

Development of an ICT-Based Exergame Program for Children with Developmental Disabilities
Abstract
:1. Introduction
2. Materials and Methods
2.1. Developing an ICT-Based Exergame for Children with Developmental Disabilities
2.1.1. Physical Fitness
2.1.2. Fundamental Motor Skills
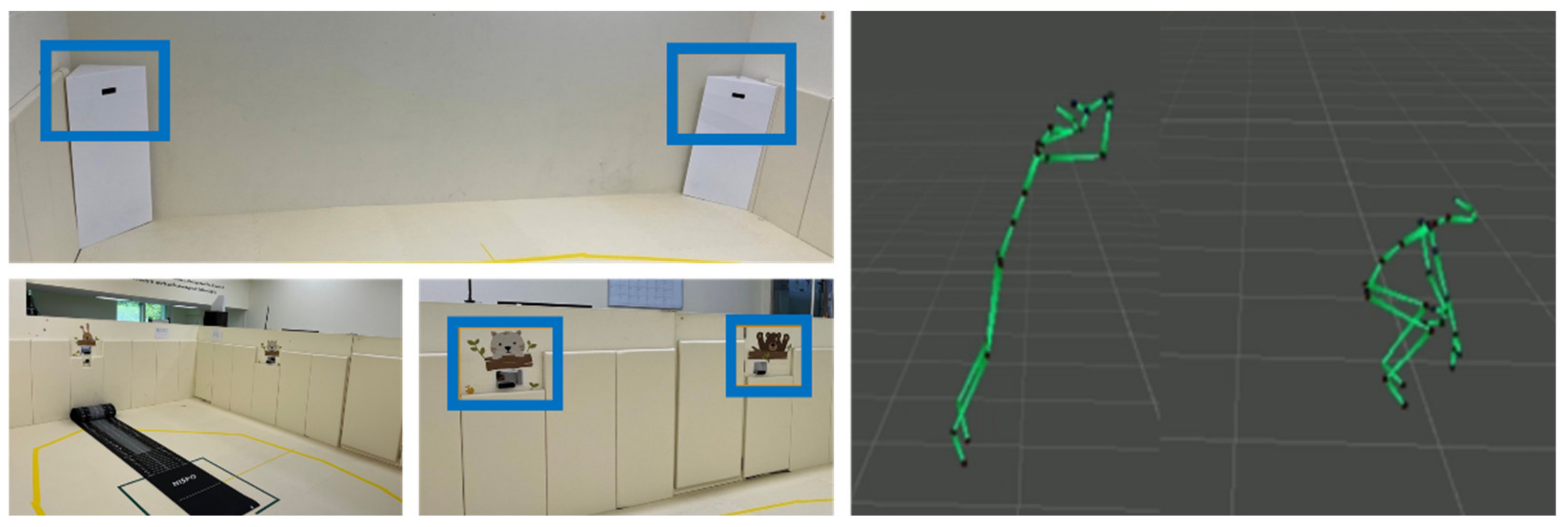
2.2. Setting
2.3. Examining the Impact of ICT-Based Exergame Program
2.3.1. Participants
2.3.2. Muscular Strength Test
2.3.3. Gross Motor Development Test
2.4. Procedure
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American College of Sports Medicine. What is Exergaming? Available online: https://healthysd.gov/what-is-exergaming-5/ (accessed on 10 August 2022).
- Barkley, R.A.; Anderson, D.L.; Kruesi, M. A Pilot Study of the Effects of Atomoxetine on Driving Performance in Adults with ADHD. J. Atten. Disord. 2007, 10, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.L.; Bialik, P.; Kizony, R. Virtual Reality Provides Leisure Time Opportunities for Young Adults with Physical and Intellectual Disabilities. Cyberpsychol. Behav. 2003, 6, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daley, A.J. Can Exergaming Contribute to Improving Physical Activity Levels and Health Outcomes in Children? Spec. Artic. Pediatr. 2009, 124, 763. [Google Scholar] [CrossRef] [PubMed]
- Mcmahon, D.D.; Barrio, B.; Mcmahon, A.K.; Tutt, K.; Firestone, J. Virtual Reality Exercise Games for High School Students with Intellectual and Developmental Disabilities. J. Spec. Educ. Technol. 2020, 35, 87–96. [Google Scholar] [CrossRef] [Green Version]
- Boger, J.; Eisapour, M.; Domenicucci, L.; Cao, S. Design of Virtual Reality Exergame to Promote Upper-Body Movement for Older Adults with Dementia. J. Rehabil. Eng. Assist. Technol. Soc. Korea 2017, 12, 91–94. [Google Scholar]
- Caro, K.; Morales-Villaverde, L.M.; Gotfrid, T.; Martinez-Garcia, A.I.; Kurniawan, S. Motivating Adults with Developmental Disabilities to Perform Motor Coordination Exercises Using Exergames. In Proceedings of the 4th EAI International Conference on Smart Objects and Technologies for Social Good, New York, NY, USA, 28–30 November 2018; pp. 183–189. [Google Scholar] [CrossRef]
- Perrot, A.; Maillot, P.; le Foulon, A.; Rebillat, A.-S. Effect of Exergaming on Physical Fitness, Functional Mobility, and Cognitive Functioning in Adults with Down Syndrome. Am. J. Intellect. Dev. Disabil. 2021, 126, 34–44. [Google Scholar] [CrossRef]
- Christison, A.; Khan, H.A. Exergaming for Health: A Community-Based Pediatric Weight Management Program Using Active Video Gaming. Clin. Pediatr. 2012, 51, 382–388. [Google Scholar] [CrossRef]
- Ma, M.; Jain, L. Future Trends of Virtual, Augmented Reality, and Games for Health. In Virtual, Augmented Reality and Serious Games for Healthcare 1; Springer: Berlin/Heidelberg, 2014; pp. 1–8. [Google Scholar]
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A. Estimated Prevalence of Autism and Other Developmental Disabilities Following Questionnaire Changes in the 2014 National Health Interview Survey. Natl. Health Stat. Rep. 2014, 87, 1–20. [Google Scholar]
- Association American Psychiatric. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association (APA): Washington, DC, USA, 2013. [Google Scholar]
- Comer, R.J. Fundamentals of Abnormal Psychology 8e & Launchpad for Fundamentals of Abnormal Psychology 8e (Six-Months Access); Worth Publishers Inc.: Duffield, UK, 2016. [Google Scholar]
- Macdonald, M.; Lord, C.; Ulrich, D. The Relationship of Motor Skills and Adaptive Behavior Skills in Young Children with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2013, 7, 1383–1390. [Google Scholar] [CrossRef] [Green Version]
- Rintala, P.; Loovis, E.M. Measuring Motor Skills in Finnish Children with Intellectual Disabilities. Percept. Mot. Skills 2013, 116, 294–303. [Google Scholar] [CrossRef]
- Staples, K.L.; Reid, G. Fundamental Movement Skills and Autism Spectrum Disorders. J. Autism Dev. Disord. 2010, 40, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Westendorp, M.; Houwen, S.; Hartman, E.; Visscher, C. Are Gross Motor Skills and Sports Participation Related in Children with Intellectual Disabilities? Res. Dev. Disabil. 2011, 32, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.; Daly, D.; Theodorou, F.; Caron, C.; Simons, J.; Andoniadou, E. Validity and Reliability of the TGMD-2 in 7–10-Year-Old Flemish Children with Intellectual Disability. Adapt. Phys. Act. Q. 2008, 25, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, J.; Jeffrey, S.; May, T.; Rinehart, N.J.; Barnett, L.M. Does Playing a Sports Active Video Game Improve Object Control Skills of Children with Autism Spectrum Disorder? J. Sport Health Sci. 2017, 6, 17–24. [Google Scholar] [CrossRef]
- Liu, T.; Breslin, C.M.; ElGarhy, S. Motor Skill Assessment in Autism Spectrum Disorder: A Case Study. Phys. Educ. 2017, 74, 239–254. [Google Scholar] [CrossRef]
- Lloyd, M.; Macdonald, M.; Lord, C. Motor Skills of Toddlers with Autism Spectrum Disorders. Autism 2013, 17, 133–146. [Google Scholar] [CrossRef] [Green Version]
- Allen, K.A.; Bredero, B.; van Damme, T.; Ulrich, D.A.; Simons, J. Test of Gross Motor Development-3 (TGMD-3) with the Use of Visual Supports for Children with Autism Spectrum Disorder: Validity and Reliability. J. Autism Dev. Disord. 2017, 47, 813–833. [Google Scholar] [CrossRef]
- Block, M.E. A Teacher’s Guide to Adapted Physical Education including Students with Disabilities in Sports and Recreation, 4th ed.; Brookes Publishing: Baltimore, MD, USA, 2016. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1. [Google Scholar] [CrossRef]
- Case, L.; Ross, S.; Yun, J. Physical Activity Guideline Compliance among a National Sample of Children with Various Developmental Disabilities. Disabil. Health J. 2020, 13, 100881. [Google Scholar] [CrossRef]
- Tybor, D.J.; Eliasziw, M.; Kral, T.V.E.; Segal, M.; Sherwood, N.E.; Sikich, L.; Stanish, H.; Bandini, L.; Curtin, C.; Must, A. Parental Concern Regarding Obesity in Children with Autism Spectrum Disorder in the United States: National Survey of Children’s Health 2016. Disabil. Health J. 2019, 12, 126–130. [Google Scholar] [CrossRef]
- McCoy, S.M.; Jakicic, J.M.; Gibbs, B.B. Comparison of Obesity, Physical Activity, and Sedentary Behaviors between Adolescents with Autism Spectrum Disorders and without. J. Autism Dev. Disord. 2016, 46, 2317–2326. [Google Scholar] [CrossRef] [PubMed]
- Must, A.; Curtin, C.; Hubbard, K.; Sikich, L.; Bedford, J.; Bandini, L. Obesity Prevention for Children with Developmental Disabilities. Curr. Obes. Rep. 2014, 3, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, J.T.; Bryan, R.R.; McCubbin, J.A. Daily Physical Activity Levels of Elementary School-Aged Children with and without Mental Retardation. J. Dev. Phys. Disabil. 2008, 20, 365–378. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Curtis, A. Measuring Physical Activity in Children and Youth Living with Intellectual Disabilities: A Systematic Review. Res. Dev. Disabil. 2013, 34, 72–86. [Google Scholar] [CrossRef]
- Whitt-Glover, M.C.; O’Neill, K.L.; Stettler, N. Physical Activity Patterns in Children with and without Down Syndrome. Pediatr. Rehabil. 2006, 9, 158–164. [Google Scholar] [CrossRef]
- Bandini, L.G.; Gleason, J.; Curtin, C.; Lividini, K.; Anderson, S.E.; Cermak, S.A.; Maslin, M.; Must, A. Comparison of Physical Activity between Children with Autism Spectrum Disorders and Typically Developing Children. Autism 2013, 17, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Esposito, P.E.; Macdonald, M.; Hornyak, J.E.; Ulrich, D.A. Physical Activity Patterns of Youth with Down Syndrome. Intellect. Dev. Disabil. 2012, 50, 109–119. [Google Scholar] [CrossRef]
- MacDonald, M.; Esposito, P.; Ulrich, D. The Physical Activity Patterns of Children with Autism. BMC Res. Notes 2011, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.Y.; Chu, C.H.; Tsai, C.L.; Sung, M.C.; Huang, C.Y.; Ma, W.Y. The Impacts of Physical Activity Intervention on Physical and Cognitive Outcomes in Children with Autism Spectrum Disorder. Autism 2017, 21, 190–202. [Google Scholar] [CrossRef]
- Whitehead, D. Before the Cradle and beyond the Grave: A Lifespan/Settings-Based Framework for Health Promotion. J. Clin. Nurs. 2011, 20, 2183–2194. [Google Scholar] [CrossRef]
- Hartman, E.; Smith, J.; Westendorp, M.; Visscher, C. Development of Physical Fitness in Children with Intellectual Disabilities. J. Intellect. Disabil. Res. 2015, 59, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Agiovlasitis, S.; Yun, J.; Jin, J.; McCubbin, J.A.; Motl, R.W. Physical Activity Promotion for Persons Experiencing Disability: The Importance of Interdisciplinary Research and Practice. Adapt. Phys. Act. Q. 2018, 35, 437–457. [Google Scholar] [CrossRef] [PubMed]
- Jeoung, B. Motor Proficiency Differences among Students with Intellectual Disabilities, Autism, and Developmental Disability. J. Exerc. Rehabil. 2018, 14, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Phillips, S.; Curtin, C.; Bandini, L.G. Barriers to Physical Activity in Children with Autism Spectrum Disorders: Relationship to Physical Activity and Screen Time. J. Phys. Act. Health 2015, 12, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichow, B.; Steiner, A.M.; Volkmar, F. Social Skills Groups for People Aged 6 to 21 with Autism Spectrum Disorders (ASD). Campbell Syst. Rev. 2012, 8, 1–76. [Google Scholar] [CrossRef]
- Annema, J.-H.; Verstraete, M.; Vanden Abeele, V.; Desmet, S.; Geerts, D. Videogames in Therapy: A Therapist’s Perspective. In Proceedings of the 3rd International Conference on Fun and Games, Leuven, Belgium, 15–17 September 2010; pp. 94–98. [Google Scholar]
- Wiemeyer, J.; Deutsch, J.; Malone, L.A.; Rowland, J.L.; Swartz, M.C.; Xiong, J.; Zhang, F.F. Recommendations for the Optimal Design of Exergame Interventions for Persons with Disabilities: Challenges, Best Practices, and Future Research. Games Health J. 2015, 4, 58. [Google Scholar] [CrossRef] [Green Version]
- Njelesani, J.; Leckie, K.; Drummond, J.; Cameron, D. Parental Perceptions of Barriers to Physical Activity in Children with Developmental Disabilities Living in Trinidad and Tobago. Disabil. Rehabil. 2015, 37, 290–295. [Google Scholar] [CrossRef]
- Kwon, H.; Yang, H. Physical Activity Intervention Using Virtual Reality Technology for Individuals with Developmental Disabilities: A Literature Review. Korean J. Adapt. Phys. Act. 2020, 28, 129–140. [Google Scholar]
- Lai, B.; Lee, E.; Frey, G.; Jung, T.; Wagatsuma, M.; Stanish, H.; Rimmer, J.H. Research Trends and Recommendations for Physical Activity Interventions among Children and Youth with Disabilities: A Review of Reviews. Adapt. Phys. Act. Q. 2020, 37, 211–234. [Google Scholar] [CrossRef]
- Navan, A.A.; Khaleghi, A.; Navan, A.A.; Khaleghi, A. Using Gamification to Improve the Education Quality of Children with Autism. Rev. Cient. 2020, 1, 90–106. [Google Scholar] [CrossRef]
- Klavina, A.; Ostrovska, K.; Campa, M. Fundamental Movement Skill and Physical Fitness Measures in Children with Disabilities. Eur. J. Adapt. Phys. Act. 2017, 10, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Frey, G.C.; Chow, B. Relationship between BMI, Physical Fitness, and Motor Skills in Youth with Mild Intellectual Disabilities. Int. J. Obes. 2006, 30, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Castelli, D.M.; Valley, J.A. The Relationship of Physical Fitness and Motor Competence to Physical Activity. J. Teach. Phys. Educ. 2007, 26, 358–374. [Google Scholar] [CrossRef]
- Goodway, J.; St, D.F. Dynamic Relationships between Motor Skill Competence and Health-Related Fitness in Youth. Pediatr. Exerc. Sci. 2014, 26, 231–241. [Google Scholar] [CrossRef]
- Rintala, P.; Asunta, P.; Lahti, J.; Loovis, E.M. Physical Fitness of Individuals with Intellectual Disability Who Have Special Olympics Experience. Eur. J. Adapt. Phys. Act. 2016, 9, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Yılmaz, A.; Karakas, G.; Kaya, H.B.; Yilmaz, A.; Karakaş, G.; Kaçay, Z. The Effects of Sportive Exercises on Physical Fitness of Children with Specific Learning Disability. The Effects of Sportive Exercises on Physical Fitness of the Effects of Sportive Exercises on Physical Fitness of Children with Specific Learning Disability. Acta Kinesiol. 2017, 11, 88–93. [Google Scholar]
- Case, L.; Yun, J. Video Modeling and Test of Gross Motor Development-3 Performance among Children with Autism Spectrum Disorder. Eur. J. Adapt. Phys. Act. 2018, 11, 3. [Google Scholar] [CrossRef]
- Staples, K.L.; Andrew Pitchford, E.; Ulrich, D.A. The Instructional Sensitivity of the Test of Gross Motor Development-3 to Detect Changes in Performance for Young Children with and without Down Syndrome. Adapt. Phys. Act. Q. 2020, 38, 95–108. [Google Scholar] [CrossRef]
- Brusseau, T.A.; Hannon, J.C.; Fu, Y.; Fang, Y.; Nam, K.; Goodrum, S.; Burns, R.D. Trends in Physical Activity, Health-Related Fitness, and Gross Motor Skills in Children during a Two-Year Comprehensive School Physical Activity Program. J. Sci. Med. Sport 2018, 21, 828–832. [Google Scholar] [CrossRef]
- Burns, R.D.; Fu, Y.; Hannon, J.C.; Brusseau, T.A. School Physical Activity Programming and Gross Motor Skills in Children. Am. J. Health Behav. 2017, 41, 591–598. [Google Scholar] [CrossRef]
- Webster, E.K.; Martin, C.K.; Staiano, A.E. Fundamental Motor Skills, Screen-Time, and Physical Activity in Preschoolers. J. Sport Health Sci. 2019, 8, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Maeng, H. The Impact of a Rater Training Program on the TGMD-3 Scoring Accuracy of Pre-Service Adapted Physical Education Teachers. Children 2022, 9, 881. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, F.; Vannozzi, G.; Camomilla, V.; Piacentini, M.F.; Boca, F.; Bortels, E.; Kathrein, E.; Magyar, A.; Verdone, F.; Sbriccoli, P. Motor Competence in Individuals with Down Syndrome: Is an Improvement Still Possible in Adulthood? Int. J. Environ. Res. Public Health 2022, 19, 2157. [Google Scholar] [CrossRef] [PubMed]
- Behan, S.; Belton, S.; Peers, C.; O’connor, N.E.; Issartel, J. Moving Well-Being Well: Investigating the Maturation of Fundamental Movement Skill Proficiency across Sex in Irish Children Aged Five to Twelve. J. Sports Sci. 2019, 37, 2604–2612. [Google Scholar] [CrossRef]
- Burns, R.; Brusseau, T.; Hannon, J. Multivariate Associations among Health-Related Fitness, Physical Activity, and TGMD-3 Test Items in Disadvantaged Children from Low-Income Families. Percept. Mot. Skills 2017, 124, 86–104. [Google Scholar] [CrossRef]
- Mellecker, R.; Lyons, E.J.; Baranowski, T. Disentangling Fun and Enjoyment in Exergames Using an Expanded Design, Play, Experience Framework: A Narrative Review. Games Health J. 2013, 2, 142. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.H.; Han, E.Y.; Kim, B.R.; Kim, S.M.; Im, S.H.; Lee, S.Y.; Hyun, C.W. Effectiveness of Commercial Gaming-Based Virtual Reality Movement Therapy on Functional Recovery of Upper Extremity in Subacute Stroke Patients. Ann. Rehabil. Med. 2014, 38, 485–493. [Google Scholar] [CrossRef]
- Hughes, T.F.; Flatt, J.D.; Fu, B.; Butters, M.A.; Chang, C.C.H.; Ganguli, M. Interactive Video Gaming Compared with Health Education in Older Adults with Mild Cognitive Impairment: A Feasibility Study. Int. J. Geriatr. Psychiatry 2014, 29, 890–898. [Google Scholar] [CrossRef] [Green Version]
- Maillot, P.; Perrot, A. The Braking Force in Walking: Age-Related Differences and Improvement in Older Adults with Exergame Training Multimodal Integration of Body Position and Vision View Project Emotions and Performance View Project. J. Aging Phys. Act. 2014, 22, 518–526. [Google Scholar] [CrossRef]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental Movement Skills in Children and Adolescents: Review of Associated Health Benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [Green Version]
- Barnett, L.; Cliff, K.; Morgan, P.; van Beurden, E. Adolescents’ Perception of the Relationship between Movement Skills, Physical Activity and Sport. Eur. Phys. Educ. Rev. 2013, 19, 271–285. [Google Scholar] [CrossRef]
- Soares, F.; Bryanton, C.; Bossé, J.; Brien, M.; Mclean, J.; Mccormick, A.; Sveistrup, H. Feasibility, Motivation, and Selective Motor Control: Virtual Reality Compared to Conventional Home Exercise in Children with Cerebral Palsy. Cyberpsychol. Behav. 2006, 9, 123–128. [Google Scholar]
- Schott, N.; Holfelder, B. Relationship between Motor Skill Competency and Executive Function in Children with Down’s Syndrome. J. Intellect. Disabil. Res. 2015, 59, 860–872. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Cattuzzo, M.T.; dos Santos Henrique, R.; Ré, A.H.N.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor Competence and Health Related Physical Fitness in Youth: A Systematic Review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Cognitive | Attractive | Psychomotor |
|---|---|---|---|
| Evaluation Subdomain |
|
|
|
| Category | Experiment Group | Control Group | |||||
|---|---|---|---|---|---|---|---|
| ASD (n = 15) | ID (n = 12) | Total (n = 27) | ASD (n = 15) | ID (n = 10) | Total (n = 25) | ||
| Gender | Female | 2 | 6 | 8 | 4 | 3 | 7 |
| Male | 13 | 6 | 19 | 11 | 7 | 18 | |
| Age a | 10.21 ± 1.64 | 10.08 ± 1.32 | 10.15 ± 1.51 | 10.07 ± 1.39 | 10.51 ± 1.57 | 10.24 ± 1.48 | |
| Height (cm) a | Pre-test | 145.4 ± 9.5 | 141.9 ± 9.3 | 143.8 ± 9.6 | 139.9 ± 8.9 | 136.5 ± 4.9 | 138.6 ± 7.8 |
| Post-test | 147.3 ± 9.3 | 144.6 ± 9.9 | 146.1 ± 9.7 | 141.9 ± 9.6 | 136.5 ± 4.9 | 138.6 ± 7.8 | |
| Weight (kg) a | Pre-test | 42.5 ± 7.6 | 38.9 ± 6.5 | 40.9 ± 7.4 | 33.6 ± 5.4 | 32.6 ± 3.9 | 33.2 ± 4.9 |
| Post-test | 42.41 ± 8.1 | 38.9 ± 7.2 | 40.9 ± 7.9 | 34.9 ± 5.3 | 34.9 ± 3.6 | 34.9 ± 4.7 | |
| BMI a | Pre-test | 29.1 ± 4.3 | 27.3 ± 3.5 | 28.3 ± 4.1 | 33.6 ± 5.4 | 23.8 ± 2.2 | 33.2 ± 4.9 |
| Post-test | 28.7 ± 4.7 | 26.7 ± 3.7 | 27.8 ± 4.4 | 24.6 ± 2.7 | 25.1 ± 1.9 | 24.8 ± 2.5 | |
| Category | Control | Experiment | F (1, 50) | p | |||
|---|---|---|---|---|---|---|---|
| Pre-Test a | Post-Test a | Pre-Test a | Post-Test a | ||||
| Standing long jump (cm) | 87.4 ± 23.1 | 85.6 ± 20.2 | 88.3 ± 24.9 | 98.8 ± 29.3 | 18.79 | 0.000 * | |
| Locomotor skill | Hop | 3.16 ± 1.19 | 3.16 ± 1.25 | 3.20 ± 1.70 | 5.08 ± 2.02 | 21.71 | 0.000 * |
| Horizontal jump | 4.68 ± 1.95 | 4.36 ± 1.49 | 4.96 ± 2.11 | 5.76 ± 1.82 | 3.39 | 0.072 | |
| Ball skill | Overhand throw | 2.20 ± 1.44 | 2.52 ± 1.17 | 1.84 ± 2.11 | 4.44 ± 1.60 | 27.94 | 0.000 * |
| Dribble | 2.20 ± 1.39 | 2.44 ± 1.24 | 1.92 ± 1.55 | 3.92 ± 1.83 | 12.95 | 0.000 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.; Maeng, H.; Chung, J. Development of an ICT-Based Exergame Program for Children with Developmental Disabilities. J. Clin. Med. 2022, 11, 5890. https://doi.org/10.3390/jcm11195890
Kwon H, Maeng H, Chung J. Development of an ICT-Based Exergame Program for Children with Developmental Disabilities. Journal of Clinical Medicine. 2022; 11(19):5890. https://doi.org/10.3390/jcm11195890
Chicago/Turabian StyleKwon, Hyunjin, Hyokju Maeng, and Jinwook Chung. 2022. "Development of an ICT-Based Exergame Program for Children with Developmental Disabilities" Journal of Clinical Medicine 11, no. 19: 5890. https://doi.org/10.3390/jcm11195890