

Effects of Oral Nutritional Supplementation on Patients with Venous Ulcers: A Clinical Trial
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
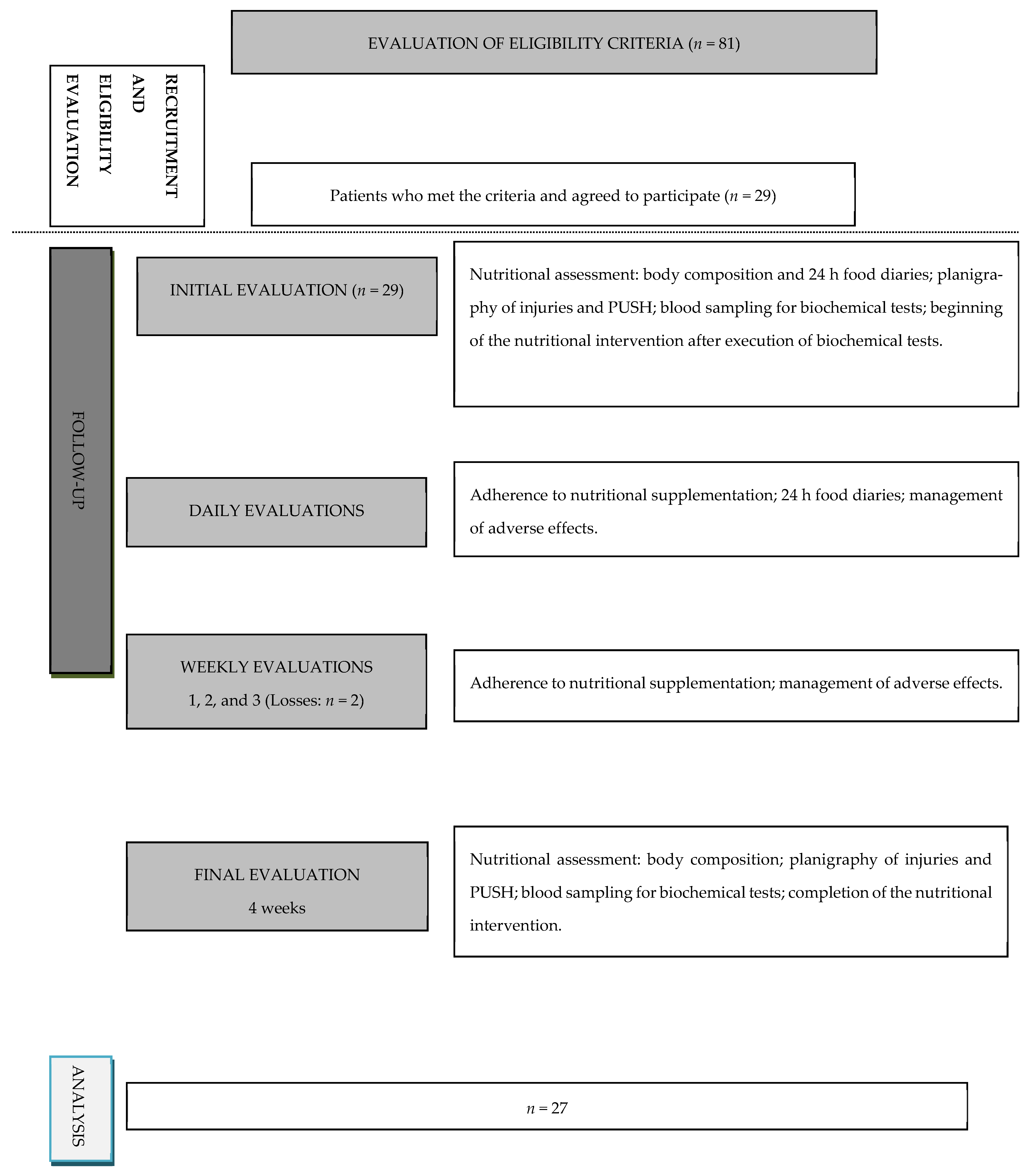
2.1. Study Design and Participants
2.2. Intervention Protocol, Follow-Up, and Adverse Events
2.3. Socioeconomic Characteristics and Associated Comorbidities
2.4. Dietary Intake and Anthropometric Measures
2.5. Injury Area, Healing Conditions, and Biochemical Data
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Dietary Intake
3.3. Anthropometric Measures, Follow-Up, and Adverse Effects
3.4. Injury Area, Healing Conditions, and Biochemical Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harding, K.; Dowsett, C.; Fias, L.; Jelnes, R.; Mosti, G.; Öien, R.; Partsch, H.; Reeder, S.W.I.; Senet, P.; Soriano, J.V.; et al. Simplifying venous leg ulcer management. In Consensus Recommendations; Wounds International: London, UK, 2015; pp. 1–25. [Google Scholar]
- Franks, P.; Barker, J.; Collier, M.; Gethin, G.; Haesler, E.; Jawien, A.; Laeuchli, S.; Mosti, G.; Probst, S.; Weller, C. Management of patients with venous leg ulcer: Challenges and current best practice. J. Wound Care 2016, 25, S1–S67. [Google Scholar] [CrossRef]
- Wild, T.; Rahbarnia, A.; Kellner, M.; Sobotka, L.; Eberlein, T. Basics in nutrition and wound healing. Nutrition 2010, 26, 862–866. [Google Scholar] [CrossRef] [PubMed]
- Verdú-Soriano, J.; Perdomo, E. Nutrición y heridas crónicas. In Serie Documentos Técnicos GNEAUPP; Grupo Nacional para el Estudio y Asesoramiento en Úlceras por Presión y Heridas Crónicas: Logroño, Spain, 2011; Volume 12, pp. 1–68. [Google Scholar]
- Haughey, L.; Barbul, A. Nutrition and lower extremity ulcers: Causality and/or treatment. Int. J. Low. Extrem. Wounds 2017, 16, 238–243. [Google Scholar] [CrossRef]
- Arribas-López, E.; Zand, N.; Ojo, O.; Snowden, M.J.; Kochhar, T. The effect of amino acids on wound healing: A systematic review and meta-analysis on arginine and glutamine. Nutrients 2021, 13, 2498. [Google Scholar] [CrossRef]
- Chow, O.; Barbul, A. Immunonutrition: Role in wound healing and tissue regeneration. Adv. Wound Care 2013, 3, 46–53. [Google Scholar] [CrossRef]
- McDaniel, J.C.; Szalacha, L.; Sales, M.; Roy, S.; Chafee, S.; Parinandi, N. EPA1DHA supplementation reduces PMN activation in microenvironment of chronic venous leg ulcers: A randomized, double-blind, controlled study. Wound Repair Regen. 2017, 25, 680–690. [Google Scholar] [CrossRef]
- Munoz, N.; Posthauer, M.E.; Cereda, E.; Schols, J.M.G.A.; Haesler, E. The Role of Nutrition for Pressure Injury Prevention and Healing: The 2019 International Clinical Practice Guideline Recommendations. Adv. Skin Wound Care 2020, 33, 123–136. [Google Scholar] [CrossRef]
- Tobón, J.; Whitney, J.D.; Jarrett, M. Nutritional status and wound severity of overweight and obese patients with venous leg ulcers: A pilot study. J. Vasc. Nurs. 2008, 26, 43–52. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, J.C.; Kemmner, K.G.; Rusnak, S. Nutritional profile of older adults with chronic venous leg ulcers: A pilot study. Geriatr. Nurs. 2015, 36, 381–386. [Google Scholar] [CrossRef]
- Renner, R.; Garibaldi, M.D.S.; Benson, S.; Ronicke, M.; Erfurt-Berge, C. Nutrition status in patients with wounds: A cross-sectional analysis of 50 patients with chronic leg ulcers or acute wounds. Eur. J. Dermatol. 2019, 29, 619–626. [Google Scholar] [CrossRef]
- Rojas, A.I.; Phillips, T.J. Patients with chronic leg ulcers show diminished levels of vitamins A and E, carotenes, and zinc. Dermatol. Surg. 1999, 25, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Burkiewicz, C.J.C.C.; Guadagnin, F.A.; Skare, T.L.; Nascimento, M.M.; Servin, S.C.N.; Souza, G.D. Vitamin D and skin repair: A prospective, double-blind and placebo controlled study in the healing of leg ulcers. Rev. Col. Bras. Cir. 2012, 39, 401–407. [Google Scholar] [CrossRef] [PubMed]
- ter Borg, S.; Verlaan, S.; Hemsworth, J.; Mijnarends, D.M.; Schols, J.M.G.A.; Luiking, Y.C.; Groot, L.C.P.G.M. Micronutrient intakes and potential inadequacies of community-dwelling older adults: A systematic review. Br. J. Nutr. 2015, 113, 1195–1206. [Google Scholar] [CrossRef]
- Engle-Stone, R.; Vosti, S.A.; Luo, H.; Kagin, J.; Tarini, A.; Adams, K.P.; French, C.; Brown, K.H. Weighing the risks of high intakes of selected micronutrients compared with the risks of deficiencies. Ann. N. Y. Acad. Sci. 2019, 1446, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Wissing, U.E.; Ek, A.C.; Wengström, Y.; Sköld, G.; Unosson, M. Can individualised nutritional support improve healing in therapy-resistant leg ulcers? J. Wound Care 2012, 11, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Cambridge, MA, USA, 2005; pp. 1–1331. [Google Scholar]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Posthauer, M.E.; Banks, M.; Dorner, B.; Schols, J.M.G.A. The role of nutrition in pressure ulcer management: National pressure ulcer advisory panel, European pressure ulcer advisory panel, and pan pacific pressure injury alliance white paper. Adv. Skin Wound Care 2015, 28, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Dorner, B.; Posthauer, M.E.; Thomas, D. National Pressure Ulcer Advisory Panel. The role of nutrition in pressure ulcer prevention and treatment: National pressure ulcer advisory panel white paper. Adv. Skin Wound Care 2009, 22, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Moore, Z.E.; Corcoran, M.A.; Patton, D. Nutritional interventions for treating foot ulcers in people with diabetes. Cochrane Database Syst. Rev. 2020, 7, CD011378. [Google Scholar] [CrossRef] [PubMed]
- Bechara, N.; Gunton, J.E.; Flood, V.; Hng, T.M.; McGloin, C. Associations between nutrients and foot ulceration in diabetes: A systematic review. Nutrients 2021, 13, 2576. [Google Scholar] [CrossRef]
- Basiri, R.; Spicer, M.; Levenson, C.; Ledermann, T.; Akhavan, N.; Arjmandi, B. Improving dietary intake of essential nutrients can ameliorate inflammation in patients with diabetic foot ulcers. Nutrients 2022, 14, 2393. [Google Scholar] [CrossRef] [PubMed]
- Barber, G.A.; Weller, C.D.; Gibson, S.J. Effects and associations of nutrition in patients with venous leg ulcers: A systematic review. J. Adv. Nurs. 2017, 7, 774–787. [Google Scholar] [CrossRef] [PubMed]
- Penny, H.; Flores, R.; Pennington, E.; Pedersen, A.; Tran, S. The role of macronutrients and micronutrients in wound healing: A narrative review. J. Wound Care 2022, 31 (Suppl. 5), S14–S22. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, G.P.; Elia, M.; Holdoway, A.; Stratton, R. A systematic review of compliance to oral nutritional supplements. Clin. Nutr. 2012, 31, 293–312. [Google Scholar] [CrossRef]
- Mościcka, P.; Cwajda-Białasik, J.; Jawień, A.; Szewczyk, M.T. Complex treatment of venous leg ulcers including the use of oral nutritional supplementation: Results of 12-week prospective study. Adv. Dermatol. Allergol. 2022, 39, 336–346. [Google Scholar] [CrossRef]
- McDaniel, J.C.; Belury, M.; Ahijevych, K.; Blakely, W. Omega-3 fatty acids effect on wound healing. Wound Repair Regen. 2008, 16, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Momen-Heravi, M.; Barahimi, E.; Razzaghi, R.; Bahmani, F.; Gilasi, H.R.; Asemi, Z. The effects of zinc supplementation on wound healing and metabolic status in patients with diabetic foot ulcer: A randomized, double-blind, placebo-controlled trial. Wound Repair Regen. 2017, 25, 512–520. [Google Scholar] [CrossRef]
- Schols, J.M.G.A.; Heyman, H.; Meijer, E.P. Nutritional support in the treatment and prevention of pressure ulcers: An overview of studies with an arginine enriched oral nutritional supplement. J. Tissue Viability 2009, 18, 72–79. [Google Scholar] [CrossRef]
- Cereda, E.; Gini, A.; Pedrolli, C.; Vanotte, A. Disease-specific, versus standard, nutritional support for the treatment of pressure ulcers in institutionalized older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2009, 57, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Van Anholt, R.D.; Sobotka, L.; Meijer, E.P.; Heyman, H.; Groen, H.W.; Topinková, E.; Van Leen, M.; Schols, J.M.G.A. Specific nutritional support accelerates pressure ulcer healing and reduces wound care intensity in non-malnourished patients. Nutrition 2010, 26, 867–872. [Google Scholar] [CrossRef]
- Cereda, E.; Klersy, C.; Serioli, M.; Crespi, A.; D’Andrea, F. A nutritional formula enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers. Ann. Intern. Med. 2015, 162, 167–174. [Google Scholar] [CrossRef]
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; de Maeseneer, M.; et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lym. Dis. 2020, 8, 342–352. [Google Scholar] [CrossRef]
- Fletcher, J.; Atkin, L.; Dowsett, C.; Hopkins, A.; Tickle, J.; Worboys, F.; Williams, A. Best Practice Statement: Holistic Management of Venous Leg Ulceration; Wounds UK: London, UK, 2016; pp. 1–20. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; Mchugh, P.R. “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiat. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Seabra, M.L.V.; Concílio, G.V.; Villares, J.B.; Carlini, E.A. Evaluation of the “Mini-Mental State” test in Brazilian volunteers and patients. Rev. ABP-APAL 1990, 12, 1–7. [Google Scholar]
- Bertolucci, P.H.F.; Brucki, S.M.D.; Campacci, S.R.; Juliano, Y. The Mini-Mental State Examination in an outpatient population: Influence of literacy. Arq. De Neuro-Psiquiatr. 1994, 52, 1–7. [Google Scholar] [CrossRef]
- Robson, M.C.; Cooper, D.M.; Aslam, R.; Gould, L.J.; Harding, K.G.; Margolis, D.J.; Ochs, D.E.; Serena, T.E.; Snyder, R.J.; Steed, D.L.; et al. Guidelines for the treatment of venous ulcers. Wound Repair Regen. 2006, 14, 649–662. [Google Scholar] [CrossRef]
- Márquez-Contreras, E. Evaluation of non-compliance in the clinical practice. Hipertensión 2008, 25, 205–213. [Google Scholar]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- World Health Organization (WHO). Physical status: The use and interpretation of anthropometry. In Report of a WHO Expert Committee; Technical Report Series, 854; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Lipschitz, D.A. Screening for nutritional status in the elderly. Prim. Care 1994, 21, 55–67. [Google Scholar] [CrossRef]
- Watanabe, T.; Owashi, K.; Kanauchi, Y.; Mura, N.; Takahara, M.; Ogino, T. The short-term reliability of grip strength measurement and the effects of posture and grip span. J. Hand Surg. Am. 2005, 30, 603–609. [Google Scholar] [CrossRef]
- Thomas, D.R.; Rodeheaver, G.T.; Bartolucci, A.A.; Franz, R.A.; Sussman, C.; Ferrell, B.A.; Cuddigan, J.; Stotts, N.A.; Maklebust, J. Pressure ulcer scale for healing: Derivation and validation of the PUSH tool. The PUSH task force. Adv. Wound Care 1997, 10, 96–101. [Google Scholar] [PubMed]
- Santos, V.L.C.G.; Azevedo, M.A.J.; Silva, T.S.; Carvalho, V.M.J.; Carvalho, V.F. Crosscultural adaptation of the pressure ulcer scale for healing to the portuguese language. Rev. Lat. Am. De Enferm. 2005, 13, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Hon, J.; Lagden, K.; McLaren, A.M.; O’Sullivan, D.; Orr, L.; Houghton, P.E.; Woodbury, M.G. A prospective, multicenter study to validate use of the PUSH in patients with diabetic, venous, and pressure ulcers. Ostomy Wound Manag. 2010, 56, 26–36. [Google Scholar]
- Alves, G.R.; Malaquias, S.G.; Bachion, M.M. Pressure Ulcer Scale for Healing (PUSH): Interobserver reliability in the evaluation of venous ulcers. Rev. Eletr. Enf. 2018, 20, 20–33. [Google Scholar]
- de Franciscis, S.; de Sarro, G.; Longo, P.; Buffone, G.; Molinari, V.; Stillitano, D.M.; Serra, R. Hyperhomocysteinaemia and chronic venous ulcers. Int. Wound J. 2015, 12, 22–26. [Google Scholar] [CrossRef]
- Serra, R.; Grande, R.; Butrico, L.; Buffone, G.; Calio, F.G.; Squillace, A.; de Franciscis, S. Effects of a new nutraceutical substance on clinical and molecular parameters in patients with chronic venous ulceration. Int. Wound J. 2016, 13, 88–96. [Google Scholar] [CrossRef]
- Raffoul, W.; Far, M.S.; Cayeux, M.C.; Berger, M.M. Nutritional status and food intake in nine patients with chronic low-limb ulcers and pressure ulcers: Importance of oral supplements. Nutrition 2006, 22, 82–88. [Google Scholar] [CrossRef]
- Neyens, J.C.L.; Cereda, E.; Meijer, E.P.; Lindholm, C.; Schols, J.M.G.A. Arginine-enriched oral nutritional supplementation in the treatment of pressure ulcers: A literature review. Wound Med. 2017, 16, 46–51. [Google Scholar] [CrossRef]
- Krejner, A.; Litwiniuk, M.; Grzela, T. LL-37 but not 25-hydroxy-vitamin D serum level correlates with healing of venous leg ulcers. Arch. Immunol. Et Ther. Exp. 2016, 65, 455–461. [Google Scholar] [CrossRef]
- Evans, D.C.; Corkins, M.R.; Malone, A.; Miller, S.; Mogensen, K.M.; Guenter, P.; Jensen, G.L.; ASPEN Malnutrition Commitee. The use of visceral proteins as nutrition markers: An ASPEN position paper. Nutr. Clin. Pract. 2021, 36, 22–28. [Google Scholar] [CrossRef]
- Norman, K.; Stobaus, N.; Gonzalez, M.C.; Schulzke, J.D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef]
- Flood, A.; Chung, A.; Parker, H.; Kearns, V.; O’Sullivan, T.A. The use of hand grip strenght as a predictor of nutrition status in hospital patients. Clin. Nutr. 2014, 33, 106–114. [Google Scholar] [CrossRef]
- Windsor, J.A.; Hill, G.L. Grip strength: A measure of the proportion of protein loss in surgical patients. Br. J. Surg. 1988, 75, 880–882. [Google Scholar] [CrossRef]
- Schlüssel, M.M.; Anjos, L.A.; Vasconcellos, M.T.L.; Kac, G. Reference values of handgrip dynamometry of healthy adults: A population based study. Clin. Nutr. 2008, 27, 601–607. [Google Scholar] [CrossRef]
- Mendes, J.; Amaral, T.F.; Borges, N.; Santos, A.; Padrão, P.; Moreira, P.; Afonso, C.; Negrão, R. Handgrip strength values of Portuguese older adults: A population based study. BMC Geriatr. 2017, 17, 191. [Google Scholar] [CrossRef]
- Labropoulos, N.; Wang, E.D.; Lanier, S.T.; Khan, S.U. Factors associated with poor healing and recurrence of venous ulceration. Plast. Reconstr. Surg. 2012, 129, 179–186. [Google Scholar] [CrossRef]
- Elia, M.; Normand, C.; Norman, K.; Laviano, A. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in the hospital setting. Clin. Nutr. 2016, 35, 370–380. [Google Scholar] [CrossRef]
- Stratton, R.; Smith, T.; Gabe, S. Managing Malnutrition to Improve Lives and Save Money; BAPEN: Redditch, UK, 2018; pp. 3–15. [Google Scholar]
- Tew, G.A.; Gumber, A.; McIntosh, E.; Kesterton, S.; King, B.; Michaels, J.A.; Klonizakis, M. Effects of supervised exercise training on lower-limb cutaneous microvascular reactivity in adults with venous ulcers. Eur. J. Appl. Physiol. 2018, 118, 321–329. [Google Scholar] [CrossRef]
- Nabil, S.; Eid, M.M.; Halim, A.E.; Mohsen, A.E.H.A.A.E.; Mohamady, H.M. Effect of Ankle Resisted Exercises on Venous Leg Ulcers Healing. Med. J. Cairo Univ. 2019, 87, 4071–4076. [Google Scholar] [CrossRef]
- O’Brien, J.; Finlayson, K.; Kerr, G.; Edwards, H. Evaluating the effectiveness of a self-management exercise intervention on wound healing, functional ability and health-related quality of life outcomes in adults with venous leg ulcers: A randomised controlled trial. Int. Wound J. 2017, 14, 130–137. [Google Scholar] [CrossRef]
- Azoubel, R.; Torres, G.V.; Silva, L.W.S.; Gomes, F.V.; Reis, L.A. Effects of the decongestive physiotherapy in the healing of venous ulcers. Rev. Da Esc. De Enferm. Da USP 2010, 44, 1085–1092. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Average | SD | Median | Minimum | Maximum |
|---|---|---|---|---|---|
| Age (years) | 59.4 | 11.2 | 61.0 | 42.0 | 86.0 |
| Per capita income (US$ *) | 235.4 | 172.2 | 191.0 | 57.31 | 859.6 |
| Level of education (years) | 6.3 | 4.7 | 6.0 | 0.0 | 13.0 |
| Injury duration (months) | 33.3 | 48.0 | 6.0 | 1.0 | 192.0 |
| Injury area (cm2) | 11.3 | 12.1 | 5.9 | 0.5 | 40.3 |
| PUSH score | 11.7 | 3.3 | 12.0 | 5.0 | 17.0 |
| Variable | Initial | Final | p-Value a,b |
|---|---|---|---|
| TEI (kcal/day) * | 2023.9 (1627.9–2608.2) | 2493.9 (2073.5–2989.8) | <0.001 b |
| TEI (kcal/kg/day) * | 24.5 (17.9–36.9) | 29.3 (26.5–7.7) | <0.001 b |
| CHO (g/day) | 343.1 ± 179.4 | 344.8 ± 116.5 | 0.895 a |
| CHO (%/day) | 58.4 ± 8.3 | 52.0 ± 6.1 | <0.001 a |
| CHO (g/kg/day) * | 3.6 (2.5–6.1) | 3.9 (3.2–5.2) | 0.691 b |
| Simple carbohydrates (g/day) | 130.1 ± 93.5 | 105.9 ± 53.3 | <0.001 a |
| LIP (g/day) | 63.6 ± 22.1 | 84.4 ± 29.5 | 0.140 a |
| LIP (%/day) | 27.0 ± 6.0 | 28.7 ± 4.2 | <0.001 a |
| LIP (g/kg/day) | 0.79 ± 0.3 | 1.0 ± 0.3 | <0.001 a |
| MUFA (g/day) | 22.7 ± 7.0 | 33.6 ± 9.9 | <0.001 a |
| PUFA (g/day) | 13.2 ± 5.9 | 19.0 ± 8.5 | <0.001 a |
| SAT (g/day) | 21.1 ± 9.1 | 24.9 ± 10.3 | 0.085 a |
| TRANS FATS (g/day) | 0.6 ± 2.1 | 0.22 ± 0.24 | <0.001 a |
| PTN (g/day) | 77.9 ± 33.2 | 122.1 ± 32.4 | <0.001 a |
| PTN (%/day) * | 14.9 (11.9–16.4) | 19.0 (16.4–20.8) | <0.001 b |
| PTN (g/kg/day) | 0.96 ± 0.40 | 1.5 ± 0.4 | 0.000 a |
| Arginine (g/day) * | 3.6 (2.6–4.7) | 10.3 (9.5–11.6) | 0.000 b |
| Vitamin A (μg/day) | 146.2 ± 102.3 | 710.3 ± 144.1 | <0.001 a |
| Vitamin C (mg/day) | 242.2 ± 237.4 | 743.2 ± 193.0 | <0.001 a |
| Iron (mg/day) | 12.0 ± 5.9 | 24.9 ± 5.2 | <0.001 a |
| Magnesium (mg/day) * | 250.4 (190.3–318.8) | 430.5 (360.6–494.6) | <0.001 b |
| Copper (mg/day) * | 1.1 (0.8–1.3) | 2.7 (2.7–4.0) | <0.001 b |
| Selenium (μg/day) | 90.4 ± 34.5 | 235.3 ± 36.2 | <0.001 a |
| Zinc (mg/day) * | 11.1 (8.1–14.2) | 30.5 (27.2–35.1) | <0.001 b |
| Nutrient | Before Supplementation (%) | After Supplementation (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Below | Normal | Above ** | Below | Normal | Above ** | ||
| Iron | 29.6 | 70.4 | 0 | 0 | 0 | 100 | 0.007 |
| Magnesium | 74.1 | 11.1 | 14.8 | 14.8 | 0 | 85.2 | <0.001 |
| Copper | 33.3 | 66.7 | 0 | 0 | 0 | 100 | <0.001 |
| Selenium | 18.5 | 81.5 | 0 | 0 | 0 | 100 | 0.062 |
| Zinc | 29.6 | 70.4 | 0 | 0 | 0 | 100 | 0.001 |
| Vitamin A | 100 | 0 | 0 | 67.7 | 0 | 32.3 | 0.003 |
| Vitamin C | 26.9 | 73.1 | 0 | 0 | 0 | 100 | 0.015 |
| TEI (kcal/kg/day) | 74.1 | 3.7 | 22.2 | 55.6 | 11.2 | 33.2 | 1 |
| PTN (g/kg/day) | 77.8 | 7.4 | 14.8 | 48.1 | 18.5 | 33.4 | <0.001 |
| Variable | Initial | Final | p-Value a,b |
|---|---|---|---|
| Hematocrit (%) | 41.5 ± 5.0 | 41.6 ± 4.1 | 0.932 a |
| Hemoglobin (g/dL) | 13.6 ± 1.6 | 13.85 ± 1.36 | 0.156 a |
| Fasting glycemia (mg/dL) * | 97.0 (86.9–107.5) | 96.0 (84–105) | 0.779 b |
| Albumin (g/dL) * | 4.0 (3.6–4.3) | 4.1 (3.7–4.3) | 0.794 b |
| CRP (mg/L) * | 6.0 (6–6) | 6.0 (6–8.5) | 0.425 b |
| Body weight (kg) * | 88.0 (71.4–94.7) | 88.0 (72.5–94.9) | 0.003 b |
| BMI (kg/m2) * | 31.3 (28.3–34.4) | 31.34 (28.7–40.7) | 0.002 b |
| AC (cm) | 33.7 ± 4.4 | 33.9 ± 4.2 | 0.207 a |
| AMC (cm) | 25.9 ± 2.8 | 26.3 ± 3.1 | 0.179 a |
| TSF (mm) | 24.7 ± 10.3 | 24.2 ± 9.7 | 0.532 a |
| HS (kgf) * | 21.0 (17.5–33) | 24.0 (18–34) | 0.010 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melo, P.G.; Mota, J.F.; Nunes, C.A.d.B.; Malaquias, S.G.; Coelho, A.S.G.; Soriano, J.V.; Bachion, M.M. Effects of Oral Nutritional Supplementation on Patients with Venous Ulcers: A Clinical Trial. J. Clin. Med. 2022, 11, 5683. https://doi.org/10.3390/jcm11195683
Melo PG, Mota JF, Nunes CAdB, Malaquias SG, Coelho ASG, Soriano JV, Bachion MM. Effects of Oral Nutritional Supplementation on Patients with Venous Ulcers: A Clinical Trial. Journal of Clinical Medicine. 2022; 11(19):5683. https://doi.org/10.3390/jcm11195683
Chicago/Turabian StyleMelo, Paulla Guimarães, João Felipe Mota, Cynthia Assis de Barros Nunes, Suelen Gomes Malaquias, Alexandre Siqueira Guedes Coelho, José Verdú Soriano, and Maria Márcia Bachion. 2022. "Effects of Oral Nutritional Supplementation on Patients with Venous Ulcers: A Clinical Trial" Journal of Clinical Medicine 11, no. 19: 5683. https://doi.org/10.3390/jcm11195683