
Risk–Benefit Balance of Renin–Angiotensin–Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia


Abstract
:1. Introduction
2. Methods
2.1. Data Source
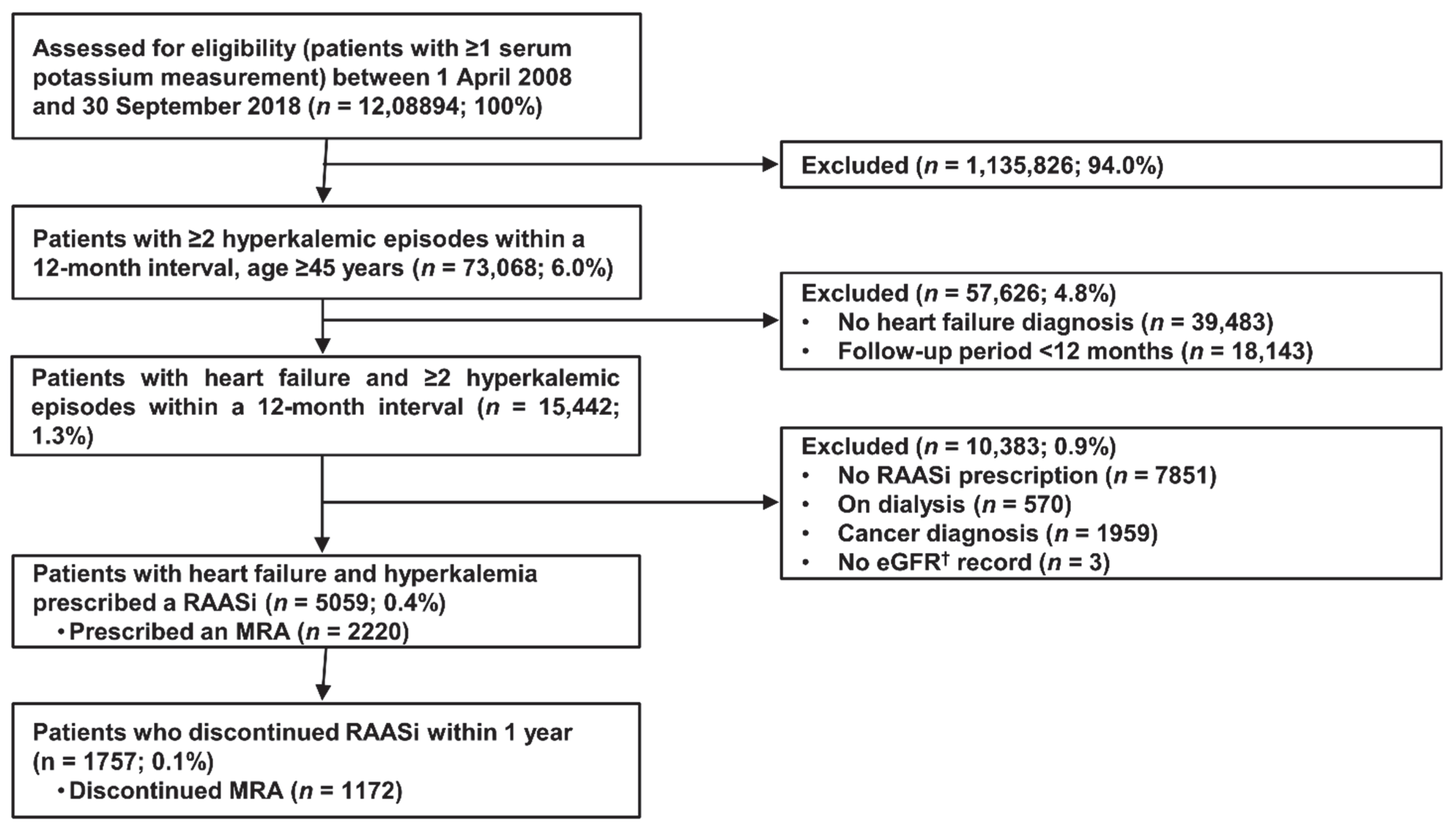
2.2. Study Design and Patient Selection
2.3. Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patients and Baseline Characteristics
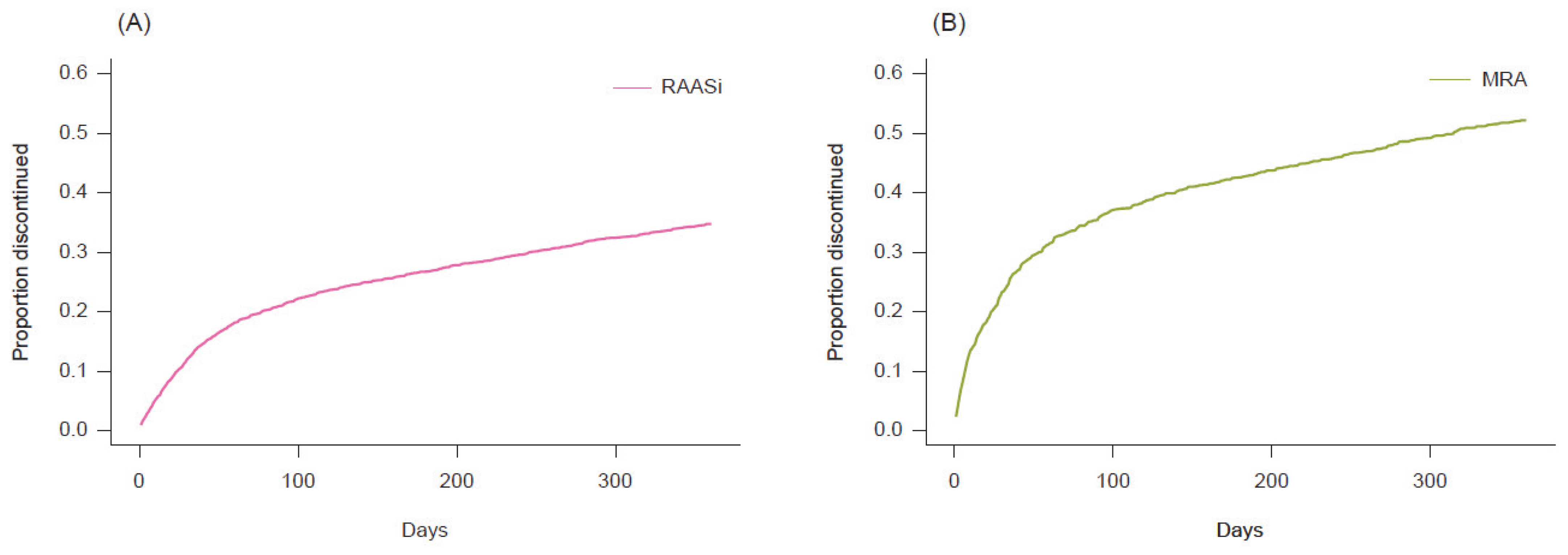
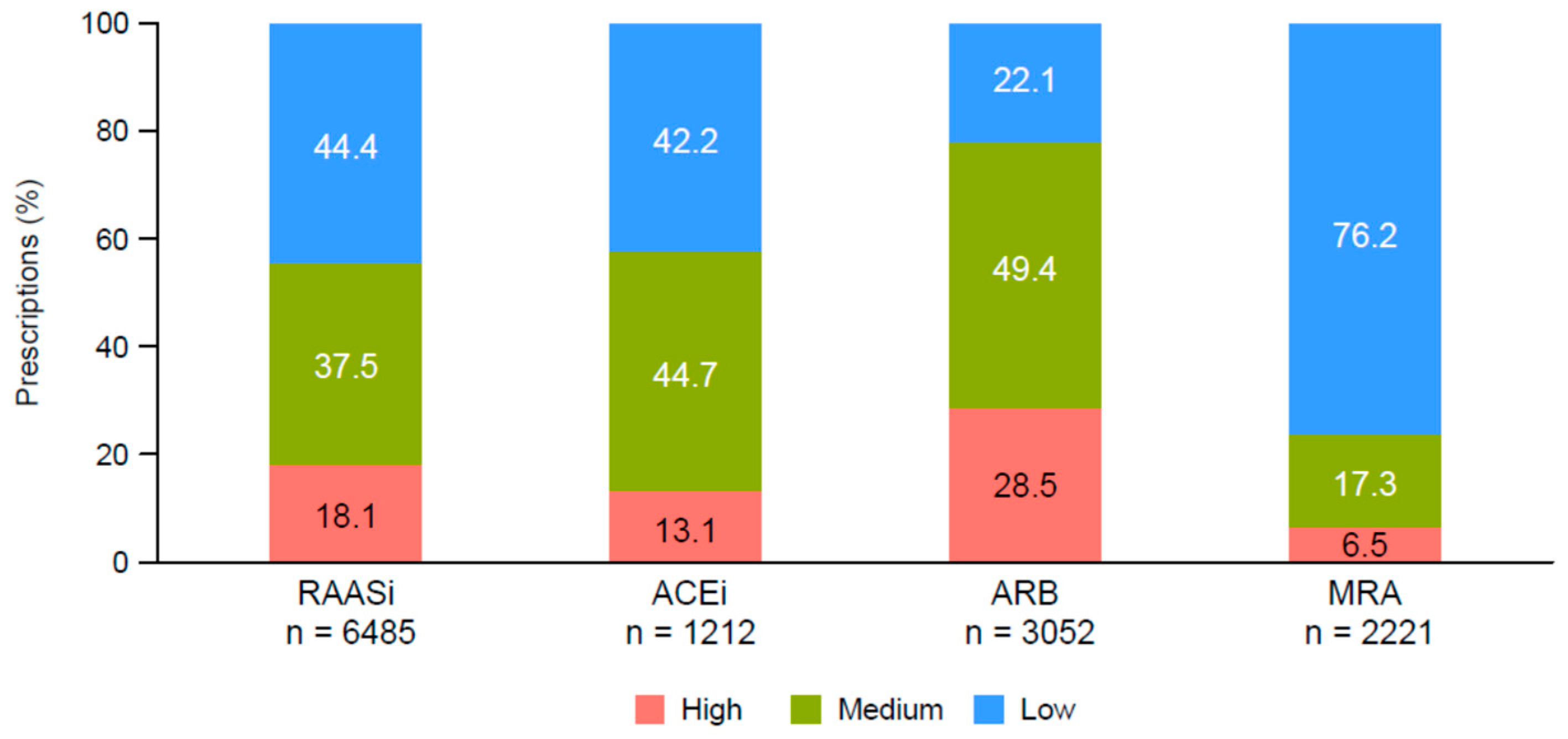
3.2. RAASi Treatment Patterns, Dose Reduction, and Cessation
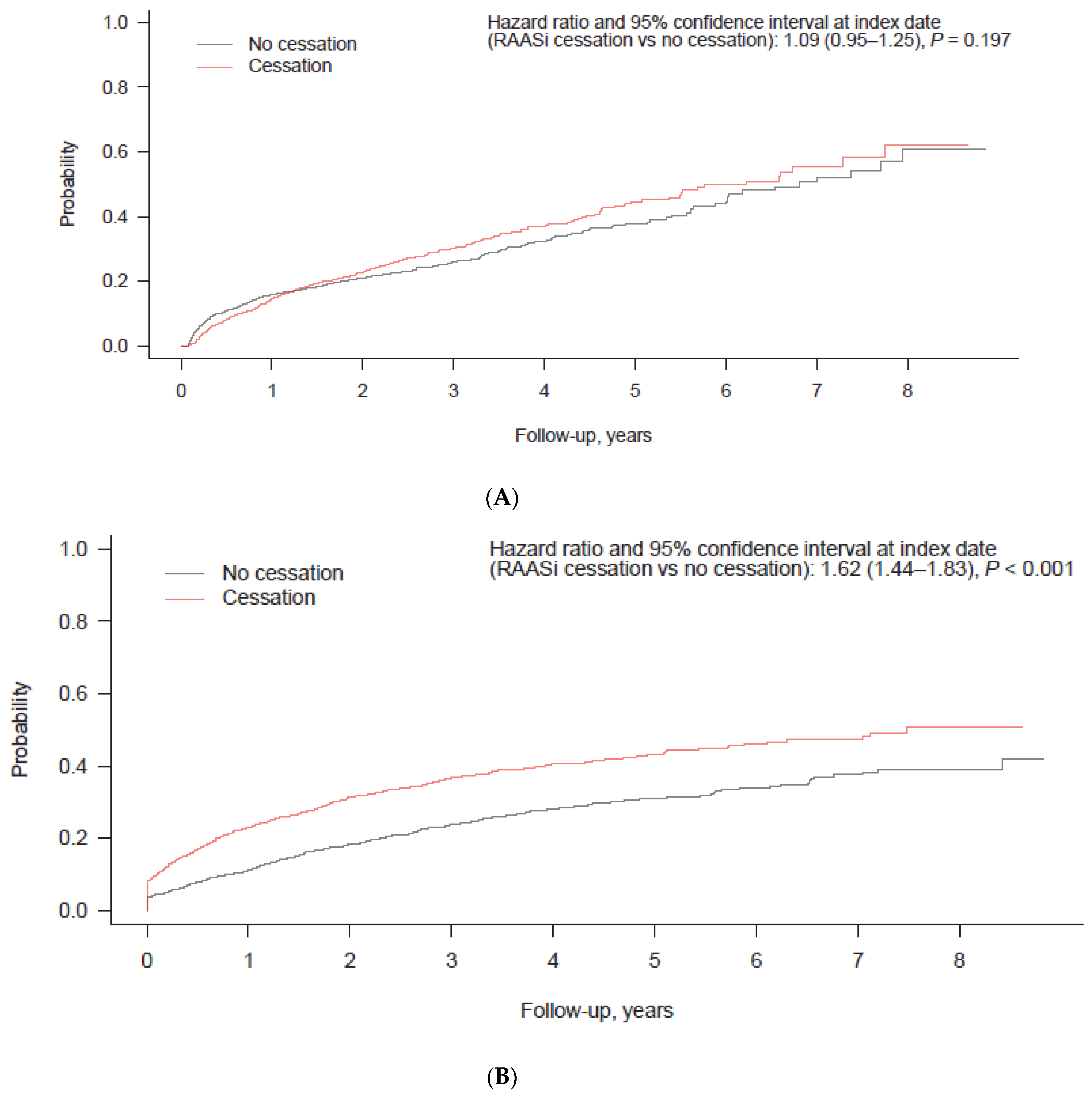
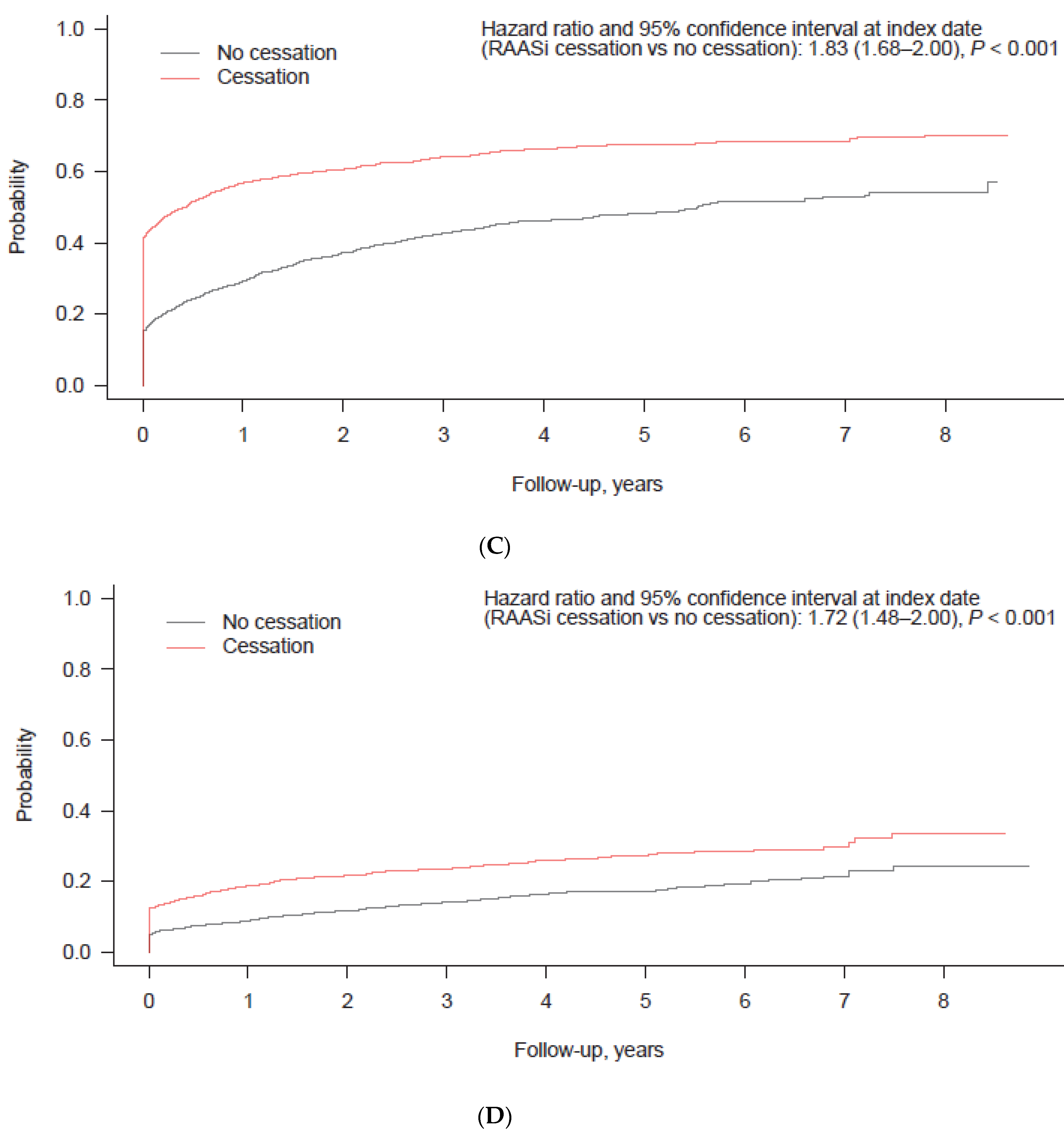
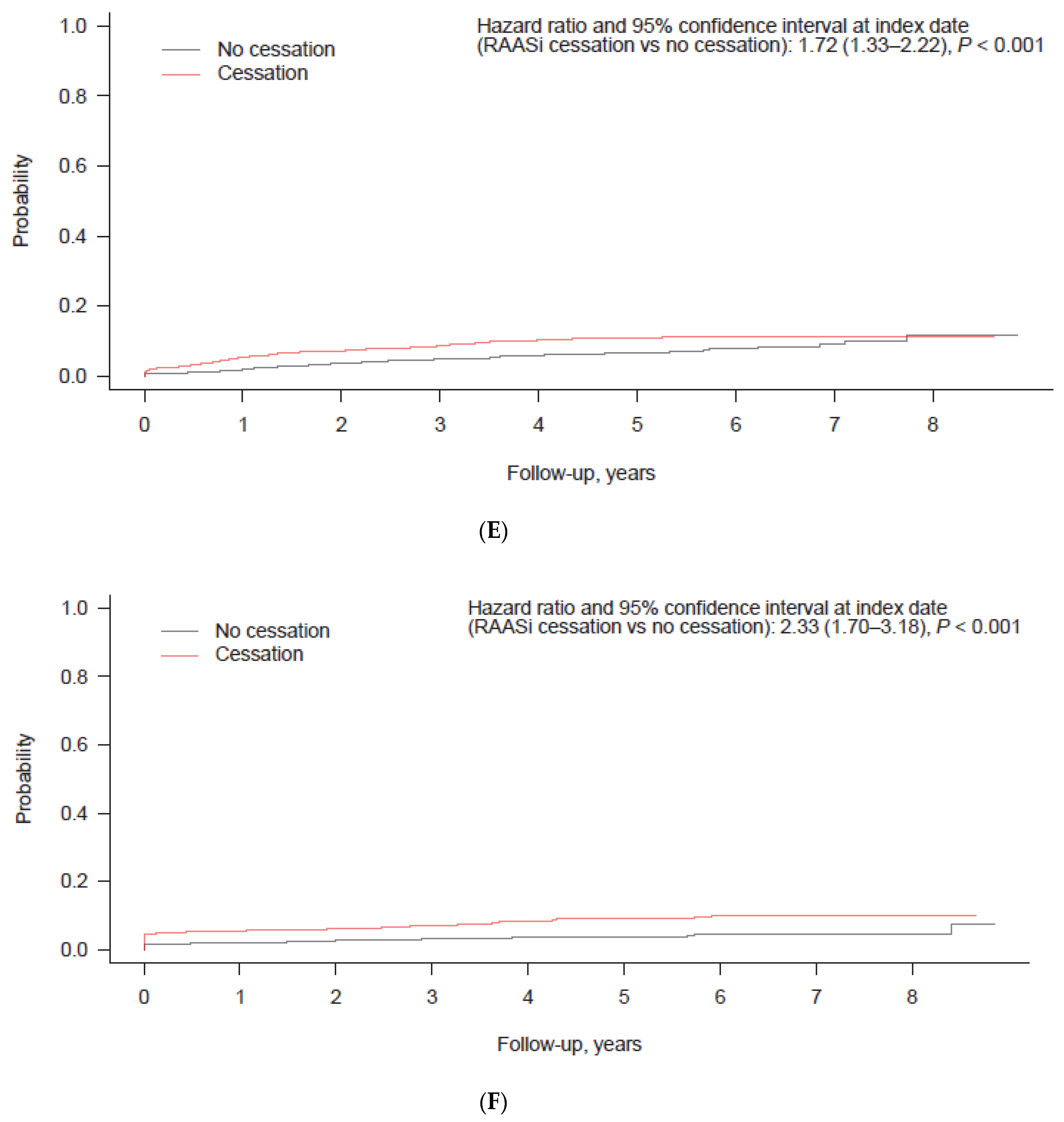
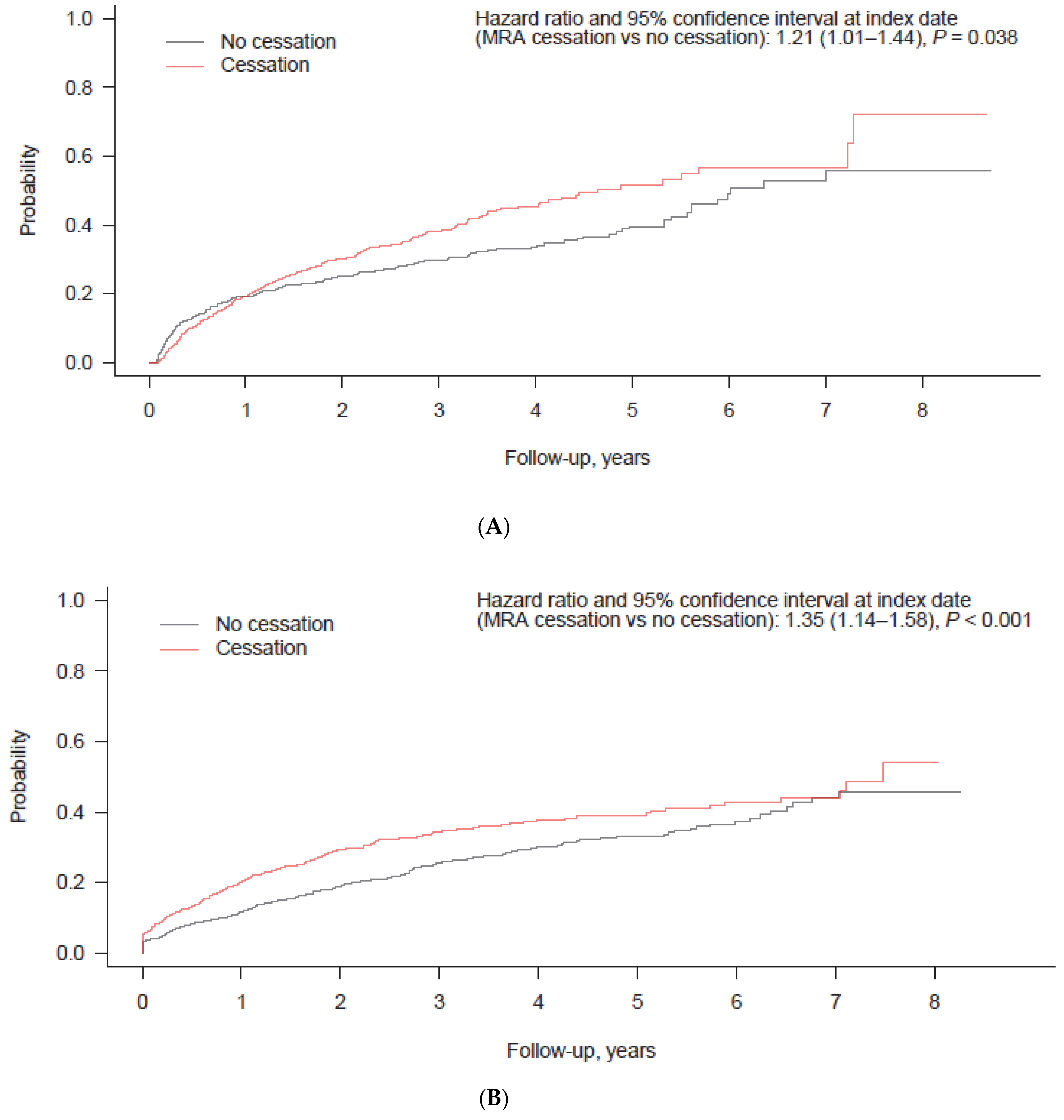
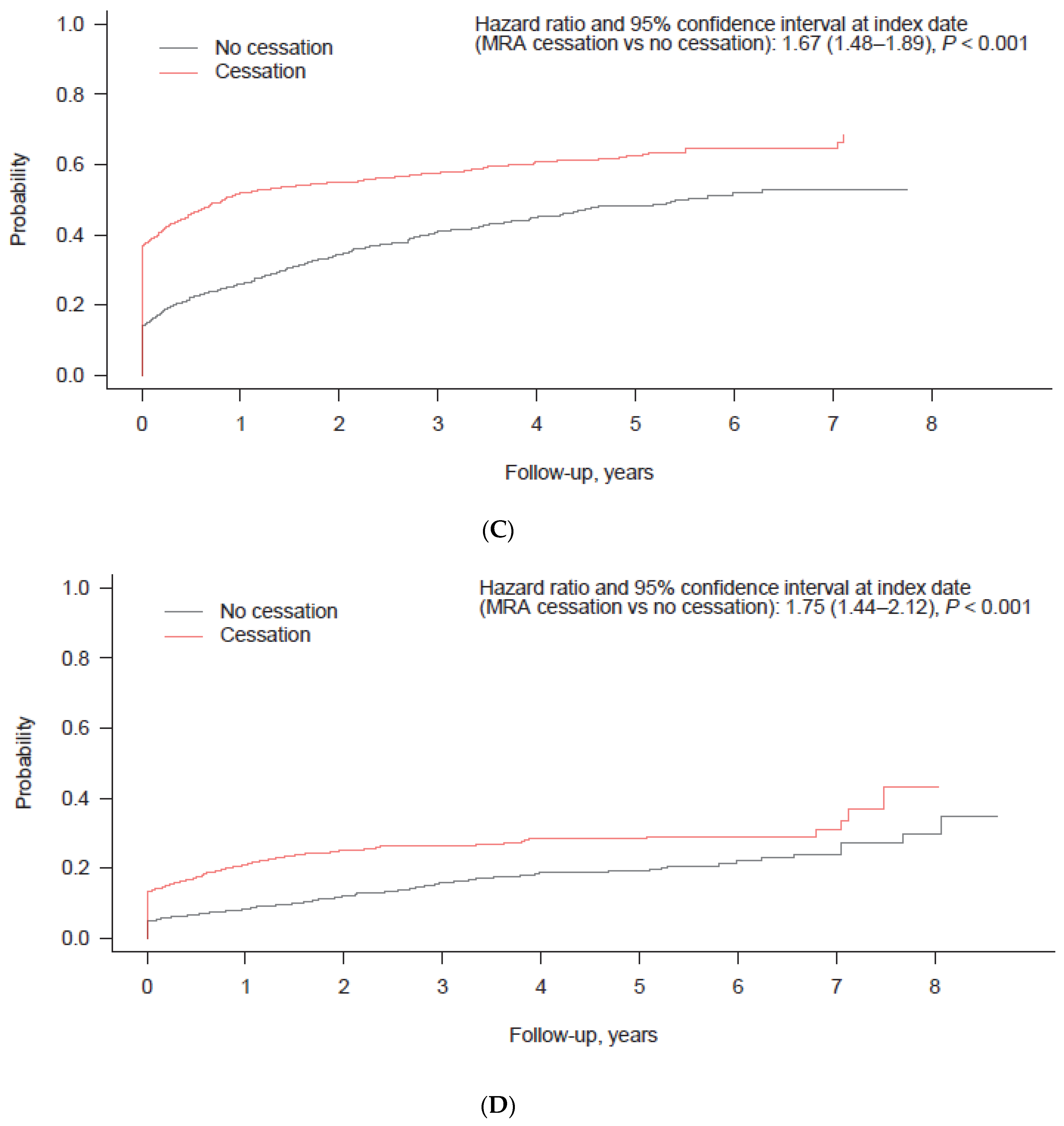
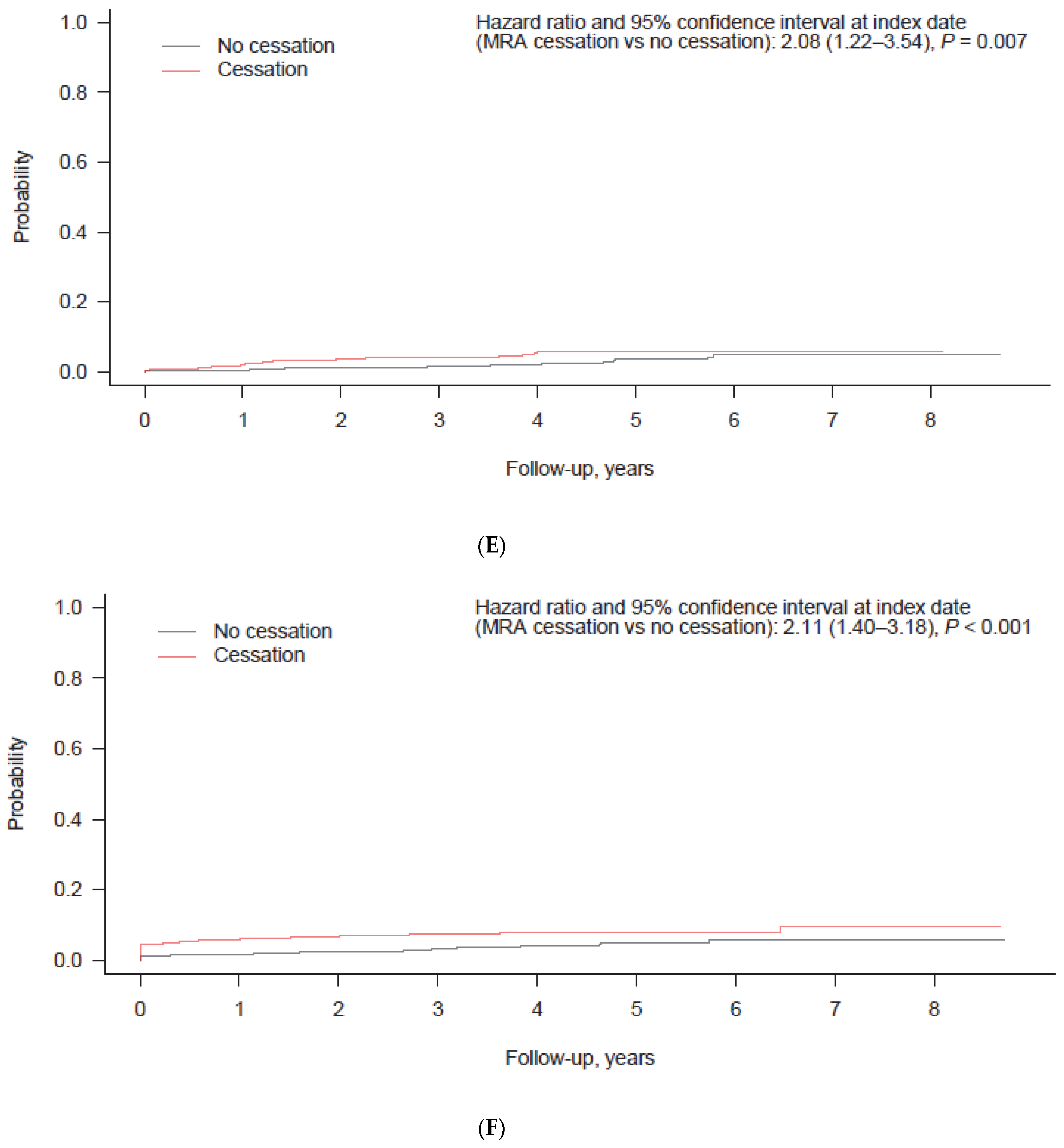
3.3. Impact of RAASi Cessation on Clinical Outcomes
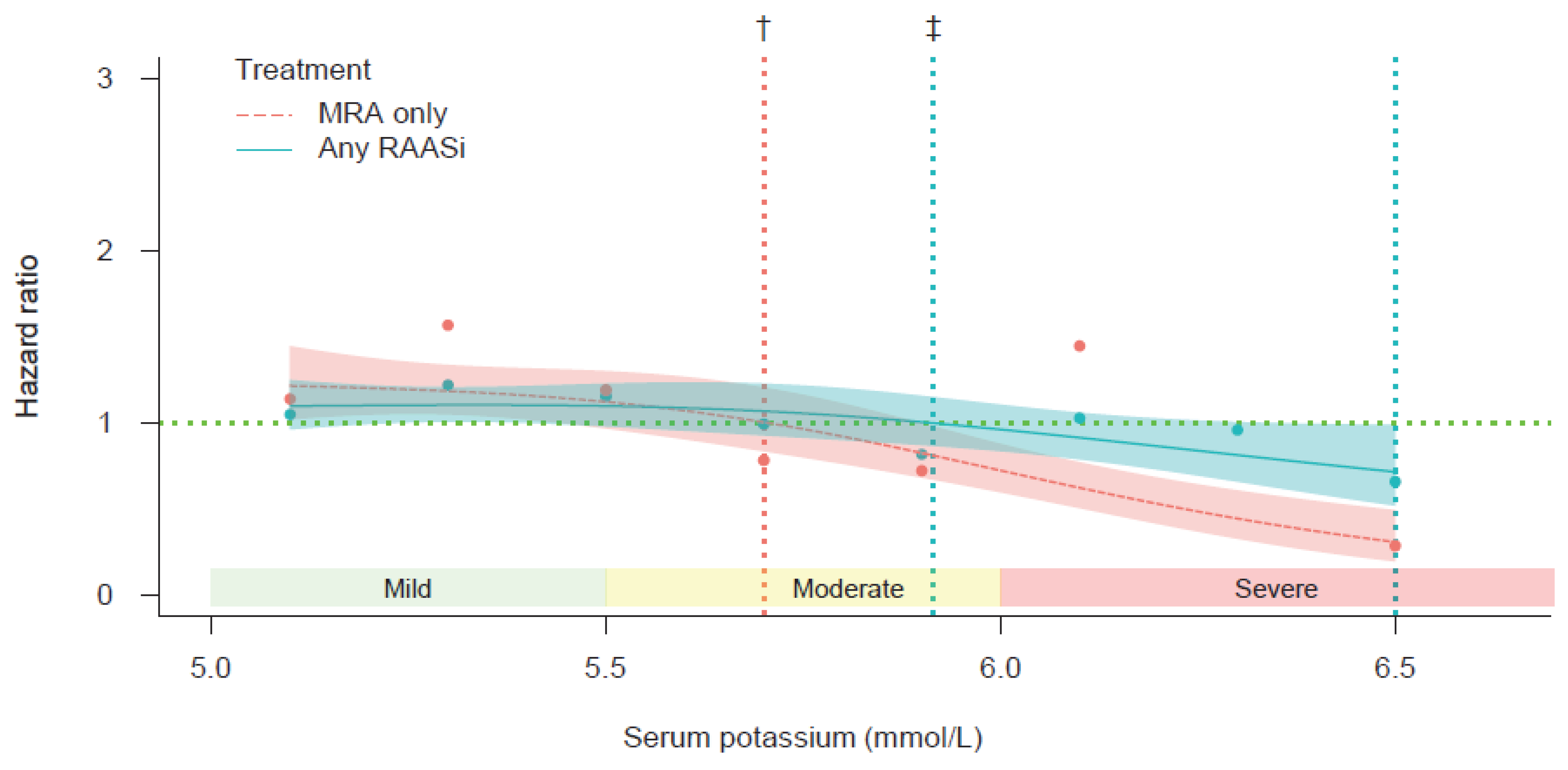
3.4. Cubic Spline Regression Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEi | angiotensin-converting enzyme inhibitor |
| ARB | angiotensin II receptor blocker |
| CKD | chronic kidney disease |
| CPS | calcium polystyrene sulfonate |
| eGFR | estimated glomerular filtration rate |
| ESC | European Society of Cardiology |
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
| HR | hazard ratio |
| ICD | International Classification of Diseases |
| MI | myocardial infarction |
| MRA | mineralocorticoid receptor antagonist |
| PS | propensity score |
| RAASi | renin–angiotensin–aldosterone system inhibitor |
| SD | standard deviation |
| SPS | sodium polystyrene sulfonate |
References
- Oliveros, E.; Oni, E.T.; Shahzad, A.; Kluger, A.Y.; Lo, K.B.; Rangaswami, J.; McCullough, P.A. Benefits and risks of continuing angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, and mineralocorticoid receptor antagonists during hospitalizations for acute heart failure. Cardiorenal Med. 2020, 10, 69–84. [Google Scholar] [CrossRef]
- Rosano, G.M.C.; Tamargo, J.; Kjeldsen, K.P.; Lainscak, M.; Agewall, S.; Anker, S.D.; Ceconi, C.; Coats, A.J.S.; Drexel, H.; Filippatos, G.; et al. Expert consensus document on the management of hyperkalaemia in patients with cardiovascular disease treated with renin angiotensin aldosterone system inhibitors: Coordinated by the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 180–188. [Google Scholar]
- Xie, X.; Liu, Y.; Perkovic, V.; Xiangling, L.; Ninomiya, T.; Hou, W.; Zhao, N.; Liu, L.; Lv, J.; Zhang, H.; et al. Renin-angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: A Bayesian network meta-analysis of randomized clinical trials. Am. J. Kidney Dis. 2016, 67, 728–741. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Turgeon, R.D.; Kolber, M.R.; Loewen, P.; Ellis, U.; McCormack, J.P. Higher versus lower doses of ACE inhibitors, angiotensin-2 receptor blockers and beta-blockers in heart failure with reduced ejection fraction: Systematic review and meta-analysis. PLoS ONE 2019, 14, e0212907. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Carrero, J.J.; Clegg, D.J.; Colbert, G.B.; Emmett, M.; Fishbane, S.; Hain, D.J.; Lerma, E.; Onuigbo, M.; Rastogi, A.; et al. Clinical Management of Hyperkalemia. Mayo Clin. Proc. 2021, 96, 744–762. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F. Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. N. Engl. J. Med. 2004, 351, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M. Hyperkalemia constitutes a constraint for implementing renin-angiotensin-aldosterone inhibition: The widening gap between mandated treatment guidelines and the real-world clinical arena. Kidney Int. Suppl. 2016, 6, 20–28. [Google Scholar] [CrossRef]
- Luo, J.; Brunelli, S.M.; Jensen, D.E.; Yang, A. Association between serum potassium and outcomes in patients with reduced kidney function. Clin. J. Am. Soc. Nephrol. 2016, 11, 90–100. [Google Scholar] [CrossRef]
- Collins, A.J.; Pitt, B.; Reaven, N.; Funk, S.; McGaughey, K.; Wilson, D.; Bushinsky, D.A. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am. J. Nephrol. 2017, 46, 213–221. [Google Scholar] [CrossRef]
- Tromp, J.; van der Meer, P. Hyperkalaemia: Aetiology, epidemiology, and clinical significance. Eur. Heart J. Suppl. 2019, 21, A6–A11. [Google Scholar] [CrossRef] [PubMed]
- Kashihara, N.; Kohsaka, S.; Kanda, E.; Okami, S.; Yajima, T. Hyperkalemia in real-world patients under continuous medical care in Japan. Kidney Int. Rep. 2019, 4, 1248–1260. [Google Scholar] [CrossRef] [PubMed]
- Linde, C.; Qin, L.; Bakhai, A.; Furuland, H.; Evans, M.; Ayoubkhani, D.; Palaka, E.; Bennett, H.; McEwan, P. Serum potassium and clinical outcomes in heart failure patients: Results of risk calculations in 21,334 patients in the UK. ESC Heart Fail. 2019, 6, 280–290. [Google Scholar] [CrossRef]
- Furuland, H.; McEwan, P.; Evans, M.; Linde, C.; Ayoubkhani, D.; Bakhai, A.; Palaka, E.; Bennett, H.; Qin, L. Serum potassium as a predictor of adverse clinical outcomes in patients with chronic kidney disease: New risk equations using the UK clinical practice research datalink. BMC Nephrol. 2018, 19, 211. [Google Scholar] [CrossRef]
- Epstein, M.; Reaven, N.L.; Funk, S.E.; McGaughey, K.J.; Oestreicher, N.; Knispel, J. Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors. Am. J. Manag. Care 2015, 21, S212–S220. [Google Scholar] [PubMed]
- Linde, C.; Bakhai, A.; Furuland, H.; Evans, M.; McEwan, P.; Ayoubkhani, D.; Qin, L. Real-world associations of renin-angiotensin-aldosterone system inhibitor dose, hyperkalemia, and adverse clinical outcomes in a cohort of patients with new-onset chronic kidney disease or heart failure in the United Kingdom. J. Am. Heart Assoc. 2019, 8, e012655. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 8 June 2022).
- Ministry of Health, Labour and Welfare. Number of Deaths and Percentage Distribution by Place of Occurrence, by Year. Available online: http://www.mhlw.go.jp/english/database/db-hh/xls/1-25.xls (accessed on 8 June 2022).
- Wetmore, J.B.; Yan, H.; Horne, L.; Peng, Y.; Gilbertson, D.T. Risk of hyperkalemia from renin-angiotensin-aldosterone system inhibitors and factors associated with treatment discontinuities in a real-world population. Nephrol. Dial. Transplant. 2021, 25, 826–839. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, M.; de Deco, P.; Xu, H.; Evans, M.; Lindholm, B.; Bellocco, R.; Barany, P.; Jernberg, T.; Lund, L.H.; Carrero, J.J. Incidence, predictors and clinical management of hyperkalaemia in new users of mineralocorticoid receptor antagonists. Eur. J. Heart Fail. 2018, 20, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Volterrani, M.; Perrone, V.; Sangiorgi, D.; Giacomini, E.; Iellamo, F.; Degli Esposti, L.; LHUs Study Group. Effects of hyperkalaemia and non-adherence to renin–angiotensin–aldosterone system inhibitor therapy in patients with heart failure in Italy: A propensity-matched study. Eur. J. Heart Fail. 2020, 22, 2049–2055. [Google Scholar] [CrossRef]
- Edner, M.; Benson, L.; Dahlström, U.; Lund, L.H. Association between renin-angiotensin system antagonist use and mortality in heart failure with severe renal insufficiency: A prospective propensity score-matched cohort study. Eur. Heart J. 2015, 36, 2318–2326. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, M.; Fu, E.L.; Xu, Y.; Savarese, G.; Dekker, F.W.; Lund, L.H.; Clase, C.M.; Sjölander, A.; Carrero, J.J. Stopping mineralocorticoid receptor antagonists after hyperkalaemia: Trial emulation in data from routine care. Eur. J. Heart Fail. 2021, 23, 1698–1707. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Poole-Wilson, P.A.; Armstrong, P.W.; Cleland, J.G.; Horowitz, J.D.; Massie, B.M.; Rydén, L.; Thygesen, K.; Uretsky, B.F. Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure. ATLAS Study Group. Circulation 1999, 100, 2312–2318. [Google Scholar] [CrossRef]
- Tsutsui, H.; Ide, T.; Ito, H.; Kihara, Y.; Kinugawa, K.; Kinugawa, S.; Makaya, M.; Murohara, T.; Node, K.; Saito, Y.; et al. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure. J. Card. Fail. 2021, 27, 1404–1444. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [PubMed]
- Savarese, G.; Bodegard, J.; Norhammar, A.; Sartipy, P.; Thuresson, M.; Cowie, M.R.; Fonarow, G.C.; Vaduganathan, M.; Coats, A.J.S. Heart failure drug titration, cessation, mortality and heart failure hospitalization risk: A multinational observational study (US, UK and Sweden). Eur. J. Heart Fail. 2021, 23, 1499–1511. [Google Scholar] [CrossRef] [PubMed]
- Cicoira, M.; Zanolla, L.; Rossi, A.; Golia, G.; Franceschini, L.; Brighetti, G.; Marino, P.; Zardini, P. Long-term, dose-dependent effects of spironolactone on left ventricular function and exercise tolerance in patients with chronic heart failure. J. Am. Coll. Cardiol. 2002, 40, 304–310. [Google Scholar] [CrossRef]
- Yaku, H.; Kato, T.; Morimoto, T.; Inuzuka, Y.; Tamaki, Y.; Ozasa, N.; Yamamoto, E.; Yoshikawa, Y.; Kitai, T.; Taniguchi, R.; et al. Association of mineralocorticoid receptor antagonist use with all-cause mortality and hospital readmission in older adults with acute decompensated heart failure. JAMA Netw. Open 2019, 2, e195892. [Google Scholar] [CrossRef] [PubMed]
- Japanese Circulation Society; Japanese Heart Failure Society. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure; Japanese Circulation Society: Tokyo, Japan, 2021; Available online: https://www.j-circ.or.jp/cms/wp-content/uploads/2021/03/JCS2021_Tsutsui.pdf (accessed on 8 June 2022). (In Japanese)
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Gal, T.B.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, P.; Dobre, D.; McMurray, J.J.V.; Swedberg, K.; Krum, H.; van Veldhuisen, D.J.; Shi, H.; Messig, M.; Vincent, J.; Girerd, N.; et al. Incidence, determinants, and prognostic significance of hyperkalemia and worsening renal function in patients with heart failure receiving the mineralocorticoid receptor antagonist eplerenone or placebo in addition to optimal medical therapy: Results from the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF). Circ. Heart Fail. 2014, 7, 51–58. [Google Scholar] [PubMed]
- Vardeny, O.; Claggett, B.; Anand, I.; Rossignol, P.; Desai, A.S.; Zannad, F.; Pitt, B.; Solomon, S.D. Randomized Aldactone Evaluation Study (RALES) Investigators. Incidence, predictors, and outcomes related to hypo- and hyperkalemia in patients with severe heart failure treated with a mineralocorticoid receptor antagonist. Circ. Heart Fail. 2014, 7, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Eschalier, R.; McMurray, J.J.V.; Swedberg, K.; van Veldhuisen, D.J.; Krum, H.; Pocock, S.J.; Shi, H.; Vincent, J.; Rossignol, P.; Zannad, F.; et al. Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: Analyses of the EMPHASIS-HF study subgroups (Eplerenone in Mild Patients Hospitalization and SurvIval Study in Heart Failure). J. Am. Coll. Cardiol. 2013, 62, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Wu, D.H.; Desai, A.; Rossignol, P.; Zannad, F.; Pitt, B.; Solomon, S.D.; RALES Investigators. Influence of baseline and worsening renal function on efficacy of spironolactone in patients with severe heart failure: Insights from RALES (Randomized Aldactone Evaluation Study). J. Am. Coll. Cardiol. 2012, 60, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.P.; Butler, J.; Rossignol, P.; Pitt, B.; Anker, S.D.; Kosiborod, M.; Lund, L.H.; Bakris, G.L.; Weir, M.R.; Zannad, F. Abnormalities of potassium in heart failure: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2020, 75, 2836–2850. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Khan, M.S.; Anker, S.D. Novel potassium binders as enabling therapy in heart failure. Eur. J. Heart Fail. 2019, 21, 550–552. [Google Scholar] [CrossRef] [PubMed]
- Silva-Cardoso, J.; Brito, D.; Frazão, J.M.; Ferreira, A.; Bettencourt, P.; Branco, P.; Fonseca, C. Management of RAASi-associated hyperkalemia in patients with cardiovascular disease. Heart Fail. Rev. 2021, 26, 891–896. [Google Scholar] [CrossRef]
- Zannad, F.; Ferreira, J.P.; Pitt, B. Potassium binders for the prevention of hyperkalaemia in heart failure patients: Implementation issues and future developments. Eur. Heart J. Suppl. 2019, 21 (Suppl. A), A55–A60. [Google Scholar] [CrossRef]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.J.; Glynn, R.J.; Avorn, J.; Stürmer, T. Variable selection for propensity score models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Any RAASi, Pre-Matching | Any RAASi, Post-Matching | MRA Group, Pre-Matching | MRA Group, Post-Matching | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Any RAASi Therapy (n = 5059) | RAASi Cessation (n = 1757) | RAASi Non-Cessation (n = 3302) | RAASi Cessation (n = 1709) | RAASi Non-Cessation (n = 1709) | Total (n = 2220) | MRA Cessation (n = 1172) | MRA Non-Cessation (n = 1048) | MRA Cessation (n = 903) | MRA Non-Cessation (n = 903) | |
| Age, years (mean ± SD) | 76.63 ± 10.96 | 77.85 ± 10.98 | 75.98 ± 10.89 | 77.64 ± 10.99 | 77.78 ± 10.76 | 77.77 ± 10.95 | 78.19 ± 10.95 | 77.30 ± 10.93 | 77.70 ± 11.22 | 77.49 ± 10.89 |
| Age group, years | ||||||||||
| 18–64 | 747 (14.8) | 238 (13.5) | 509 (15.4) | 237(13.9) | 202(11.8) | 291 (13.1) | 147 (12.5) | 144 (13.7) | 124 (13.7) | 119 (13.2) |
| 65–79 | 2019 (39.9) | 622 (35.4) | 1397 (42.3) | 612 (35.8) | 644 (37.7) | 808 (36.4) | 406 (34.6) | 402 (38.4) | 319 (35.3) | 344 (38.1) |
| ≥80 | 2293 (45.3) | 897 (51.1) | 1396 (42.3) | 860 (50.3) | 863 (50.5) | 1121 (50.5) | 619 (52.8) | 502 (47.9) | 460 (50.9) | 440 (48.7) |
| Sex, male | 2623 (51.8) | 879 (50.0) | 1744 (52.8) | 865 (50.6) | 841 (49.2) | 1071 (48.2) | 547 (46.7) | 524 (50.0) | 433 (48.0) | 438 (48.5) |
| Follow-up period, years (mean ± SD) | 2.8 ± 2.0 | 2.6 ± 1.7 | 2.9 ± 2.1 | 2.6 ± 1.8 | 2.6 ± 2.0 | 2.4 ± 1.9 | 2.5 ± 1.8 | 2.3 ± 2.1 | 2.4 ± 1.7 | 2.5 ± 2.1 |
| Serum potassium at index date, mmol/L (mean ± SD) | 5.37 ± 0.37 | 5.39 ± 0.40 | 5.36 ± 0.34 | 5.39 ± 0.41 | 5.36 ± 0.36 | 5.38 ± 0.39 | 5.39 ± 0.41 | 5.36 ± 0.35 | 5.39 ± 0.41 | 5.36 ± 0.36 |
| Serum potassium group, mmol/L | ||||||||||
| 5.1–<5.5 | 3743 (74.0) | 1257 (71.5) | 2486 (75.3) | 1227 (71.8) | 1266 (74.1) | 1637 (73.7) | 845 (72.1) | 792 (75.6) | 656 (72.6) | 686 (76.0) |
| 5.5–<6.0 | 1020 (20.2) | 382 (21.7) | 638 (19.3) | 365 (21.4) | 342 (20.0) | 455 (20.5) | 256 (21.8) | 199 (19.0) | 194 (21.5) | 170 (18.8) |
| 6.0–<6.5 | 188 (3.7) | 79 (4.5) | 109 (3.3) | 79 (4.6) | 62 (3.6) | 81 (3.6) | 42 (3.6) | 39 (3.7) | 31 (3.4) | 32 (3.5) |
| CKD | 3584 (70.8) | 1203 (68.5) | 2381 (72.1) | 1179 (69.0) | 1175 (68.8) | 1516 (68.3) | 814 (69.5) | 702 (67.0) | 605 (67.0) | 609 (67.4) |
| CKD stage * | ||||||||||
| 1 | 16 (0.4) | 6 (0.5) | 10(0.4) | 6 (0.5) | 5 (0.4) | 5 (0.3) | 2 (0.2) | 3 (0.4) | 2 (0.3) | 2 (0.3) |
| 2 | 173 (4.8) | 70 (5.8) | 103 (4.3) | 68 (5.8) | 65 (5.5) | 72 (4.7) | 44 (5.4) | 28 (4.0) | 27 (4.5) | 24 (3.9) |
| 3a | 624 (17.4) | 183 (15.2) | 441 (18.5) | 179 (15.2) | 157 (13.4) | 267 (17.6) | 129 (15.8) | 138 (19.7) | 112 (18.5) | 113 (18.6) |
| 3b | 1134 (31.6) | 342 (28.4) | 792 (33.3) | 336 (28.5) | 360 (30.6) | 531 (35.0) | 259 (31.8) | 272 (38.7) | 220 (36.4) | 222 (36.5) |
| 4 | 1196 (33.4) | 431 (35.8) | 765 (32.1) | 421 (35.7) | 413 (35.1) | 536 (35.4) | 320 (39.3) | 216 (30.8) | 200 (33.1) | 207 (34.0) |
| 5 | 441 (12.3) | 171 (14.2) | 270 (11.3) | 169 (14.3) | 175 (14.9) | 105 (6.9) | 60 (7.4) | 45 (6.4) | 44 (7.3) | 41 (6.7) |
| Diabetes | 2505 (49.5) | 763 (43.4) | 1742 (52.8) | 755 (44.2) | 743 (43.5) | 950 (42.8) | 489 (41.7) | 461 (44.0) | 397 (44.0) | 398 (44.1) |
| Hypertension | 4573 (90.4) | 1499 (85.3) | 3074 (93.1) | 1489 (87.1) | 1499 (87.7) | 1897 (85.5) | 980 (83.6) | 917 (87.5) | 771 (85.4) | 785 (86.9) |
| Other comorbidities | ||||||||||
| Myocardial infarction | 458 (9.1) | 169 (9.6) | 289 (8.8) | 165 (9.7) | 140 (8.2) | 205 (9.2) | 112 (9.6) | 93 (8.9) | 90 (10.0) | 77 (8.5) |
| Peripheral vascular disease | 1153 (22.8) | 364 (20.7) | 789 (23.9) | 361 (21.1) | 352 (20.6) | 481 (21.7) | 227 (19.4) | 254 (24.2) | 188 (20.8) | 200 (22.1) |
| Cerebrovascular disease | 1547 (30.6) | 503 (28.6) | 1044 (31.6) | 483 (28.3) | 498 (29.1) | 626 (28.2) | 298 (25.4) | 328 (31.3) | 248 (27.5) | 266 (29.5) |
| Chronic pulmonary disease | 1208 (23.9) | 400 (22.8) | 808 (24.5) | 395 (23.1) | 383 (22.4) | 569 (25.6) | 274 (23.4) | 295 (28.1) | 219 (24.3) | 232 (25.7) |
| Atrial fibrillation or atrial flutter | 1708 (33.8) | 593 (33.8) | 1115 (33.8) | 581 (34.0) | 594 (34.8) | 986 (44.4) | 510 (43.5) | 476 (45.4) | 402 (44.5) | 404 (44.7) |
| Valvular heart disease | 1205 (23.8) | 417 (23.7) | 788 (23.9) | 409 (23.9) | 414 (24.2) | 654 (29.5) | 347 (29.6) | 307 (29.3) | 257 (28.5) | 264 (29.2) |
| Acute kidney injury | 201 (4.0) | 76 (4.3) | 125 (3.8) | 74 (4.3) | 73 (4.3) | 89 (4.0) | 43 (3.7) | 46 (4.4) | 36 (4.0) | 37 (4.1) |
| Sepsis | 733 (14.5) | 242 (13.8) | 491 (14.9) | 239 (14.0) | 235 (13.8) | 342 (15.4) | 149 (12.7) | 193 (18.4) | 129 (14.3) | 136 (15.1) |
| Treatment for HF | ||||||||||
| ACEi and/or ARB | 4111 (81.3) | 1399 (79.6) | 2914 (88.2) | 1376 (80.5) | 1461 (85.5) | 1474 (66.4) | 800 (68.3) | 674 (64.3) | 610 (67.6) | 592 (65.6) |
| Beta-blocker | 2689 (53.2) | 874 (49.7) | 1815 (55.0) | 855 (50.0) | 944 (55.2) | 1296 (58.4) | 675 (57.6) | 621 (59.3) | 507 (56.1) | 550 (60.9) |
| Digoxin | 629 (12.4) | 202 (11.5) | 427 (12.9) | 196 (11.5) | 240 (14.0) | 398 (17.9) | 191 (16.3) | 207 (19.8) | 151 (16.7) | 166 (18.4) |
| Inotrope | 983 (19.4) | 389 (22.1) | 594 (18.0) | 373 (21.8) | 363 (21.2) | 547 (24.6) | 280 (23.9) | 267 (25.5) | 220 (24.4) | 215 (23.8) |
| MRA | 2220 (43.9) | 949 (54.0) | 1550 (46.9) | 913 (53.4) | 909 (53.2) | 2220 (100.0) | 1172 (100.0) | 1048 (100.0) | 903 (100.0) | 903 (100.0) |
| Hyperkalemia treatment at index date | ||||||||||
| Thiazide diuretics | 208 (4.1) | 55 (3.1) | 153 (4.6) | 55 (3.2) | 76 (4.4) | 80 (3.6) | 34 (2.9) | 40 (4.4) | 31 (3.4) | 39 (4.3) |
| Loop diuretics | 2428 (48.0) | 808 (46.0) | 1620 (49.1) | 791 (46.3) | 800 (46.8) | 1340 (60.4) | 660 (56.3) | 680 (64.9) | 556 (61.6) | 563 (62.3) |
| Glucose + insulin injection | 90 (1.8) | 30 (1.7) | 60 (1.8) | 29 (1.7) | 40 (2.3) | 46 (2.1) | 23 (2.0) | 23 (2.2) | 18 (2.0) | 18 (2.0) |
| Calcium gluconate | 70 (1.4) | 26 (1.5) | 44 (1.3) | 26 (1.5) | 28 (1.6) | 32 (1.4) | 18 (1.5) | 14 (1.3) | 15 (1.7) | 10 (1.1) |
| Sodium bicarbonate | 527 (10.4) | 211 (12.0) | 316 (9.6) | 209 (12.2) | 153 (9.0) | 201 (9.1) | 109 (9.3) | 92 (8.8) | 95 (10.5) | 74 (8.2) |
| Potassium binder (SPS/CPS) | 352 (7.0) | 129 (7.3) | 223 (6.8) | 125 (7.3) | 118 (6.9) | 91 (4.1) | 63 (5.4) | 28 (2.7) | 50 (5.5) | 26 (2.9) |
| Baseline | 1 Year after Index Date | ||
|---|---|---|---|
| n = 5059 | n = 4175 | ||
| Any RAASi | 5059 (100) | 2913 (69.8) | |
| No cessation 3302 | Cessation 1757 | ||
| ACEi only | 610 (12.1) | 402 (9.6) | |
| ARB only | 2128 (42.1) | 1537 (36.8) | |
| ACEi + ARB | 101 (2.0) | 70 (1.7) | |
| Any MRA | 2220 (43.9) | 907 (21.7) | |
| No cessation 1048 | Cessation 1172 | ||
| MRA only | 948 (18.7) | 315 (7.5) | |
| ACEi + MRA | 464 (9.2) | 198 (4.7) | |
| ARB + MRA | 772 (15.3) | 377 (9.0) | |
| ACEi + ARB + MRA | 36 (0.7) | 14 (0.3) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohsaka, S.; Okami, S.; Morita, N.; Yajima, T. Risk–Benefit Balance of Renin–Angiotensin–Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia. J. Clin. Med. 2022, 11, 5828. https://doi.org/10.3390/jcm11195828
Kohsaka S, Okami S, Morita N, Yajima T. Risk–Benefit Balance of Renin–Angiotensin–Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia. Journal of Clinical Medicine. 2022; 11(19):5828. https://doi.org/10.3390/jcm11195828
Chicago/Turabian StyleKohsaka, Shun, Suguru Okami, Naru Morita, and Toshitaka Yajima. 2022. "Risk–Benefit Balance of Renin–Angiotensin–Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia" Journal of Clinical Medicine 11, no. 19: 5828. https://doi.org/10.3390/jcm11195828