
Midazolam versus Dexmedetomidine in Patients at Risk of Obstructive Sleep Apnea during Urology Procedures: A Randomized Controlled Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
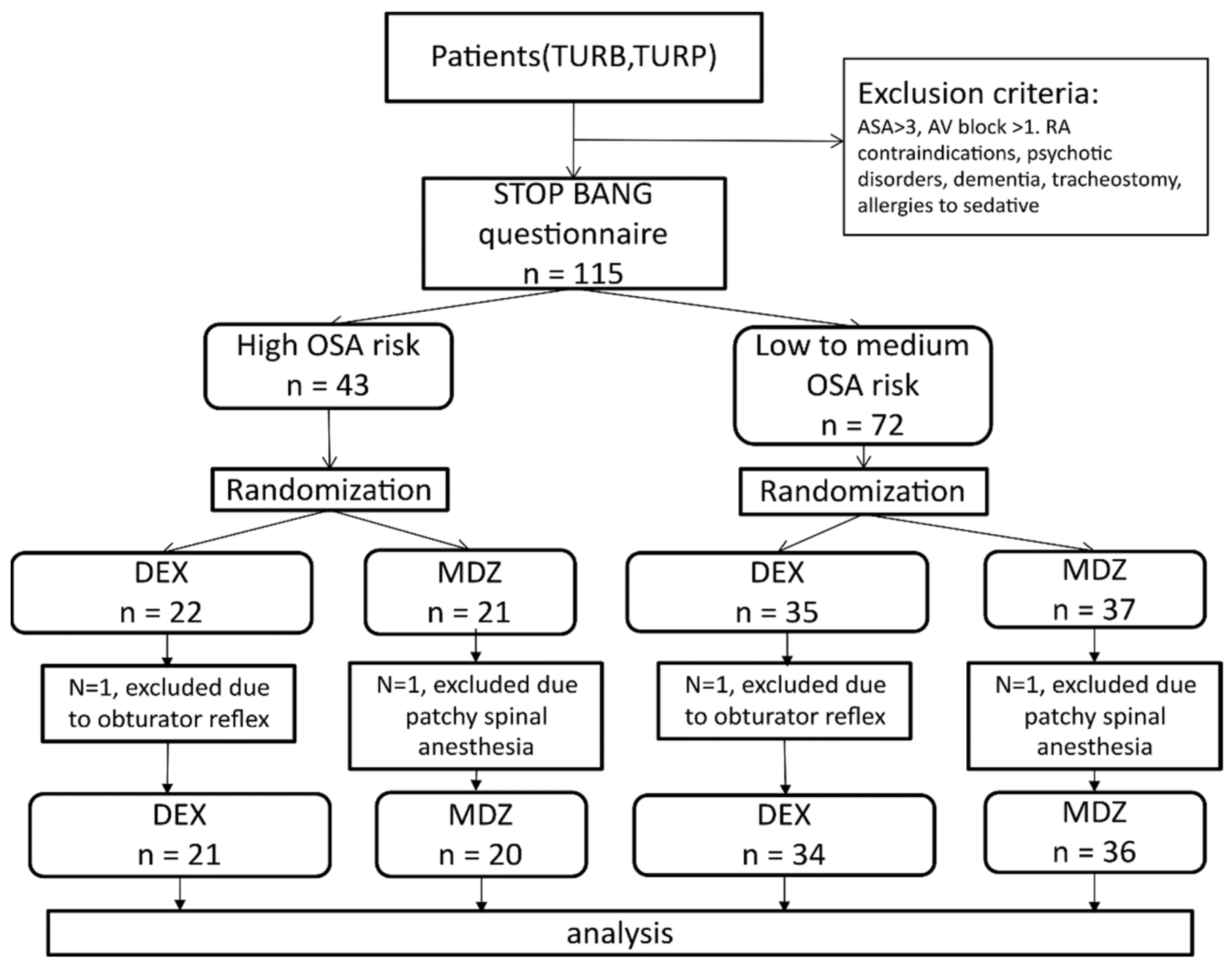
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Effects of OSA Risk on Primary Outcomes
3.2. Effects of Hypnotic on Primary Outcomes
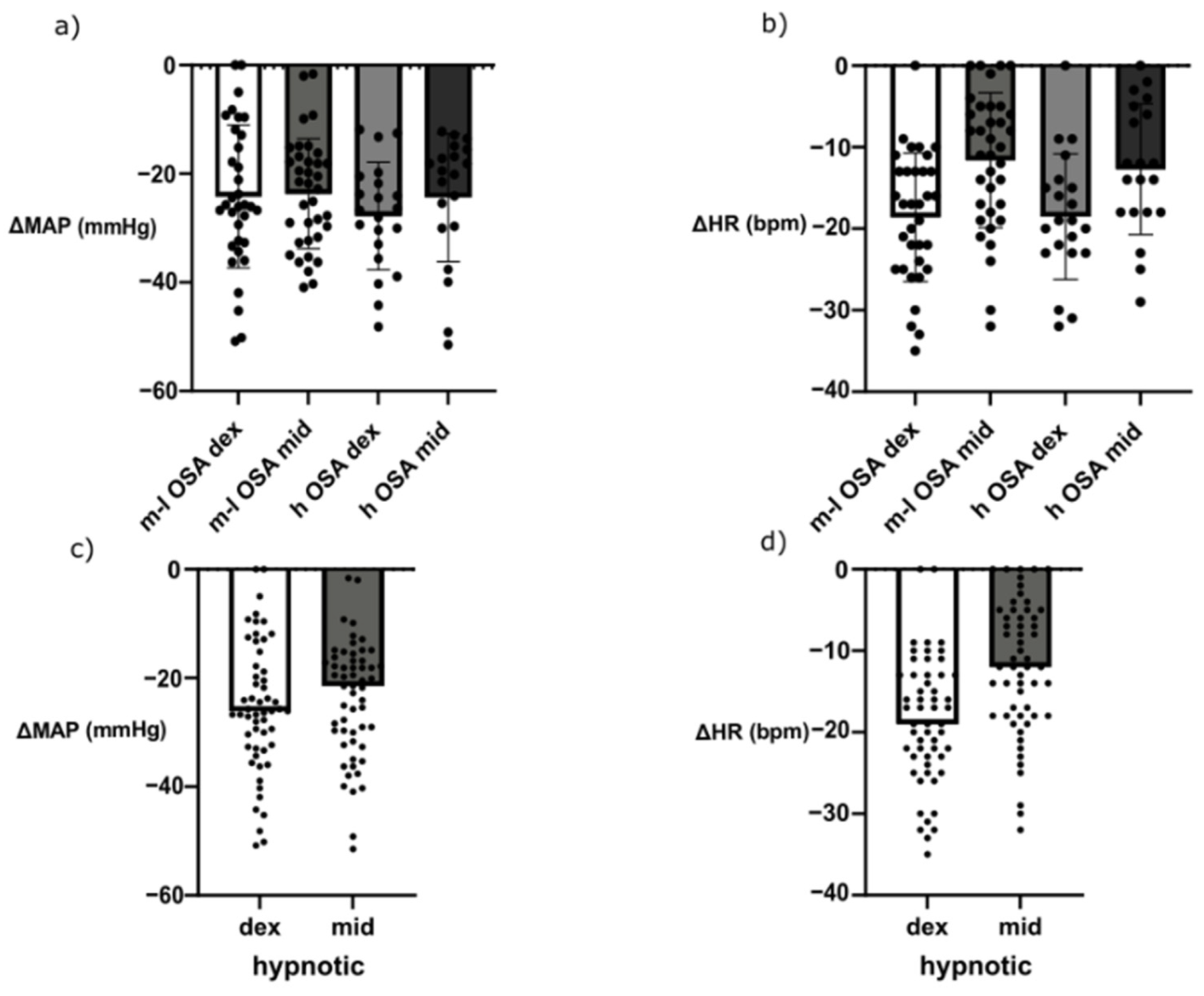
3.3. Effects of Hypnotics on Hemodynamics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roesslein, M.; Chung, F. Obstructive sleep apnoea in adults: Peri-operative considerations: A narrative review. Eur. J. Anaesthesiol. 2018, 35, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Madhusudan, P.; Wong, J.; Prasad, A.; Sadeghian, E.; Chung, F.F. An update on preoperative assessment and preparation of surgical patients with obstructive sleep apnea. Curr. Opin. Anaesthesiol. 2018, 31, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.K.; Sharma, A. Atrial fibrillation in obstructive sleep apnea. World J. Cardiol. 2013, 5, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Corso, R.; Russotto, V.; Gregoretti, C.; Cattano, D. Perioperative management of obstructive sleep apnea: A systematic review. Minerva Anestesiol. 2018, 84, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.T.; Lee, Z.X.; Ang, E.; Teoh, W.Y.; Wang, C.Y. Association of obstructive sleep apnea and postoperative cardiac complications: A systematic review and meta-analysis with trial sequential analysis. J. Clin. Anesth. 2020, 62, 109731. [Google Scholar] [CrossRef]
- Pivetta, B.; Sun, Y.; Nagappa, M.; Chan, M.; Englesakis, M.; Chung, F. Postoperative outcomes in surgical patients with obstructive sleep apnoea diagnosed by sleep studies: A meta-analysis and trial sequential analysis. Anaesthesia 2022, 77, 818–828. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP Questionnaire. A Tool to Screen Patients for Obstructive Sleep Apnea. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Li, S.; Zhao, Y.; Zhao, X.; Zhou, Z.; Hao, Q.; Luo, A.; Sun, R. Preoperative screening of patients at high risk of obstructive sleep apnea and postoperative complications: A systematic review and meta-analysis. J. Clin. Anesth. 2022, 79, 110692. [Google Scholar] [CrossRef]
- Seet, E.; Chua, M.; Liaw, C.M. High STOP-BANG questionnaire scores predict intraoperative and early postoperative adverse events. Singap. Med. J. 2015, 56, 212–216. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharyya, S.; Bisai, S.; Biswas, H.; Tiwary, M.K.; Mallik, S.; Saha, S.M. Regional anesthesia in transurethral resection of prostate (TURP) surgery: A comparative study between saddle block and subarachnoid block. Saudi J. Anaesth. 2015, 9, 268–271. [Google Scholar] [CrossRef]
- Memtsoudis, S.G.; Cozowicz, C.; Nagappa, M.; Wong, J.; Joshi, G.P.; Wong, D.T.; Doufas, A.G.; Yilmaz, M.; Stein, M.H.; Krajewski, M.L.; et al. Society of Anesthesia and Sleep Medicine Guideline on Intraoperative Management of Adult Patients With Obstructive Sleep Apnea. Anesth. Analg. 2018, 127, 967–987. [Google Scholar] [CrossRef] [PubMed]
- Pollock, J.E.; Neal, J.M.; Liu, S.S.; Burkhead, D.; Polissar, N. Sedation during spinal anesthesia. Anesthesiology 2000, 93, 728–734. [Google Scholar] [CrossRef] [PubMed]
- De Andrés, J.; Valía, J.C.; Gil, A.; Bolinches, R. Predictors of patient satisfaction with regional anesthesia. Reg. Anesth. 1995, 20, 498–505. [Google Scholar] [PubMed]
- Becker, D.E.; Haas, D.A. Management of complications during moderate and deep sedation: Respiratory and cardiovascular considerations. Anesth. Prog. 2007, 54, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.D. Miller’s Anesthesia; Elsevier Saunders: Philadelphia, PA, USA, 2009. [Google Scholar]
- Hall, J.E.; Uhrich, T.D.; Barney, J.A.; Arain, S.R.; Ebert, T.J. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth. Analg. 2000, 90, 699–705. [Google Scholar] [CrossRef]
- Hsu, Y.W.; Cortinez, L.I.; Robertson, K.M.; Keifer, J.C.; Sum-Ping, S.T.; Moretti, E.W.; Young, C.C.; Wright, D.R.; Macleod, D.B.; Somma, J. Dexmedetomidine pharmacodynamics: Part I: Crossover comparison of the respiratory effects of dexmedetomidine and remifentanil in healthy volunteers. Anesthesiology 2004, 101, 1066–1076. [Google Scholar] [CrossRef]
- Silva, J.M., Jr.; Katayama, H.T.; Nogueira, F.A.M.; Moura, T.B.; Alves, T.L.; de Oliveira, B.W. Comparison of dexmedetomidine and benzodiazepine for intraoperative sedation in elderly patients: A randomized clinical trial. Reg. Anesth. Pain Med. 2019, 44, 319–324. [Google Scholar] [CrossRef]
- Jo, Y.Y.; Lee, D.; Jung, W.S.; Cho, N.R.; Kwak, H.J. Comparison of Intravenous Dexmedetomidine and Midazolam for Bispectral Index-Guided Sedation During Spinal Anesthesia. Med. Sci. Monit. 2016, 22, 3544–3551. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.M.; Choi, E.J.; Ri, H.S.; Park, J.Y.; You, J.A.; Byeon, G.J. The effect of dexmedetomidine and midazolam on combined spinal-epidural anesthesia in patients undergoing total knee arthroplasty. Anesth. Pain Med. 2020, 15, 111–119. [Google Scholar] [CrossRef]
- Kress, J.P.; Hall, J.B. Sedation in the mechanically ventilated patient. Crit. Care Med. 2006, 34, 2541–2546. [Google Scholar] [CrossRef]
- Shin, H.J.; Kim, E.Y.; Hwang, J.W.; Do, S.H.; Na, H.S. Comparison of upper airway patency in patients with mild obstructive sleep apnea during dexmedetomidine or propofol sedation: A prospective, randomized, controlled trial. BMC Anesthesiol. 2018, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Höhener, D.; Blumenthal, S.; Borgeat, A. Sedation and regional anaesthesia in the adult patient. Br. J. Anaesth. 2008, 100, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, P.J.; Dubey, K.P.; Sahare, K.K.; Agrawal, A. Intravenous dexmedetomidine versus propofol for intraoperative moderate sedation during spinal anesthesia: A comparative study. J. Anaesthesiol. Clin. Pharmacol. 2016, 32, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Lodenius, Å.; Maddison, K.J.; Lawther, B.K.; Scheinin, M.; Eriksson, L.I.; Eastwood, P.R.; Hillman, D.R.; Fagerlund, M.J.; Walsh, J.H. Upper Airway Collapsibility during Dexmedetomidine and Propofol Sedation in Healthy Volunteers: A Nonblinded Randomized Crossover Study. Anesthesiology 2019, 131, 962–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capasso, R.; Rosa, T.; Tsou, D.Y.-A.; Nekhendzy, V.; Drover, D.; Collins, J.; Zaghi, S.; Camacho, M. Variable Findings for Drug-Induced Sleep Endoscopy in Obstructive Sleep Apnea with Propofol versus Dexmedetomidine. Otolaryngol. Head Neck Surg. 2016, 154, 765–770. [Google Scholar] [CrossRef]
- Yoon, B.W.; Hong, J.M.; Hong, S.L.; Koo, S.K.; Roh, H.J.; Cho, K.S. A comparison of dexmedetomidine versus propofol during drug-induced sleep endoscopy in sleep apnea patients. Laryngoscope 2016, 126, 763–767. [Google Scholar] [CrossRef]
- Ma, X.X.; Fang, X.M.; Hou, T.N. Comparison of the effectiveness of dexmedetomidine versus propofol target-controlled infusion for sedation during coblation-assisted upper airway procedure. Chin. Med. J. 2012, 125, 869–873. [Google Scholar]
- Chen, Y.-T.; Sun, C.-K.; Wu, K.-Y.; Chang, Y.-J.; Chiang, M.-H.; Chen, I.-W.; Liao, S.-W.; Hung, K.-C. The Use of Propofol versus Dexmedetomidine for Patients Receiving Drug-Induced Sleep Endoscopy: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 1585. [Google Scholar] [CrossRef]
- Yun, M.; Kim, J.; Ryu, S.; Han, S.; Shin, Y. The correlation between the STOP-Bang score and oxygen saturation during spinal anesthesia with dexmedetomidine sedation. Anesth. Pain Med. 2021, 16, 305–311. [Google Scholar] [CrossRef]
- Weinbroum, A.A.; Szold, O.; Ogorek, D.; Flaishon, R. The midazolam-induced paradox phenomenon is reversible by flumazenil. Epidemiology, patient characteristics and review of the literature. Eur. J. Anaesthesiol. 2001, 18, 789–797. [Google Scholar] [CrossRef]
- Robin, C.; Trieger, N. Paradoxical reactions to benzodiazepines in intravenous sedation: A report of 2 cases and review of the literature. Anesth. Prog. 2002, 49, 128–132. [Google Scholar] [PubMed]
- Bloor, B.C.; Ward, D.S.; Belleville, J.P.; Maze, M. Effects of intravenous dexmedetomidine in humans. II. Hemodynamic changes. Anesthesiology 1992, 77, 1134–1142. [Google Scholar] [CrossRef] [PubMed]
- Riker, R.R.; Shehabi, Y.; Bokesch, P.M.; Ceraso, D.; Wisemandle, W.; Koura, F.; Whitten, P.; Margolis, B.D.; Byrne, D.W.; Ely, E.W.; et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: A randomized trial. JAMA 2009, 301, 489–499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OSA Risk | Low to Medium | High | p Value * | ||||||
|---|---|---|---|---|---|---|---|---|---|
| hypnotic | DEX | MDZ | DEX | MDZ | |||||
| age (years, median, IQR) | 65 | 61 to 68.25 | 69.5 | 61.25 to 69.5 | 68 | 63 to 68 | 69 | 67 to 71.75 | 0.1207 |
| sex (male, %) | 67.65 | 80.56 | 90.48 | 100 | 0.0169 | ||||
| BMI (kg/m2, median, IQR) | 25.75 a | 23.4 to 29.56 | 28.5 | 24.59 to 30.03 | 30.79 a | 27 to 33.93 | 28.72 | 27.44 to 33.29 | 0.0009 |
| neck circumference (cm, median, IQR) | 39 b | 36.5 to 44 | 41 c | 37.5 to 45 | 46 b | 42.5 to 48 | 45 c | 42.25 to 47 | <0.0001 |
| ASA score (median, IQR) | 2 d | 2 to 2 | 2 | 2 to 2 | 2 d | 2 to 3 | 2 | 2 to 2 | 0.0097 |
| duration of surgical procedure (min., median, IQR) | 50 | 30 to 70 | 50 | 30 to 70 | 40 | 30 to 70 | 60 | 40 to 70 | 0.3332 |
| time for eyes closing (min., median, IQR) | 10 e | 9 to 11.5 | 8 e | 7 to 9 | 9 | 7 to 11 | 9.5 | 8 to 10.75 | 0.0389 |
| baseline SpO2 (%, median, IQR) | 97 f | 96.75 to 99 | 98 g | 97 to 98 | 96 f,g | 95 to 97 | 97 | 96 to 99 | 0.0053 |
| STOP BANG (point, median, IQR) | 3 h | 2 to 3 | 3 i | 2 to 4 | 5 h,i | 5 to 6 | 5 h,i | 5 to 6 | <0.0001 |
| Outcome | OSA Low to Medium Risk | OSA High Risk | OR (OSA High) | 95% CI | OR (Dex) | 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DEX (Total n = 34) | MDZ (Total n = 36) | DEX (Total n = 21) | MDZ (Total n = 20) | Lower | Upper | Upper | Lower | |||||||
| n | % | n | % | n | % | n | % | |||||||
| desaturation | 2 | 5.88% | 9 | 25.00% | 5 | 23.81% | 16 | 80.00% | 8.981 | 3.257 | 28.4 | 0.112 | 0.032 | 0.323 |
| snoring | 10 | 29.41% | 23 | 63.89% | 17 | 80.95% | 20 | 100.00% | 14.26 | 4.67 | 55.58 | 0.195 | 0.072 | 0.491 |
| coughing | 4 | 11.76% | 14 | 38.89% | 4 | 19.05% | 10 | 50.00% | 1.62 | 0.66 | 3.98 | 0.225 | 0.084 | 0.548 |
| restlessness | 0 | 0.00% | 9 | 25.00% | 1 | 4.76% | 6 | 30.00% | 1.56 | 0.48 | 5.01 | 0.049 | 0.002 | 0.261 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vuković, I.; Duplančić, B.; Benzon, B.; Đogaš, Z.; Kovač, R.; Pecotić, R. Midazolam versus Dexmedetomidine in Patients at Risk of Obstructive Sleep Apnea during Urology Procedures: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 5849. https://doi.org/10.3390/jcm11195849
Vuković I, Duplančić B, Benzon B, Đogaš Z, Kovač R, Pecotić R. Midazolam versus Dexmedetomidine in Patients at Risk of Obstructive Sleep Apnea during Urology Procedures: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(19):5849. https://doi.org/10.3390/jcm11195849
Chicago/Turabian StyleVuković, Ivan, Božidar Duplančić, Benjamin Benzon, Zoran Đogaš, Ruben Kovač, and Renata Pecotić. 2022. "Midazolam versus Dexmedetomidine in Patients at Risk of Obstructive Sleep Apnea during Urology Procedures: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 19: 5849. https://doi.org/10.3390/jcm11195849