
Prognostic Benefit of New Drugs for HFrEF: A Systematic Review and Network Meta-Analysis

 , , ,
, , ,
Abstract
:
1. Introduction
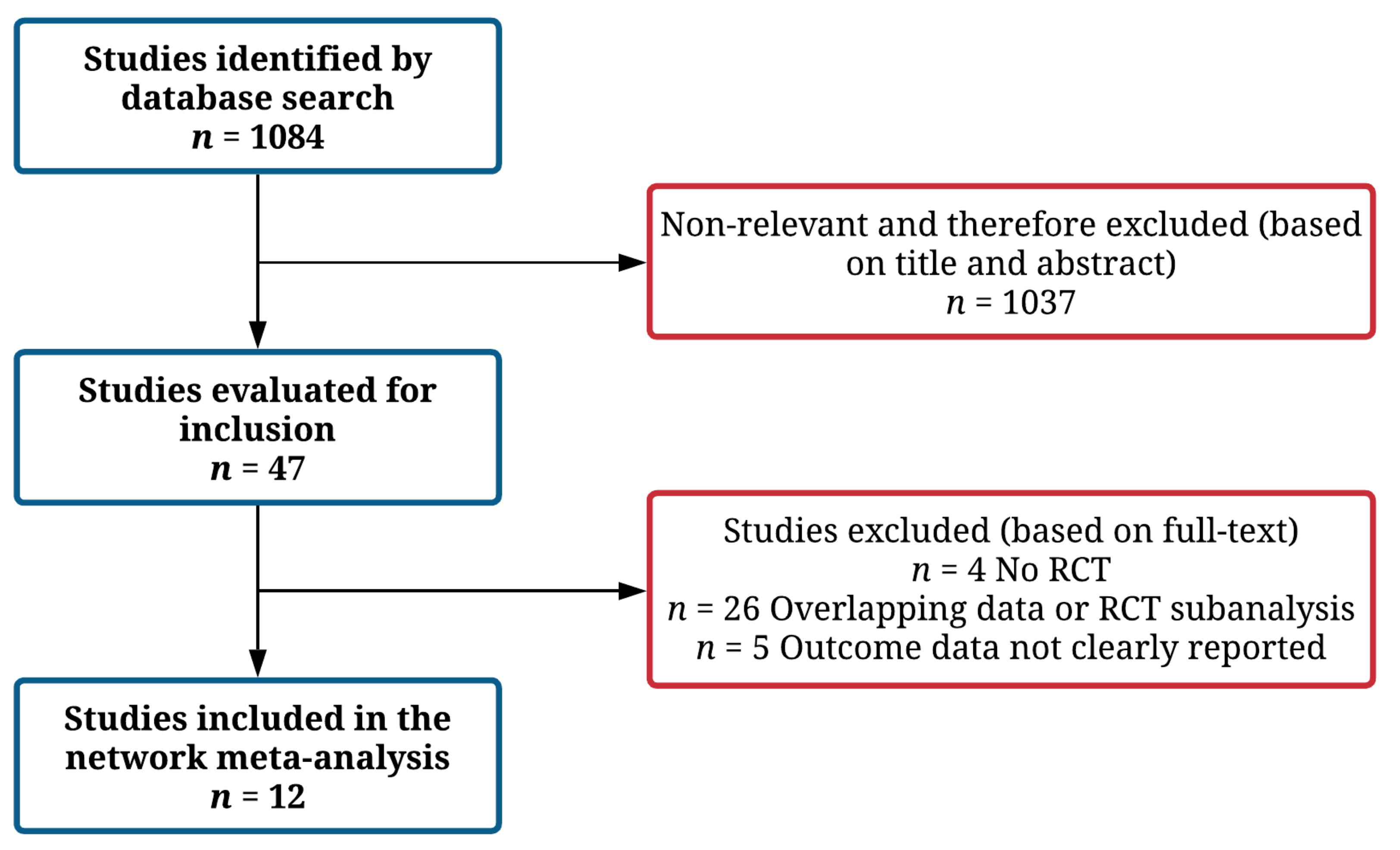
2. Materials and Methods
2.1. Study Endpoints
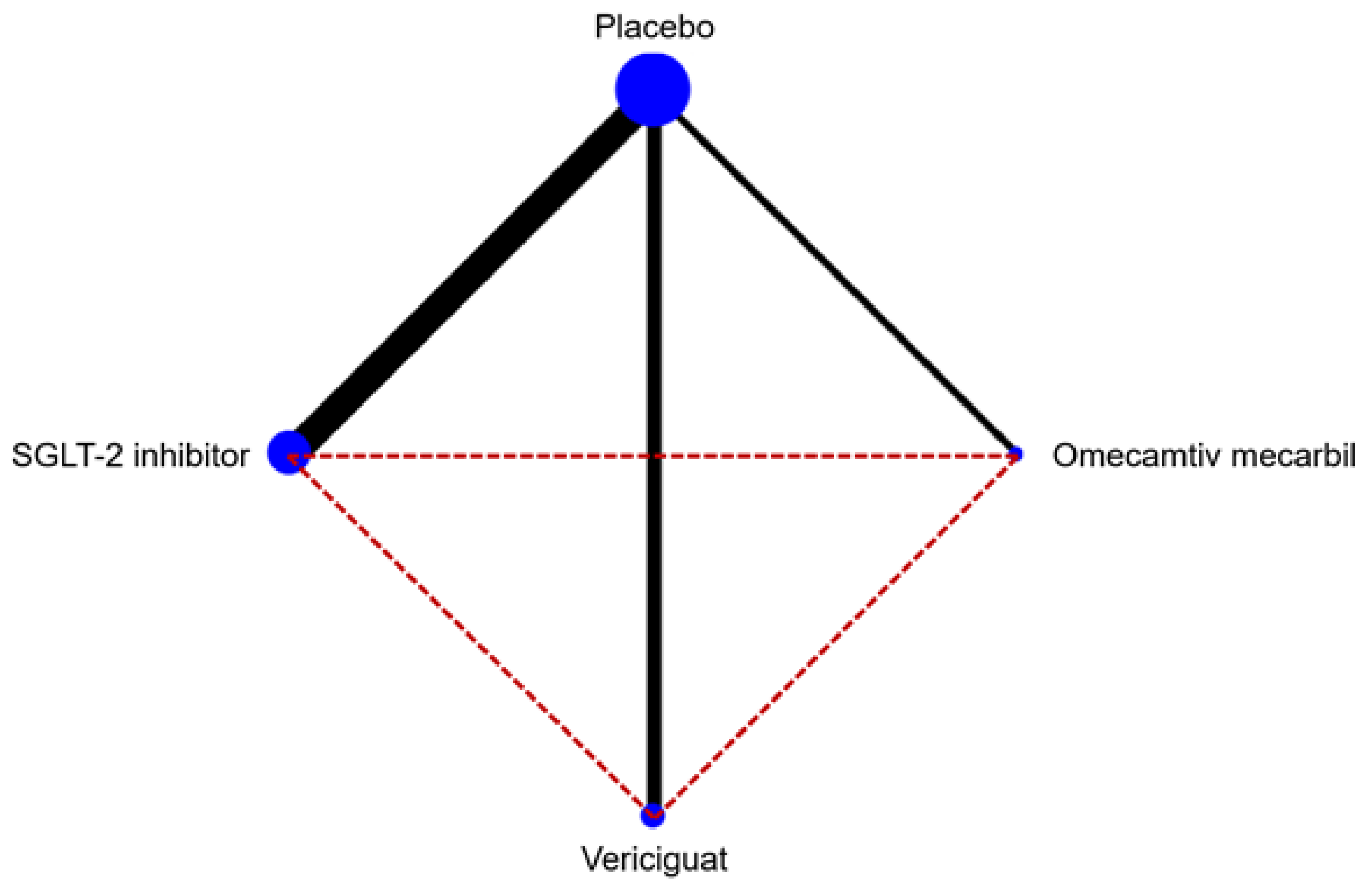
2.2. Statistical Analysis
3. Results
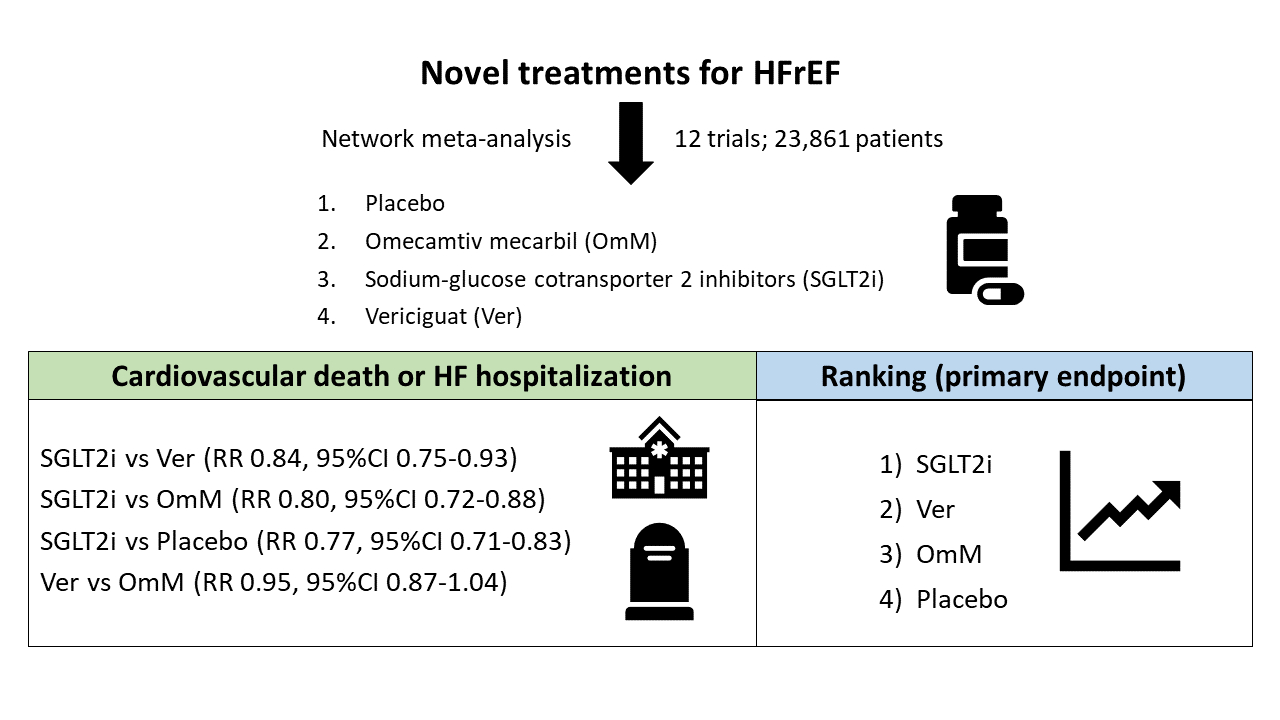
3.1. Primary Endpoint
3.2. Secondary Endpoints
3.3. Sensitivity Analyses
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEi | angiotensin-converting enzyme inhibitor |
| ARB | angiotensin receptor blocker |
| ARNI | angiotensin receptor-neprilysin inhibitor |
| CI | confidence interval |
| CVD | cardiovascular death |
| CVD-HF | cardiovascular death or heart failure hospitalization |
| HF | heart failure |
| HFH | heart failure hospitalization |
| HR | hazard ratio |
| HFrEF | heart failure with reduced ejection fraction |
| MRA | mineralocorticoid receptor antagonist |
References
- Metra, M.; Teerlink, J.R. Heart failure. Lancet 2017, 390, 1981–1995. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of Amer. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; Ezekowitz, J.; Hernandez, A.F.; Butler, J.; Lam, C.S.; Ponikowski, P.; Voors, A.A.; Jia, G.; et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2020, 382, 1883–1893. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Diaz, R.; Felker, G.M.; McMurray, J.J.V.; Metra, M.; Solomon, S.D.; Adams, K.F.; Anand, I.; Arias-Mendoza, A.; Biering-Sørensen, T.; et al. Cardiac Myosin Activation with Omecamtiv Mecarbil in Systolic Heart Failure. N. Engl. J. Med. 2021, 384, 105–116. [Google Scholar] [CrossRef]
- O’Meara, E.; McDonald, M.; Chan, M.; Ducharme, A.; Ezekowitz, J.A.; Giannetti, N.; Grzeslo, A.; Heckman, G.A.; Howlett, J.G.; Koshman, S.L.; et al. CCS/CHFS Heart Failure Guidelines: Clinical Trial Update on Functional Mitral Regurgitation, SGLT2 Inhibitors, ARNI in HFpEF, and Tafamidis in Amyloidosis. Can. J. Cardiol. 2020, 36, 159–169. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, C.M.; Cimino, G.; Pagnesi, M.; Dell’Aquila, A.; Tomasoni, D.; Ravera, A.; Inciardi, R.; Carubelli, V.; Vizzardi, E.; Nodari, S.; et al. Vericiguat for Heart Failure with Reduced Ejection Fraction. Curr. Cardiol. Rep. 2021, 23, 144. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Cooper, N.J.; Peters, J.; Lai, M.C.; Juni, P.; Wandel, S.; Palmer, S.; Paulden, M.; Conti, S.; Welton, N.J.; Abrams, K.R.; et al. How Valuable are Multiple Treatment Comparison Methods in Evidence-Based Health-Care Evaluation? Value Health 2011, 14, 371–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, D.M.; Dias, S.; Welton, N.J. Extending Treatment Networks in Health Technology Assessment: How Far Should We Go? Value Health 2015, 18, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: 2021. Available online: www.training.cochrane.org/handbook (accessed on 10 November 2021).
- Lumley, T. Network meta-analysis for indirect treatment comparisons. Stat. Med. 2002, 21, 2313–2324. [Google Scholar] [CrossRef]
- Caldwell, D.M.; Ades, T.; Higgins, J. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ 2005, 331, 897–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, G.; Ades, A.E. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Kato, E.; Silverman, M.G.; Mosenzon, O.; Zelniker, T.A.; Cahn, A.; Furtado, R.H.M.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; et al. Effect of Dapagliflozin on Heart Failure and Mortality in Type 2 Diabetes Mellitus. Circulation 2019, 139, 2528–2536. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Tang, F.; Khariton, Y.; Husain, M.; Inzucchi, S.E.; Mc-Guire, D.K.; Pitt, B.; Scirica, B.M.; Austin, B.; et al. Dapagliflozin Effects on Biomarkers, Symptoms, and Functional Status in Patients with Heart Failure With Reduced Ejection Fraction. Circulation 2019, 140, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Felker, G.M.; McMurray, J.J.V.; Solomon, S.D.; Adams, K.F.; Cleland, J.G.F.; Ezekowitz, J.A.; Goudev, A.; Macdonald, P.; Metra, M.; et al. Chronic Oral Study of Myosin Activation to Increase Contractility in Heart Failure (COSMIC-HF): A phase 2, pharmacokinetic, randomised, placebo-controlled trial. Lancet 2016, 388, 2895–2903. [Google Scholar] [CrossRef] [Green Version]
- Gheorghiade, M.; Greene, S.J.; Butler, J.; Filippatos, G.; Lam, C.S.P.; Maggioni, A.P.; Ponikowski, P.; Shah, S.J.; Solomon, S.D.; Kraigher-Krainer, E.; et al. Effect of Vericiguat, a Soluble Guanylate Cyclase Stimulator, on Natriuretic Peptide Levels in Patients With Worsening Chronic Heart Failure and Reduced Ejection Fraction: The SOCRATES-REDUCED Randomized Trial. JAMA 2015, 314, 2251–2262. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Lindenfeld, J.; Ponikowski, P.; Agostoni, P.; Butler, J.; Desai, A.S.; Filippatos, G.; Gniot, J.; Fu, M.; Gullestad, L.; et al. Effect of empagliflozin on exercise ability and symptoms in heart failure patients with reduced and preserved ejection fraction, with and without type 2 diabetes. Eur. Heart J. 2021, 42, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Omar, M.; Kistorp, C.; Poulsen, M.K.; Tuxen, C.; Gustafsson, I.; Køber, L.; Gustafsson, F.; Faber, J.; Fosbøl, E.L.; et al. Twelve weeks of treatment with empagliflozin in patients with heart failure and reduced ejection fraction: A double-blinded, randomized, and placebo-controlled trial. Am. Heart J. 2020, 228, 47–56. [Google Scholar] [CrossRef]
- Lee, M.M.Y.; Brooksbank, K.J.M.; Wetherall, K.; Mangion, K.; Roditi, G.; Campbell, R.T.; Berry, C.; Chong, V.; Coyle, L.; Docherty, K.F.; et al. Effect of Empagliflozin on Left Ventricular Volumes in Patients with Type 2 Diabetes, or Prediabetes, and Heart Failure with Reduced Ejection Fraction (SUGAR-DM-HF). Circulation 2020, 143, 516–525. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Vargas-Delgado, A.P.; Requena-Ibanez, J.A.; Garcia-Ropero, A.; Mancini, D.; Pinney, S.; Macaluso, F.; Sartori, S.; Roque, M.; Sabatel-Perez, F.; et al. Randomized Trial of Empagliflozin in Nondiabetic Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 243–255. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Packer, M. How Should We Sequence the Treatments for Heart Failure and a Reduced Ejection Fraction? A Redefinition of Evidence-Based Medicine. Circulation 2021, 143, 875–877. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Ferreira, J.P.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.V.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: A comparative analysis of three randomised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef]
- Seferović, P.M.; Coats, A.J.; Ponikowski, P.; Filippatos, G.; Huelsmann, M.; Jhund, P.S.; Polovina, M.M.; Komajda, M.; Seferović, J.; Sari, I.; et al. European Society of Cardiology/Heart Failure Association position paper on the role and safety of new glucose-lowering drugs in patients with heart failure. Eur. J. Heart Fail. 2020, 22, 196–213. [Google Scholar] [CrossRef] [Green Version]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Verma, S. Mechanisms of Cardiovascular Benefits of Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors. JACC Basic Transl. Sci. 2020, 5, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Seferović, P.M.; Fragasso, G.; Petrie, M.; Mullens, W.; Ferrari, R.; Thum, T.; Bauersachs, J.; Anker, S.D.; Ray, R.; Çavuşoğlu, Y.; et al. Sodium–glucose co-transporter 2 inhibitors in heart failure: Beyond glycaemic control. The position paper of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1495–1503. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrie, M.C.; Verma, S.; Docherty, K.; Inzucchi, S.E.; Anand, I.; Belohlávek, J.; Böhm, M.; Chiang, C.-E.; Chopra, V.K.; De Boer, R.A.; et al. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients with Heart Failure With and Without Diabetes. JAMA J. Am. Med Assoc. 2020, 323, 1353–1368. [Google Scholar] [CrossRef]
- Omar, M.; Jensen, J.; Ali, M.; Frederiksen, P.H.; Kistorp, C.; Videbæk, L.; Poulsen, M.K.; Tuxen, C.D.; Möller, S.; Gustafsson, F.; et al. Associations of Empagliflozin with Left Ventricular Volumes, Mass, and Function in Patients With Heart Failure and Reduced Ejection Fraction. JAMA Cardiol. 2021, 6, 836. [Google Scholar] [CrossRef]
- Nassif, M.E.; Qintar, M.; Windsor, S.L.; Jermyn, R.; Shavelle, D.M.; Tang, F.; Lamba, S.; Bhatt, K.; Brush, J.; Civitello, A.; et al. Empagliflozin Effects on Pulmonary Artery Pressure in Patients with Heart Failure. Circulation 2021, 143, 1673–1686. [Google Scholar] [CrossRef]
- Jansen, J.P.; Fleurence, R.; Devine, B.; Itzler, R.; Barrett, A.; Hawkins, N.; Lee, K.; Boersma, C.; Annemans, L.; Cappelleri, J.C. Interpreting Indirect Treatment Comparisons and Network Meta-Analysis for Health-Care Decision Making: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 1. Value Health 2011, 14, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Study | Year | Treatment | n Patients | Age (Years) | Male Sex (%) | EF (%) | Diabetes (%) | NT-proBNP (pg/mL) | Background HF Therapy | Follow-Up | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACEi/ARB (%) | Beta-Blocker (%) | ARNI (%) | MRA (%) | ||||||||||
| GALACTIC-HF [9] | 2021 | Omecamtiv mecarbil vs. Placebo | 8232 | 65 | 79 | 27 | 40 | 1971 | 87 * | 94 | 19 | 78 | 22 months (median) |
| COSMIC-HF [22] | 2016 | Omecamtiv mecarbil vs. Placebo | 298 | 63 | 82 | 29 | 39 | 1719 | 93 | 97 | 0 | 61 | 24 weeks |
| VICTORIA [8] | 2020 | Vericiguat vs. Placebo | 5050 | 67 | 76 | 29 | 47 | 2816 | 73 | 93 | 15 | 70 | 11 months (median) |
| SOCRATES-REDUCED [23] | 2015 | Vericiguat vs. Placebo | 183 | 68 | 82 | 29 | 49 | 3076 | 81 | 92 | 0 | 62 | 12 weeks |
| EMPEROR-Reduced [7] | 2020 | Empagliflozin vs. Placebo | 3730 | 67 | 76 | 27 | 50 | 1907 | 70 | 95 | 19 | 71 | 16 months (median) |
| EMPERIAL-Reduced [24] | 2020 | Empagliflozin vs. Placebo | 311 | 70 | 74 | 30 | 60 | 1489 | 55 | 95 | 37 | 58 | 12 weeks |
| Empire HF [25] | 2020 | Empagliflozin vs. Placebo | 190 | 64 | 85 | 30 | 17 | 594 | 96 * | 95 | 31 | 66 | 12 weeks |
| SUGAR-DM-HF [26] | 2021 | Empagliflozin vs. Placebo | 105 | 69 | 73 | 33 | 78 | 466 | 61 | 91 | 34 | 60 | 40 weeks |
| EMPA-TROPISM (ATRU-4) [27] | 2021 | Empagliflozin vs. Placebo | 84 | 62 | 64 | 36 | 0 | NA | 42 | 88 | 43 | 33 | 6 months |
| DAPA-HF [6] | 2019 | Dapagliflozin vs. Placebo | 4744 | 66 | 77 | 31 | 42 | 1437 | 84 | 96 | 11 | 71 | 18 months (median) |
| DECLARE-TIMI 58 (HFrEF subgroup) [20] | 2019 | Dapagliflozin vs. Placebo | 671 | 63 | 84 | 38 | 100 | NA | 88 | 88 | NA | 30 | 4.2 years (median) |
| DEFINE-HF [21] | 2019 | Dapagliflozin vs. Placebo | 263 | 61 | 73 | 26 | 62 | 1136 | 59 | 97 | 33 | 61 | 12 weeks |
| Endpoint | Placebo | SGLT2i | Vericiguat | Omecamtiv Mecarbil |
|---|---|---|---|---|
| CV death or HF hospitalization | ||||
| Placebo | 0.77 (0.71–0.83) | 0.92 (0.85–0.99) | 0.96 (0.91–1.02) | |
| 1.30 (1.20–1.41) | SGLT2i | 1.19 (1.07–1.33) | 1.25 (1.13–1.39) | |
| 1.09 (1.01–1.17) | 0.84 (0.75–0.93) | Vericiguat | 1.05 (0.96–1.15) | |
| 1.04 (0.98–1.10) | 0.80 (0.72–0.88) | 0.95 (0.87–1.04) | Omecamtiv mecarbil | |
| CV death | ||||
| Placebo | 0.85 (0.75–0.96) | 0.94 (0.83–1.06) | 1.01 (0.93–1.10) | |
| 1.18 (1.04–1.33) | SGLT2i | 1.10 (0.93–1.31) | 1.19 (1.03–1.38) | |
| 1.07 (0.95–1.21) | 0.91 (0.76–1.08) | Vericiguat | 1.08 (0.93–1.25) | |
| 0.99 (0.91–1.08) | 0.84 (0.72–0.98) | 0.93 (0.80–1.08) | Omecamtiv mecarbil | |
| All-cause death | ||||
| Placebo | 0.86 (0.77–0.95) | 0.96 (0.86–1.07) | 1.00 (0.93–1.07) | |
| 1.16 (1.05–1.29) | SGLT2i | 1.11 (0.96–1.29) | 1.16 (1.02–1.32) | |
| 1.05 (0.94–1.16) | 0.90 (0.77–1.04) | Vericiguat | 1.04 (0.92–1.19) | |
| 1.00 (0.93–1.08) | 0.86 (0.76–0.98) | 0.96 (0.84–1.09) | Omecamtiv mecarbil | |
| HF hospitalization | ||||
| Placebo | 0.73 (0.66–0.81) | 0.92 (0.84–1.00) | 0.97 (0.90–1.04) | |
| 1.37 (1.24–1.52) | SGLT2i | 1.26 (1.10–1.44) | 1.33 (1.17–1.50) | |
| 1.09 (1.00–1.19) | 0.79 (0.69–0.91) | Vericiguat | 1.05 (0.94–1.18) | |
| 1.03 (0.97–1.11) | 0.75 (0.67–0.85) | 0.95 (0.85–1.06) | Omecamtiv mecarbil |
| Treatment | Pbest | SUCRA |
|---|---|---|
| CV death or HF hospitalization | ||
| Placebo | 0.29 | 3.91 |
| SGLT2i | 77.24 | 99.97 |
| Vericiguat | 15.92 | 61.54 |
| Omecamtiv mecarbil | 6.55 | 34.58 |
| CV death | ||
| Placebo | 1.49 | 24.76 |
| SGLT2i | 61.14 | 95.09 |
| Vericiguat | 25.89 | 60.85 |
| Omecamtiv mecarbil | 11.48 | 19.30 |
| Any death | ||
| Placebo | 3.66 | 23.49 |
| SGLT2i | 64.97 | 96.92 |
| Vericiguat | 28.40 | 53.75 |
| Omecamtiv mecarbil | 2.97 | 25.83 |
| HF hospitalization | ||
| Placebo | 0.48 | 6.40 |
| SGLT2i | 78.21 | 99.99 |
| Vericiguat | 19.12 | 59.60 |
| Omecamtiv mecarbil | 2.19 | 34.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagnesi, M.; Baldetti, L.; Aimo, A.; Inciardi, R.M.; Tomasoni, D.; Vizzardi, E.; Vergaro, G.; Emdin, M.; Lombardi, C.M. Prognostic Benefit of New Drugs for HFrEF: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2022, 11, 348. https://doi.org/10.3390/jcm11020348
Pagnesi M, Baldetti L, Aimo A, Inciardi RM, Tomasoni D, Vizzardi E, Vergaro G, Emdin M, Lombardi CM. Prognostic Benefit of New Drugs for HFrEF: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2022; 11(2):348. https://doi.org/10.3390/jcm11020348
Chicago/Turabian StylePagnesi, Matteo, Luca Baldetti, Alberto Aimo, Riccardo Maria Inciardi, Daniela Tomasoni, Enrico Vizzardi, Giuseppe Vergaro, Michele Emdin, and Carlo Mario Lombardi. 2022. "Prognostic Benefit of New Drugs for HFrEF: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 11, no. 2: 348. https://doi.org/10.3390/jcm11020348