lymphoma Patients Receiving Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisolone Therapy. Oncol. Res. 2019, 27, 469–474. [Google Scholar] [CrossRef]
- Wang, J.; Udd, K.A.; Vidisheva, A.; Swift, R.A.; Spektor, T.M.; Bravin, E.; Ibrahim, E.; Treisman, J.; Masri, M.; Berenson, J.R. Low serum vitamin D occurs commonly among multiple myeloma patients treated with bortezomib and/or thalidomide and is associated with severe neuropathy. Support. Care Cancer 2016, 24, 3105–3110. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, N.; Cengiz, M. Predictive clinical factors of chronic peripheral neuropathy induced by oxaliplatin. Support. Care Cancer 2020, 28, 4781–4788. [Google Scholar] [CrossRef] [PubMed]
- Velasco, R.; Santos, C.; Soler, G.; Gil-Gil, M.; Pernas, S.; Galan, M.; Palmero, R.; Bruna, J. Serum micronutrients and prealbumin during development and recovery of chemotherapy-induced peripheral neuropathy. J. Peripher. Nerv. Syst. 2016, 21, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Popović, J.; Klajn, A.; Paunesku, T.; Ma, Q.; Chen, S.; Lai, B.; Stevanović, M.; Woloschak, G.E. Neuroprotective Role of Selected Antioxidant Agents in Preventing Cisplatin-Induced Damage of Human Neurons In Vitro. Cell. Mol. Neurobiol. 2019, 39, 619–636. [Google Scholar] [CrossRef] [Green Version]
- Solomon, L.R. Functional vitamin B12 deficiency in advanced malignancy: Implications for the management of neuropathy and neuropathic pain. Support. Care Cancer 2016, 24, 3489–3494. [Google Scholar] [CrossRef]
- Schmid, C.H. Discussion of “quantifying publication bias in meta-analysis” by Lin et al. Biometrics 2018, 74, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Timmins, H.C.; Li, T.; Goldstein, D.; Trinh, T.; Mizrahi, D.; Harrison, M.; Horvath, L.G.; Friedlander, M.; Kiernan, M.C.; Park, S.B. The impact of obesity on neuropathy outcomes for paclitaxel- and oxaliplatin-treated cancer survivors. J. Cancer Surviv. 2021, 1–10. [Google Scholar] [CrossRef]
- Mizrahi, D.; Park, S.B.; Li, T.; Timmins, H.C.; Trinh, T.; Au, K.; Battaglini, E.; Wyld, D.; Henderson, R.D.; Grimison, P.; et al. Hemoglobin, Body Mass Index, and Age as Risk Factors for Paclitaxel- and Oxaliplatin-Induced Peripheral Neuropathy. JAMA Netw. Open 2021, 4, e2036695. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Balamurugan, A.; Biddle, J.; Rollins, K.M. Diabetic neuropathy status and the concerns in underserved rural communities: Challenges and opportunities for diabetes educators. Diabetes Educ. 2011, 37, 536–548. [Google Scholar] [CrossRef] [PubMed]
- Nyrop, K.A.; Damone, E.M.; Deal, A.M.; Wheeler, S.B.; Charlot, M.; Reeve, B.B.; Basch, E.; Shachar, S.S.; Carey, L.A.; Reeder-Hayes, K.E.; et al. Patient-reported treatment toxicity and adverse events in Black and White women receiving chemotherapy for early breast cancer. Breast Cancer Res. Treat. 2021, 1–14. [Google Scholar] [CrossRef]
- Sugihara, K.; Ohtsu, A.; Shimada, Y.; Mizunuma, N.; Gomi, K.; Lee, P.H.; Gramont, A.; Rothenberg, M.L.; André, T.; Brienza, S.; et al. Analysis of neurosensory adverse events induced by FOLFOX4 treatment in colorectal cancer patients: A comparison between two Asian studies and four Western studies. Cancer Med. 2012, 1, 198–206. [Google Scholar] [CrossRef]
- Jordan, B.; Jahn, F.; Beckmann, J.; Unverzagt, S.; Müller-Tidow, C.; Jordan, K. Calcium and Magnesium Infusions for the Prevention of Oxaliplatin-Induced Peripheral Neurotoxicity: A Systematic Review. Oncology 2016, 90, 299–306. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Drug | Cancer Diagnosis | Neuropathy Measure | Percentage of Sample with Neuropathy |
|---|---|---|---|---|
| Grim et al. [12] | Paclitaxel | Breast | Michigan Neuropathy Screening Instrument | 60% 1 |
| Jennaro et al. [10] | Paclitaxel | Breast | EORTC CIPN-20 5 | 32.4% |
| Ottaiano et al. [13] | Oxaliplatin | Colorectal | CTCAE 6 | 17.7% |
| Robertson et al. [11] | Paclitaxel | Breast | TNS 7 | 42% |
| Saito et al. [17] | Vincristine | Lymphoma | CTCAE | 17.5% 2 |
| Shahriari-Ahmadi et al. [14] | Oxaliplatin | Colorectal | CTCAE | 80.7% |
| Velasco et al. [20] | Platinum or taxane | Colorectal, gastric, lung, or breast | TNS CTCAE Nerve conduction studies | 52% 4 |
| Vincenzi et al. [15] | Oxaliplatin | Colorectal | CTCAE | 40% |
| Wang et al. [18] | Thalidomide/velcade | Multiple myeloma | CTCAE FACT/GOG-NTX 8 | 59% |
| Winkels et al. [16] | Oxaliplatin/ capecitabine | Colorectal | CIPN20 | 81% |
| Yildirim et al. [19] | Oxaliplatin | Gastrointestinal (colorectal, gastric, or pancreatic) | CTCAE | 42% 2,3 |
| Reference | Country | Sample Size | Frequency (Percent) of Minority Race or Ethnicity | African American/Black 1 | Hispanic 1 | Asian 1 | Other 1 |
|---|---|---|---|---|---|---|---|
| Wang et al. [18] | USA | 109 | 21 (19.3) | 9 (8.3) | 5 (4.6) | 3 (2.8) | 4 (3.7) |
| Robertson et al. [11] | USA | 61 | 12 (19.1) | 7 (11.5) | 2 (3.3) | 3 (4.9) | 0 |
| Jennaro et al. [10] | USA | 37 | 3 (8.1) | Race/ethnicity only described as white or non-white. No non-white participants were in the vitamin D-deficient group. | |||
| Vincenzi et al. [15] | Italy | 169 | NR 1 | Race/ethnicity not described. | |||
| Ottaiano et al. [13] | Italy | 102 | NR | Race/ethnicity not described. | |||
| Shahriari-Ahmadi et al. [14] | Iran | 130 | NR | Race/ethnicity not described. | |||
| Saito et al. [17] | Japan | 40 | NR | Race/ethnicity not described. | |||
| Grim et al. [12] | Czech Republic | 70 | NR | Race/ethnicity not described. | |||
| Velasco et al. [20] | Spain | 113 | NR | Race/ethnicity not described. | |||
| Winkels et al. [16] | Netherlands | 159 | NR | Race/ethnicity not described. | |||
| Yildirim et al. [19] | Turkey | 186 | NR | Race/ethnicity not described. | |||
| Vincenzi et al. [15] | Wang et al. [18] | Jennaro et al. [10] | Robertson et al. [11] | Shahriari-Ahmadi et al. [14] | Saito et al. [17] | Ottaiano et al. [13] | Grim et al. [12] | Velasco et al. [20] | Winkels et al. [16] | Yildirim et al. [19] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (demographic data) | 169 | 109 | 37 | 61 | 130 | 40 | 102 | 70 | 113 | 159 | 186 |
| Diabetes/hyperglycemia 2 | 29 (17.2) | 11 (10) | 8 (21.6) | 4 (6.6) | 28 (21.5) | 7 (17.5) | 19 (18.7) | NR 1 (9.5) | 18 (16) | NR | NR |
| Renal failure 2 | 15 (8.9) | NR | NR | NR | NR | 5 (12.5) | NR | NR | NR | NR | NR |
| Hepatic dysfunction 2 | NR | NR | NR | NR | NR | 10 (25) | NR | NR | NR | NR | NR |
| Alcohol use 2 | 13 (7.7) | NR | 19 (51.4) | 38 (62.3) | 5 (3.8) | NR | NR | NR | NR | NR | NR |
| Tobacco use 2 | NR | NR | NR | NR | NR | NR | 66 (64.7) | NR | NR | NR | NR |
| Malnutrition 2 | NR | NR | NR | NR | NR | 12 (30) | NR | NR | NR | NR | NR |
| Overweight/obese 2 | NR | NR | NR | NR | NR | NR | 36 (35.3) | NR | NR | NR | NR |
| Hypertension 2 | NR | NR | NR | 14 (22.9) | NR | NR | 21 (20.6) | NR | NR | NR | 36 (19.4) |
| Electrolyte imbalance 2 | NR | NR | NR | NR | NR | 4 (10) | NR | NR | NR | NR | NR |
| High cholesterol 2 | NR | NR | NR | NR | NR | NR | 23 (22.5) | NR | NR | NR | NR |
| Hyperlipidemia 2 | NR | NR | NR | 13 (21.3) | NR | NR | NR | NR | NR | NR | NR |
| High triglycerides 2 | NR | NR | NR | NR | NR | NR | 21 (20.6) | NR | NR | NR | NR |
| Hypocalcemia | 34 (20) | NR | NR | NR | 25 (19.3) | NR | NR | NR | NR | NR | NR |
| Coronary artery disease | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 12 (6.5) |
| Dyslipidemia | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 14 (7.5) |
| Author | Nutritional Lab Measures Evaluated | Lab Measures Associated with CIPN |
|---|---|---|
| Grim et al. [12] | Vitamin B1 Vitamin B6 Omega 3 fatty acids Vitamin D | Vitamin D |
| Jennaro et al. [10] | Vitamin D Vitamin B12 Folate Homocysteine | Vitamin D |
| Ottaiano et al. [13] | Triglycerides Cholesterol HbA1c | None |
| Robertson et al. [11] | HbA1c Vitamin B12 Vitamin B6 Vitamin E Folate Lipid panel Albumin Prealbumin | Albumin |
| Saito et al. [17] | Glucose Albumin Hemoglobin Potassium | Hemoglobin |
| Shahriari-Ahmadi et al. [14] | Calcium Magnesium | Hemoglobin Magnesium |
| Velasco et al. [20] | Magnesium Vitamin B12 Prealbumin Vitamin E | Vitamin E Pre-albumin |
| Vincenzi et al. [15] | Calcium Magnesium Albumin Hemoglobin Folate Vitamin B12 | Hemoglobin Albumin Magnesium |
| Wang et al. [18] | Vitamin D | Vitamin D |
| Winkels et al. [16] | Ergothioneine | None |
| Yildirim et al. [19] | Blood glucose Vitamin D Hemoglobin Albumin Magnesium Triglycerides Calcium Sodium Potassium Vitamin B12 Folic acid | Blood glucose Vitamin D Hemoglobin Albumin Magnesium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tofthagen, C.; Tanay, M.; Perlman, A.; Starr, J.; Advani, P.; Sheffield, K.; Brigham, T. A Systematic Review of Nutritional Lab Correlates with Chemotherapy Induced Peripheral Neuropathy. J. Clin. Med. 2022, 11, 355. https://doi.org/10.3390/jcm11020355
Tofthagen C, Tanay M, Perlman A, Starr J, Advani P, Sheffield K, Brigham T. A Systematic Review of Nutritional Lab Correlates with Chemotherapy Induced Peripheral Neuropathy. Journal of Clinical Medicine. 2022; 11(2):355. https://doi.org/10.3390/jcm11020355
Chicago/Turabian StyleTofthagen, Cindy, Mary Tanay, Adam Perlman, Jason Starr, Pooja Advani, Katharine Sheffield, and Tara Brigham. 2022. "A Systematic Review of Nutritional Lab Correlates with Chemotherapy Induced Peripheral Neuropathy" Journal of Clinical Medicine 11, no. 2: 355. https://doi.org/10.3390/jcm11020355