
Influence of Rolfing Structural Integration on Active Range of Motion: A Retrospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Outcomes
2.2.1. AROM of the Shoulder
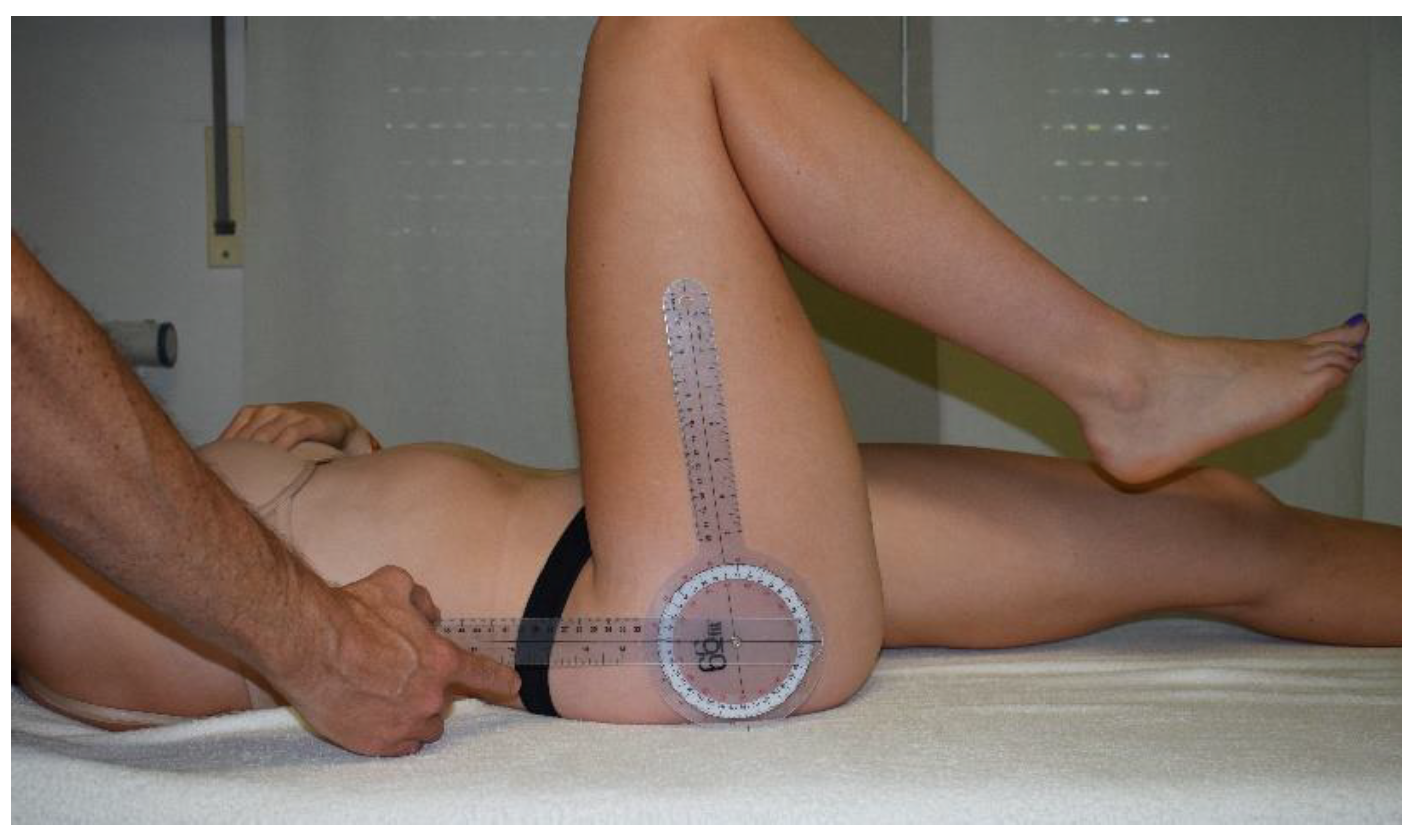
2.2.2. AROM of the Hip
2.2.3. Side Bend
2.2.4. Finger to Floor Distance
2.3. Statistical Analyses
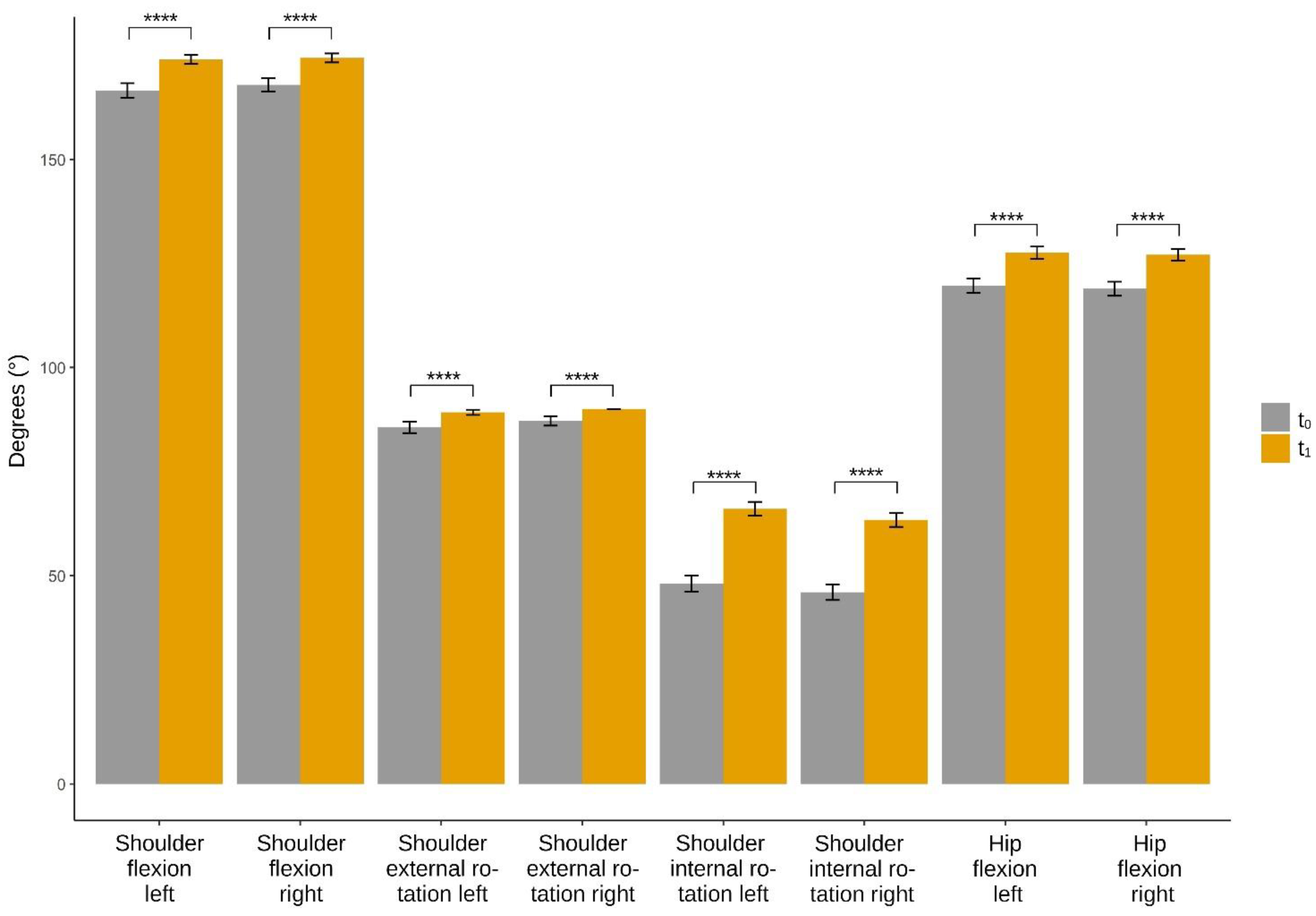
3. Results
4. Discussion
4.1. AROM of the Shoulder
4.2. AROM of the Hip
4.3. General Effects
4.4. Age-Related Treatment Effects
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schleip, R. Vom Aschenputtel Ins Rampenlicht: Die Wiederentdeckung Der Faszien in Der Muskuloskeletalen Medizin. Tamed Kongress J. 2012, 8, 6–9. [Google Scholar]
- Schleip, R.; Gabbiani, G.; Wilke, J.; Naylor, I.; Hinz, B.; Zorn, A.; Jäger, H.; Breul, R.; Schreiner, S.; Klingler, W. Fascia Is Able to Actively Contract and May Thereby Influence Musculoskeletal Dynamics: A Histochemical and Mechanographic Investigation. Front. Physiol. 2019, 10, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleip, R.; Duerselen, L.; Vleeming, A.; Naylor, I.L.; Lehmann-Horn, F.; Zorn, A.; Jaeger, H.; Klingler, W. Strain Hardening of Fascia: Static Stretching of Dense Fibrous Connective Tissues Can Induce a Temporary Stiffness Increase Accompanied by Enhanced Matrix Hydration. J. Bodyw. Mov. Ther. 2012, 16, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Krause, F. Myofascial Chains of the Upper Limb: A Systematic Review of Anatomical Studies. Clin. Anat 2019, 32, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Yucesoy, C.A. Epimuscular Myofascial Force Transmission Implies Novel Principles for Muscular Mechanics. Exerc. Sport Sci. 2010, 38, 128–134. [Google Scholar] [CrossRef]
- Wilke, J.; Debelle, H.; Tenberg, S.; Dilley, A.; Maganaris, C. Ankle Motion Is Associated With Soft Tissue Displacement in the Dorsal Thigh: An in Vivo Investigation Suggesting Myofascial Force Transmission Across the Knee Joint. Front. Physiol. 2020, 11, 180. [Google Scholar] [CrossRef] [Green Version]
- Griegel-Morris, P.; Larson, K.; Mueller-Klaus, K.; Oatis, C.A. Incidence of Common Postural Abnormalities in the Cervical, Shoulder, and Thoracic Regions and Their Association with Pain in Two Age Groups of Healthy Subjects. Phys. Ther. 1992, 72, 425–431. [Google Scholar] [CrossRef]
- Santos, T.S.; Oliveira, K.K.B.; Martins, L.V.; Vidal, A.P.C. Effects of Manual Therapy on Body Posture: Systematic Review and Meta-Analysis. Gait Posture 2022, 96, 280–294. [Google Scholar] [CrossRef]
- Elkjær, E.; Mikkelsen, M.B.; Michalak, J.; Mennin, D.S.; O’Toole, M.S. Expansive and Contractive Postures and Movement: A Systematic Review and Meta-Analysis of the Effect of Motor Displays on Affective and Behavioral Responses. Perspect. Psychol. Sci. 2022, 17, 276–304. [Google Scholar] [CrossRef]
- Threlkeld, A.J. The Effects of Manual Therapy on Connective Tissue. Phys. Ther. 1992, 72, 893–902. [Google Scholar] [CrossRef]
- Taylor, H.H.; Murphy, B. Altered Central Integration of Dual Somatosensory Input after Cervical Spine Manipulation. J. Manip. Physiol. Ther. 2010, 33, 178–188. [Google Scholar] [CrossRef]
- Haavik-Taylor, H.; Murphy, B. Cervical Spine Manipulation Alters Sensorimotor Integration: A Somatosensory Evoked Potential Study. Clin. Neurophysiol. 2007, 118, 391–402. [Google Scholar] [CrossRef]
- Rossettini, G.; Camerone, E.M.; Carlino, E.; Benedetti, F.; Testa, M. Context Matters: The Psychoneurobiological Determinants of Placebo, Nocebo and Context-Related Effects in Physiotherapy. Arch. Physiother. 2020, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Findley, T.; DeFilippis, J. Information for Clinical Health Care Practitioners; Rolfing Structural Integration—The Rolf Institute Research Committee: Seattle, WA, USA, 2005. [Google Scholar]
- Kasper-Jędrzejewska, M.; Jędrzejewski, G.; Ptaszkowska, L.; Ptaszkowski, K.; Schleip, R.; Halski, T. The Rolf Method of Structural Integration and Pelvic Floor Muscle Facilitation: Preliminary Results of a Randomized, Interventional Study. JCM 2020, 9, 3981. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, E. Structural Integration, an Alternative Method of Manual Therapy and Sensorimotor Education. J. Altern. Complement. Med. 2011, 17, 891–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleip, R. Fascial Plasticity—A New Neurobiological Explanation: Part 1. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Brandl, A.; Egner, C.; Schleip, R. Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial. Life 2021, 11, 845. [Google Scholar] [CrossRef]
- Schleip, R. Fascial Plasticity—A New Neurobiological Explanation Part 2. J. Bodyw. Mov. Ther. 2003, 7, 104–116. [Google Scholar] [CrossRef]
- Weinberg, R.S.; Hunt, V.V. Effects of Structural Integration on State-Trait Anxiety. J. Clin. Psychol. 1979, 35, 319–322. [Google Scholar] [CrossRef]
- Jones, T.A. Rolfing. Phys. Med. Rehabil. Clin. N. Am. 2004, 15, 799–809. [Google Scholar] [CrossRef]
- James, H.; Castaneda, L.; Miller, M.E.; Findley, T. Rolfing Structural Integration Treatment of Cervical Spine Dysfunction. J. Bodyw. Mov. Ther. 2009, 13, 229–238. [Google Scholar] [CrossRef]
- Evans, E.M.; Rowe, D.A.; Racette, S.B.; Ross, K.M.; McAuley, E. Is the Current BMI Obesity Classification Appropriate for Black and White Postmenopausal Women? Int. J. Obes. 2006, 30, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry; FA Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Fleiss, J.L. Reliability of Measurement. In Design and Analysis of Clinical Experiments; John Wiley & Sons: Hoboken, NJ, USA, 2011; pp. 1–32. [Google Scholar]
- Mullaney, M.J.; McHugh, M.P.; Johnson, C.P.; Tyler, T.F. Reliability of Shoulder Range of Motion Comparing a Goniometer to a Digital Level. Physiother. Theory Pract. 2010, 26, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Adegoke, B.O.; Fapojuwo, O.A. Range of Active Hip Motion in Low Back Pain Patients and Apparently Healthy Controls. J. Allied Health Sci. Pract. 2010, 8, 11. [Google Scholar] [CrossRef]
- Frost, M.; Stuckey, S.; Smalley, L.A.; Dorman, G. Reliability of Measuring Trunk Motions in Centimeters. Phys Ther 1982, 62, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 1st ed.; Academic Press: New York, NY, USA, 1988; ISBN 978-0-12-179060-8. [Google Scholar]
- Taş, S.; Salkın, Y. An Investigation of the Sex-Related Differences in the Stiffness of the Achilles Tendon and Gastrocnemius Muscle: Inter-Observer Reliability and Inter-Day Repeatability and the Effect of Ankle Joint Motion. Foot 2019, 41, 44–50. [Google Scholar] [CrossRef]
- Bohlen, L.; Schwarze, J.; Richter, J.; Gietl, B.; Lazarov, C.; Kopyakova, A.; Brandl, A.; Schmidt, T. Immediate Effect of Osteopathic Techniques on Human Resting Muscle Tone in Healthy Subjects Using Myotonometry: A Factorial Randomized Trial. medRxiv 2022. [Google Scholar] [CrossRef]
- Ilahi, S.; Masi, A.; White, A.; Devos, A.; Henderson, J.; Nair, K. Quantified Biomechanical Properties of Lower Lumbar Myofascia in Younger Adults with Chronic Idiopathic Low Back Pain and Matched Healthy Controls. Clin. Biomech. 2020, 73, 78–85. [Google Scholar] [CrossRef]
- Durand, S.; Rohan, C.P.-Y.; Hamilton, T.; Skalli, W.; Krebs, H.I. Passive Wrist Stiffness: The Influence of Handedness. IEEE Trans. Biomed. Eng. 2019, 66, 656–665. [Google Scholar] [CrossRef] [Green Version]
- Papadatou-Pastou, M.; Ntolka, E.; Schmitz, J.; Martin, M.; Munafò, M.R.; Ocklenburg, S.; Paracchini, S. Human Handedness: A Meta-Analysis. Psychol. Bull. 2020, 146, 481. [Google Scholar] [CrossRef]
- Willard, F.H.; Vleeming, A.; Schuenke, M.D.; Danneels, L.; Schleip, R. The Thoracolumbar Fascia: Anatomy, Function and Clinical Considerations. J. Anat. 2012, 221, 507–536. [Google Scholar] [CrossRef]
- Schuenke, M.D.; Vleeming, A.; Van Hoof, T.; Willard, F.H. A Description of the Lumbar Interfascial Triangle and Its Relation with the Lateral Raphe: Anatomical Constituents of Load Transfer through the Lateral Margin of the Thoracolumbar Fascia. J. Anat. 2012, 221, 568–576. [Google Scholar] [CrossRef]
- Vleeming, A.; Schuenke, M.D.; Danneels, L.; Willard, F.H. The Functional Coupling of the Deep Abdominal and Paraspinal Muscles: The Effects of Simulated Paraspinal Muscle Contraction on Force Transfer to the Middle and Posterior Layer of the Thoracolumbar Fascia. J. Anat. 2014, 225, 447–462. [Google Scholar] [CrossRef] [PubMed]
- Brandl, A.; Egner, C.; Schleip, R. Practical Measurement of Changes in Leg Length Discrepancy After a Myofascial Release on the Thoracolumbar Fascia in Patients With Acute Low Back Pain: A Pilot Study. Cureus 2022, 14, 29084. [Google Scholar] [CrossRef]
- Camargo, P.R.; Neumann, D.A. Kinesiologic Considerations for Targeting Activation of Scapulothoracic Muscles—Part 2: Trapezius. Braz. J. Phys. Ther. 2019, 23, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Krause, F.; Wilke, J.; Vogt, L.; Banzer, W. Intermuscular Force Transmission along Myofascial Chains: A Systematic Review. J. Anat. 2016, 228, 910–918. [Google Scholar] [CrossRef]
- Findley, T.W.; Schleip, R. Basic Science and Implications for Conventional and Complementary Health Care; Elsevier Urban and Fischer: Munich, Germany, 2007. [Google Scholar]
- Andrade, R.J.; Freitas, S.R.; Hug, F.; Le Sant, G.; Lacourpaille, L.; Gross, R.; McNair, P.; Nordez, A. The Potential Role of Sciatic Nerve Stiffness in the Limitation of Maximal Ankle Range of Motion. Sci. Rep. 2018, 8, 14532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stecco, A.; Gesi, M.; Stecco, C.; Stern, R. Fascial Components of the Myofascial Pain Syndrome. Curr. Pain Headache Rep. 2013, 17, 352. [Google Scholar] [CrossRef]
- Chen, Y.-L.; Lin, W.-C.; Liao, Y.-H.; Chen, Y.; Kang, P.-Y. Changing the Pattern of the Back-Muscle Flexion–Relaxation Phenomenon through Flexibility Training in Relatively Inflexible Young Men. PLoS ONE 2021, 16, e0259619. [Google Scholar] [CrossRef]
- Wilke, J.; Macchi, V.; De Caro, R.; Stecco, C. Fascia Thickness, Aging and Flexibility: Is There an Association? J. Anat. 2019, 234, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.; Kongsgaard, M.; Holm, L.; Skovgaard, D.; Magnusson, S.P.; Qvortrup, K.; Larsen, J.O.; Aagaard, P.; Dahl, M.; Serup, A.; et al. Effect of Estrogen on Tendon Collagen Synthesis, Tendon Structural Characteristics, and Biomechanical Properties in Postmenopausal Women. J. Appl. Physiol. 2009, 106, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.V.; Barton, F.B.; Terhorst, L.; Shembel, A. Retrospective Studies: A Fresh Look. Am. J. Speech Lang. Pathol. 2016, 25, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Tarsha, M.S.; Park, S.; Tortora, S. Body-Centered Interventions for Psychopathological Conditions: A Review. Front. Psychol. 2020, 10, 2907. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Session | Intervention |
|---|---|
| 1 | The focus of this session is breathing. Myofascial release is applied to the muscles of the trunk, ribs, shoulder, neck, and head. They also mobilize the hip and legs to align the pelvis horizontally. The assessment and treatment of specific problems is addressed throughout every session. |
| 2 | The focus of this session is posture. They balance the feet, lower legs, and knees to correct the spinal curvatures. |
| 3 | The focus of this session is spinal elongation. They work on the lateral aspect of the body to create elongation of the spine. |
| 4 | The focus of this session is stability of the legs. They work on the plantar arches and the medial aspect of the lower extremity. The spine is mobilized and continues to be elongated. |
| 5 | The focus of this session is to balance the trunk with the legs. They work on the abdominal, pelvic, and iliopsoas muscles. The outer abdominal wall is elongated and mobilized to create continuity with the inner tissues. |
| 6 | The focus of this session is to improve trunk mobility with stabilization of the pelvis and lower extremities. They work on the posterior pelvis, back, neck, and head. |
| 7 | The focus of this session is to balance the rhythm of cranial movements. Work is done in the upper back, shoulders, neck, cranium, and facial structures. |
| 8 | The focus of this session is lower body integration. Work is done to the pelvic girdle and extremities. Specific problems become a priority in the treatment. |
| 9 | The focus of this session is upper body integration. Work is done to the pelvic girdle and extremities. Specific problems become a priority in the treatment. |
| 10 | The focus of this session is to correct the level of the structures bilaterally during static and dynamic activities. Specific problems become a priority in the treatment. Specific problems are assessed and treated throughout the 10 sessions. |
| Baseline Characteristics | Participants (n = 383) Mean ± SD |
|---|---|
| Gender (men/woman) | 154/228 |
| Disease (A/B/C/D/E) | 101/114/42/27/99 |
| Age (years) | 39.0 ± 11.1 |
| Age group (younger/older) | 189/194 |
| Height (m) | 1.70 ± 0.1 |
| Weight (kg) | 71.3 ± 16.1 |
| BMI (kg/m2) | 25.2 ± 5.7 |
| All Subjects (n = 383) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Shoulder (n = 242) | Hip (n = 141) | Functional Tests (n = 141) | |||||||||
| Flexion L | Flexion R | External Rotation L | External Rotation R | Internal Rotation L | Internal Rotation R | Flexion L | Flexion R | Side Bend L | Side Bend R | Finger to Floor | |
| ∆Mean | 7.81° | 7.16° | 4.26° | 4.52° | 18.00° | 17.33° | 8.30° | 8.26° | 0.42 cm | 0.68 cm | −2.21 cm |
| SD | 12.87 | 10.83 | 9.06 | 10.61 | 13.13 | 10.87 | 8.84 | 8.70 | 1.61 | 1.77 | 6.73 |
| 95%-CI | 5.17–10.6 | 4.62–9.70 | 2.61–5.92 | 2.22–6.22 | 15.5–20.5 | 14.9–19.8 | 6.12–10.8 | 6.14–10.9 | −0.33–1.17 | −0.07–1.42 | −4.51–0.09 |
| % t1–t0 | +5% | +4% | +5% | +5% | +37% | +38% | +7% | +7% | +1% | +2% | −25% |
| ANOVA 1 | |||||||||||
| DFn, DFd | 1418 | 1416 | 1386 | 1386 | 1440 | 1440 | 1238 | 1242 | 1242 | 1244 | 1230 |
| F | 70.80 | 57.26 | 70.80 | 32.81 | 207.7 | 189.3 | 56.41 | 57.48 | 1.56 | 3.75 | 3.02 |
| part. η² | 0.15 | 0.12 | 0.08 | 0.08 | 0.32 | 0.30 | 0.19 | 0.19 | 0.006 | 0.015 | 0.013 |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | 0.213 | 0.054 | 0.084 |
| Female (n = 228) | |||||||||||
| Shoulder (n = 147) | Hip (n = 81) | Functional tests (n = 81) | |||||||||
| Flexion L | Flexion R | External rotation L | External rotation R | Internal rotation L | Internal rotation R | Flexion L | Flexion R | Side bend L | Side bend R | Finger to floor | |
| ∆Mean | 5.48° | 6.19° | 2.46° | 3.45° | 16.97° | 16.64° | 8.70° | 8.21° | 0.43 cm | 0.67 cm | −1.93 cm |
| SD | 14.34 | 11.29 | 7.34 | 10.59 | 13.69 | 10.46 | 8.76 | 8.11 | 1.60 | 1.79 | 6.82 |
| 95%-CI | 1.04–9.91 | 1.92–10.5 | −0.34–5.25 | 0.62–6.32 | 12.8–21.1 | 12.5–20.8 | 4.94–12.5 | 4.54–11.9 | −0.84–1.69 | −0.61–1.95 | −5.91–2.06 |
| p (adjusted) 2 | 0.008 | 0.158 | 0.112 | ||||||||
| Male (n = 154) | |||||||||||
| Shoulder (n = 95) | Hip (n = 59) | Functional tests (n = 59) | |||||||||
| Flexion L | Flexion R | External rotation L | External rotation R | Internal rotation L | Internal rotation R | Flexion L | Flexion R | Side bend L | Side bend R | Finger to floor | |
| ∆Mean | 11.42° | 8.65° | 7.06° | 6.16° | 19.58° | 18.40° | 7.75° | 8.33° | 0.42 cm | 0.69 cm | −2.59 cm |
| SD | 9.16 | 9.94 | 10.66 | 11.31 | 12.13 | 11.46 | 8.99 | 9.51 | 1.64 | 1.77 | 6.65 |
| 95%-CI | 5.90–16.94 | 3.33–14.0 | 3.59–10.5 | 2.61–9.70 | 14.4–24.7 | 13.3–23.6 | 3.38–12.1 | 4.07–12.6 | −1.05–1.89 | −0.82–2.19 | −7.22–2.04 |
| % m–f | +108% | +40% | +187% | +79% | +15% | +11% | −11% | +1% | −2% | +3% | +34% |
| p (adjusted) 2 | <0.0001 | <0.0001 | <0.0001 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brandl, A.; Bartsch, K.; James, H.; Miller, M.E.; Schleip, R. Influence of Rolfing Structural Integration on Active Range of Motion: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 5878. https://doi.org/10.3390/jcm11195878
Brandl A, Bartsch K, James H, Miller ME, Schleip R. Influence of Rolfing Structural Integration on Active Range of Motion: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(19):5878. https://doi.org/10.3390/jcm11195878
Chicago/Turabian StyleBrandl, Andreas, Katja Bartsch, Helen James, Marilyn E. Miller, and Robert Schleip. 2022. "Influence of Rolfing Structural Integration on Active Range of Motion: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 19: 5878. https://doi.org/10.3390/jcm11195878