
Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Articles Selection
2.2. Data Extraction
2.3. Outcomes of Interest
2.4. Statistical Analysis
2.5. Quality and Publication Bias Assessment
3. Results
3.1. Articles Selection and Patient Demographics
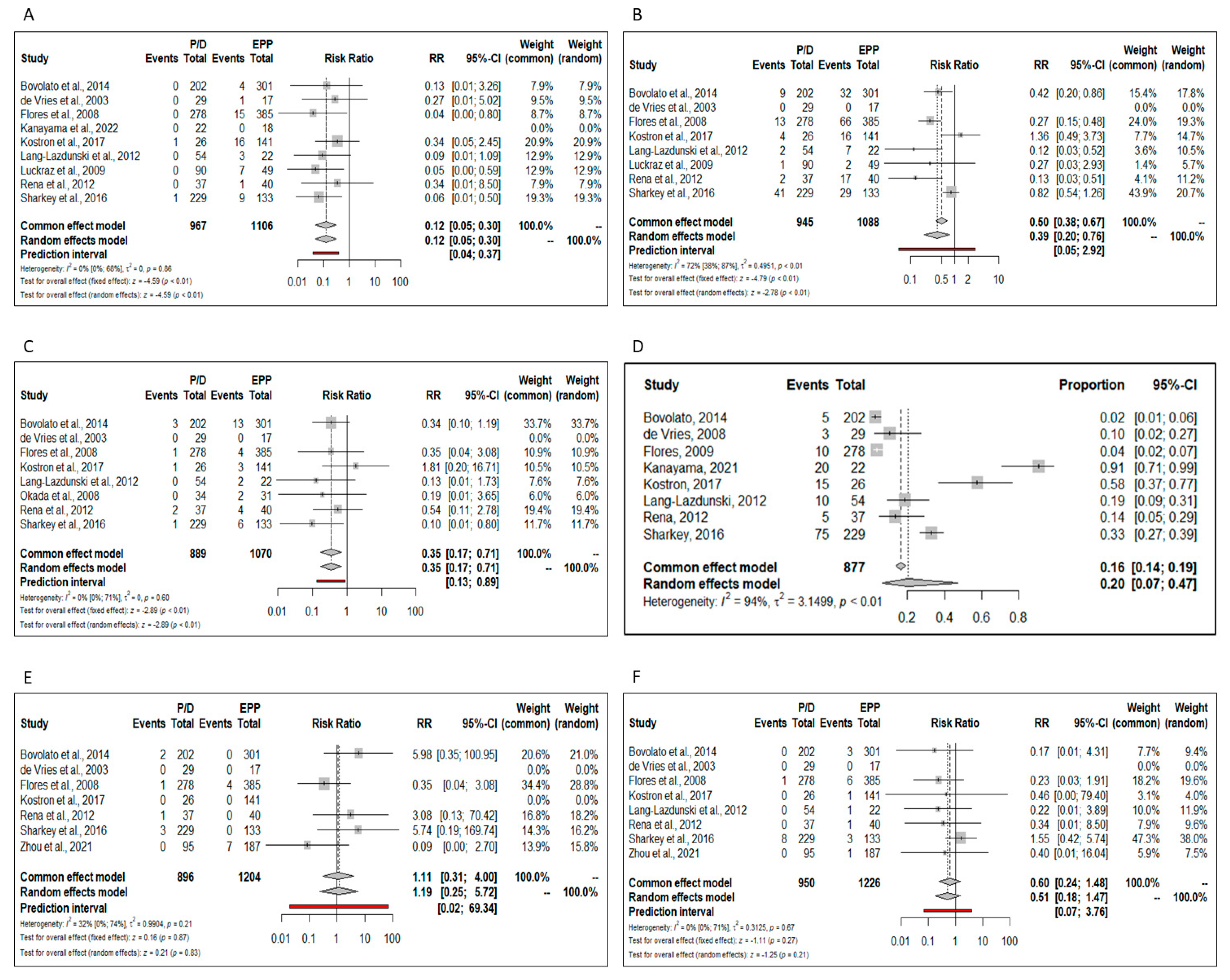
3.2. Meta-Analysis: Primary Outcomes
3.3. Meta-Analysis: Secondary Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagner, J.C.; Sleggs, C.A.; Marchand, P. Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province. Br. J. Ind. Med. 1960, 17, 260–271. [Google Scholar] [CrossRef]
- Taioli, E.; Wolf, A.S.; Flores, R.M. Meta-analysis of survival after pleurectomy decortication versus extrapleural pneumonectomy in mesothelioma. Ann. Thorac. Surg. 2015, 99, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Tian, D.; Park, J.; Allan, J.; Pataky, K.A.; Yan, T.D. A systematic review and meta-analysis of surgical treatments for malignant pleural mesothelioma. Lung Cancer 2014, 83, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Magouliotis, D.E.; Tasiopoulou, V.S.; Athanassiadi, K. Updated meta-analysis of survival after extrapleural pneumonectomy versus pleurectomy/decortication in mesothelioma. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 312–320. [Google Scholar] [CrossRef]
- Bertoglio, P.; Korasidis, S. Extrapleural Pneumonectomy and Pleurectomy Decortication: Can We Really Compare Their Survival? Ann. Thorac. Surg. 2015, 100, 1508–1509. [Google Scholar] [CrossRef] [PubMed]
- Garner, P.; Hopewell, S.; Chandler, J.; MacLehose, H.; Schünemann, H.J.; Akl, E.A.; Beyene, J.; Chang, S.; Churchill, R.; Dearness, K.; et al. Panel for updating guidance for systematic reviews (PUGs). When and how to update systematic reviews: Consensus and checklist. BMJ 2016, 354, i3507, Erratum in BMJ 2016, 354, i4853. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Rice, D.; Rusch, V.; Pass, H. Recommendations for uniform definitions of surgical techniques for malignant pleural mesothelioma: A consensus report of the International Association for the Study of Lung Cancer International Staging Committee and the International Mesothelioma Interest. J. Thorac. 2011, 6, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley and Sons: Chichester, UK, 2009. [Google Scholar]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.N.M.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Parmar, M.K. Restricted mean survival time: An alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med. Res. Methodol. 2013, 13, 152. [Google Scholar]
- Viechtbauer, W. Model checking in meta-analysis. In Handbook of Meta-Analysis; Schmid, C.H., Stijnen, T., White, I.R., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 219–254. [Google Scholar]
- Stang, A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in metaanalyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Bovolato, P.; Casadio, C.; Billè, A.; Ardissone, F.; Santambrogio, L.; Ratto, G.B.; Garofalo, G.; Bedini, A.V.; Garassino, M.; Porcu, L.; et al. Does surgery improve survival of patients with malignant pleural mesothelioma? A multicenter retro- spective analysis of 1365 consecutive patients. J. Thorac. Oncol. 2014, 9, 390–396. [Google Scholar] [CrossRef]
- De Vries, W.J.; Long, M.A. Treatment of mesothelioma in Bloemfon- tein, South Africa. Eur. J. Cardiothorac. Surg. 2003, 24, 434–440. [Google Scholar] [CrossRef]
- Flores, R.M.; Pass, H.; Seshan, V.E.; Dycoco, J.; Zakowski, M.; Carbone, M.; Bains, M.S.; Rusch, V. Extrapleural pneumonectomy versus pleurectomy/decortication in the surgical management of malignant pleural mesothelioma: Results in 663 patients. J. Thorac. Cardiovasc. Surg. 2008, 135, 620–626.e3. [Google Scholar] [CrossRef] [PubMed]
- Kai, Y.; Tsutani, Y.; Tsubokawa, N.; Ito, M.; Mimura, T.; Miyata, Y.; Okada, M. Prolonged post-recurrence survival following pleurectomy/decortication for malignant pleural mesothelioma. Oncol. Lett. 2019, 17, 3607–3614. [Google Scholar] [CrossRef]
- Kanayama, M.; Mori, M.; Matsumiya, H.; Taira, A.; Shinohara, S.; Takenaka, M.; Kuroda, K.; Tanaka, F. Surgical strategy for malignant pleural mesothelioma: The superiority of pleurectomy/decortication. Surg. Today 2022, 52, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Kostron, A.; Friess, M.; Inci, I.; Hillinger, S.; Schneiter, D.; Gelpke, H.; Stahel, R.; Seifert, B.; Weder, W.; Opitz, I. Propensity matched comparison of extrapleural pneumonec- tomy and pleurectomy/decortication for mesothelioma patients. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 740–746. [Google Scholar] [CrossRef]
- Lang-Lazdunski, L.; Bille, A.; Lal, R.; Cane, P.; McLean, E.; Landau, D.; Steele, J.; Spicer, J. Pleurectomy/decortication is superior to extrapleural pneu- monectomy in the multimodality management of patients with malignant pleural mesothelioma. J. Thorac. Oncol. 2012, 7, 737–743. [Google Scholar] [CrossRef]
- Luckraz, H.; Rahman, M.; Patel, N.; Szafranek, A.; Gibbs, A.R.; Butchart, E.G. Three decades of experience in the surgical multi-modality management of pleural mesothelioma. Eur. J. Cardiothorac. Surg. 2010, 37, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Mimura, T.; Ohbayashi, C.; Sakuma, T.; Soejima, T.; Tsubota, N. Radical surgery for malignant pleural mesothelioma: Results and prognosis. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Rena, O.; Casadio, C. Extrapleural pneumonectomy for early stage malignant pleural mesothelioma: A harmful procedure. Lung Cancer 2012, 77, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, A.J.; Tenconi, S.; Nakas, A.; Waller, D.A. The effects of an intentional transition from extrapleural pneumonectomy to extended pleurectomy/decortication. Eur. J. Cardiothorac. Surg. 2016, 49, 1632–1641. [Google Scholar] [CrossRef]
- Verma, V.; Ahern, C.A.; Berlind, C.G.; Lindsay, W.D.; Sharma, S.; Shabason, J.; Culligan, M.J.; Grover, S.; Friedberg, J.S.; Simone, C.B. National Cancer Database Report on pneumonectomy versus lung-sparing surgery for malignant pleural mesothelioma. J. Thorac. Oncol. 2017, 12, 1704–1714. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Rice, D.C.; Tsao, A.S.; Lee, P.P.; Haymaker, C.L.; Corsini, E.M.; Antonoff, M.B.; Hofstetter, W.L.; Rajaram, R.; Roth, J.A.; et al. Extrapleural Pneumonectomy Versus Pleurectomy/Decortication for Malignant Pleural Mesothelioma. Ann. Thorac. Surg. 2022, 113, 200–208. [Google Scholar] [CrossRef]
- Weder, W.; Stahel, R.A.; Baas, P.; Dafni, U.; de Perrot, M.; McCaughan, B.C.; Nakano, T.; Pass, H.I.; Robinson, B.W.; Rusch, V.W.; et al. The MARS feasibility trial: Conclusions not supported by data. Lancet Oncol. 2011, 12, 1093–1094. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year (Reference Number) | Country | Study Design | P/D Approach | Patients, n | Female, n (%) | Mean Age (Range) | Stage | NOS | Neoadjuvant/Adjuvant | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EPP | P/D | EPP | P/D | EPP | P/D | |||||||
| Bovolato et al., 2014 [16] | Italy | R | P/D | 301 | 202 | 76 (25.3) | 53 (26.2) | 58.7 (33–78) | 62.5 (30–87) | I: 9.5%; II: 27.6%; ≥III: 19%; ND: 43.7% (ND) | 6 | adjuvant CT RT |
| de Vries et al., 2003 [17] | South Africa | R | P/D | 17 | 29 | – | – | – | – | I–III ** | 5 | adjuvant CT RT |
| Flores et al., 2008 [18] | USA | R | Extended P/D | 385 | 278 | 69 (18) | 58 (21) | 60 | 63 | I: 2%; II: 95%; III: 24%; IV: 16%; ND: 48% *** | 7 | adjuvant CT RT |
| Kai et al., 2019 [19] | Japan | R | Extended P/D | 29 | 15 | 0 (0) | 0 (0) | 64 (42–73) | 66 (48–72) | I–IV * | 6 | neoadjuvant + adjuvant |
| Kanayama et al., 2022 [20] | Singapore | R | Extended P/D | 18 | 22 | 1 (5.6) | 3 (13.6) | 64.0 (51–77) | 69.5 (54–82) | IA–IIIB * | 6 | adjuvant |
| Kostron et al., 2017 [21] | Switzerland | R PSM | P/D and extended P/D | 141 | 26 | 16 (11) | 1 (4) | 61 (36–73) | 66 (34–77) | I–IV * | 7 | neoadjuvant CT |
| Lang-Lazdunski et al., 2012 [22] | UK | P | P/D and extended P/D | 22 | 54 | 2 (8.1) | 7 (13) | 62 (52–68) | 62.5 (45–74) | I–IV * | 6 | neoadjuvant + adjuvant |
| Luckraz et al., 2009 [23] | UK | R | P/D | 49 | 90 | 0 (0) | 4 (12) | 57.8 (12.6) | 63.5 (9.1) | I–III ** | 5 | neoadjuvant + adjuvant |
| Okada et al., 2008 [24] | Japan | R | Extended P/D | 31 | 34 | 4 (13) | 3 (9) | 60 (35–72) | 60 (37–78) | I–IV * | 6 | neoadjuvant + adjuvant |
| Rena et al., 2012 [25] | Italy | R | P/D | 40 | 37 | 29 (27) | 6 (32) | 56 ± 11 ° | 58.5 ± 9.5 ° | I, II (ND) | 6 | neoadjuvant + adjuvant |
| Sharkey et al., 2016 [26] | UK, Italy | R | Extended P/D | 133 | 229 | 19 (14) | 33 (14) | 57 (14–70) | 65 (42–81) | I: 4%; II: 14%; III: 57%; IV: 25% * | 6 | neoadjuvant + adjuvant |
| Verma et al., 2017 [27] | USA | R | Extended P/D | 271 | 1036 | 60 (22) | 217 (21) | 65 (58–71) | 69 (62–76) | I–IV (ND) | 7 | adjuvant CT RT |
| Zhou et al., 2021 [28] | USA | R PSM | ND | 187 | 95 | 32 (17.1) | 24 (26.3) | 61 (56–67) | 65 (61–71) | I–III (ND) | 6 | adjuvant RT |
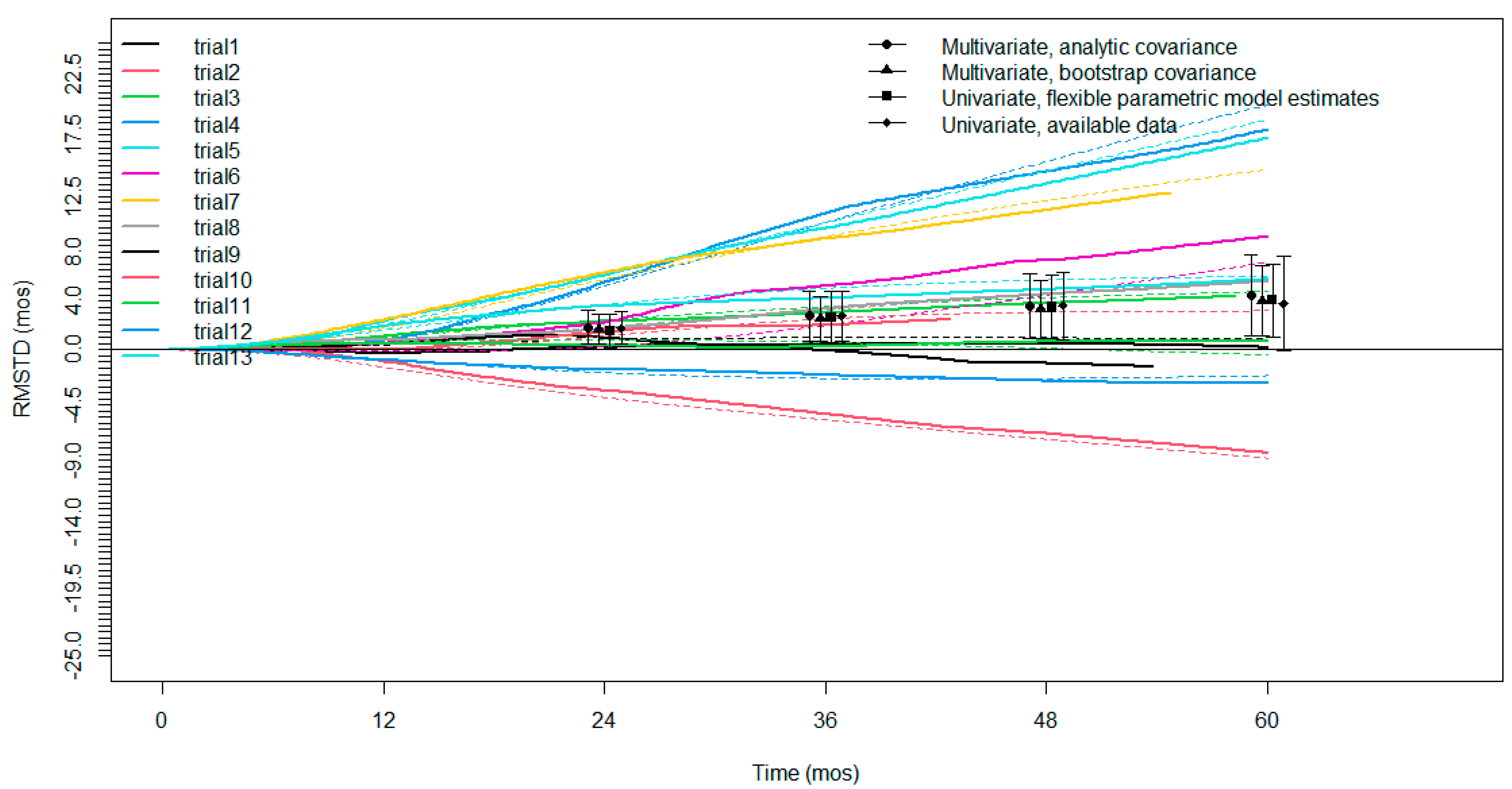
| Time Horizon | No. Trials | RMSTD (Months) | SE | 95% CI | p Value |
|---|---|---|---|---|---|
| 12 months | 13 | 0.5 | 0.3 | 0.03 to 1.05 | 0.038 |
| 24 months | 13 | 1.7 | 0.6 | 0.4 to 2.98 | 0.010 |
| 36 months | 13 | 2.6 | 1.0 | 0.63 to 4.49 | 0.009 |
| 48 months | 12 | 3.4 | 1.3 | 0.78 to 5.94 | 0.01 |
| 60 months | 9 | 4.2 | 1.6 | 1.0 to 7.46 | 0.01 |
| Authors, Year (Reference Number) | Nunber of Patients | 30 Days Mortality | 90 Days Mortality | Total Complications | Atrial Fibrillation | Bleeding | Pulmonary Embolism | Miocardial Infarction | Empyema | Prolongued Air Leaks | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | EPP | P/D | |
| Bovolato et al., 2014 [16] | 301 | 202 | 4.1% | 2.6% | 6.9% | 6% | 21.6% | 10.4% | 10.6% | 4.5% | 4.3% | 1.5% | 1% | 0% | 0% | 1% | 1.3% | 0% | 0% | 1.3% |
| de Vries et al., 2003 [17] | 17 | 29 | 5.8% | 3.8% | N.A. | N.A. | 5.9% | 31% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 5.9% | 0% | 0% | 1% |
| Flores et al., 2008 [18] | 385 | 278 | 7% | 4% | N.A. | N.A. | 39.4% | 17.6% | 17.1% | 4.7% | 1% | 0.4% | 1.6% | 0.4% | 1% | 0.4% | 3.9% | 0% | 0% | 3.6% |
| Kai et al., 2019 [19] | 29 | 15 | N.A. | N.A. | 6.9% | 0% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. |
| Kanayama et al., 2022 [20] | 18 | 22 | 5.6% | 0% | 5.6% | 0% | 83.3% | 95.5% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | 0% | 0% | 0% | 91% |
| Kostron et al., 2017 [21] | 141 | 26 | 2% | 0% | 8% | 0% | 38% | 58% | 11.3% | 15.4% | 2.1% | 3.8% | 0.7% | 0% | 0% | 0% | 11.3% | 3.8% | 0% | 57.7% |
| Lang-Lazdunski et al., 2012 [22] | 22 | 54 | 4.5% | 0% | N.A. | N.A. | 68% | 27.7% | 31.8% | 3.7% | 9% | 0% | 4.5% | 0% | N.A. | N.A. | 13.6% | 0% | 0% | 45.5% |
| Luckraz et al., 2009 [23] | 49 | 90 | 8.2% | 1.1% | N.A. | N.A. | 48.9% | 17.7% | 4% | 1% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | 14.3% | 0% | N.A. | N.A. |
| Okada et al., 2008 [24] | 31 | 34 | 3.2% | 0% | N.A. | N.A. | 48% | 15% | N.A. | N.A. | 6.5% | 0% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. |
| Rena et al., 2012 [25] | 40 | 37 | 5% | 0% | N.A. | N.A. | 62% | 24% | 42.5% | 5.4% | 10% | 5.4% | 2.5% | 0% | 0% | 2.5% | 2.7% | 0% | 0% | 13.5% |
| Sharkey et al., 2016 [26] | 133 | 229 | 6% | 3.5% | 13.5% | 9.2% | 88.7% | 93% | 21.8% | 17.9% | 4.5% | 0.4% | 2.3% | 3.5% | 0% | 1.3% | 6.8% | 4.4% | 0% | 32.8% |
| Verma et al., 2017 [27] | 271 | 1036 | 5% | 5% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. |
| Zhou et al., 2021 [28] | 187 | 95 | 7% | 0% | 18% | 5% | N.A. | N.A. | N.A. | N.A. | N.A. | N.A. | 0.5% | 0% | 3.7% | 0% | N.A. | N.A. | N.A. | N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danuzzo, F.; Maiorca, S.; Bonitta, G.; Nosotti, M. Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma. J. Clin. Med. 2022, 11, 5544. https://doi.org/10.3390/jcm11195544
Danuzzo F, Maiorca S, Bonitta G, Nosotti M. Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma. Journal of Clinical Medicine. 2022; 11(19):5544. https://doi.org/10.3390/jcm11195544
Chicago/Turabian StyleDanuzzo, Federica, Sebastiano Maiorca, Gianluca Bonitta, and Mario Nosotti. 2022. "Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma" Journal of Clinical Medicine 11, no. 19: 5544. https://doi.org/10.3390/jcm11195544