
Advances in Optical Coherence Tomography Imaging Technology and Techniques for Choroidal and Retinal Disorders

 ,
,
Abstract
:1. Introduction
2. Recent Advances in OCT Technology and Techniques
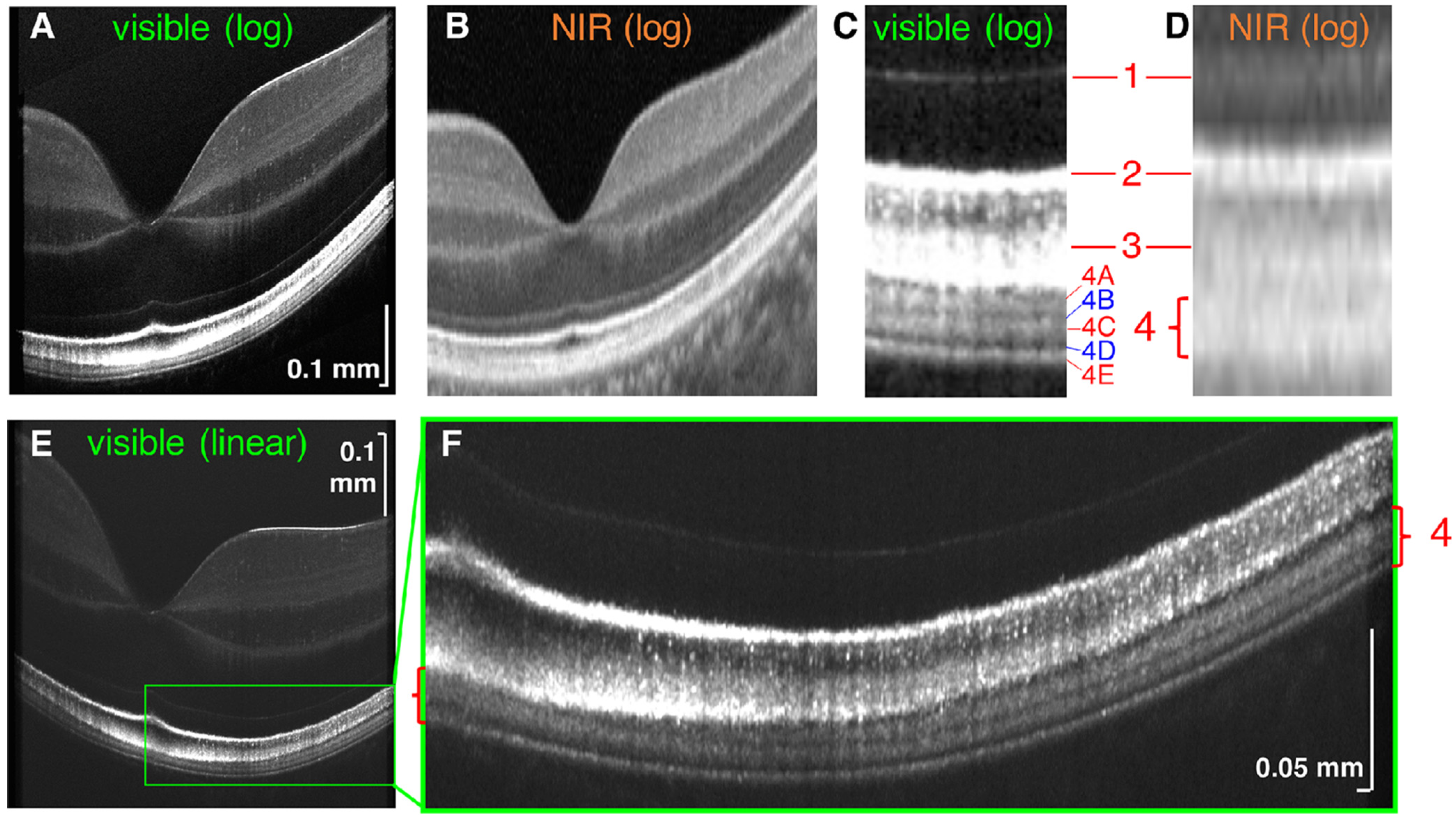
3. Visible Light OCT (Vis-OCT)
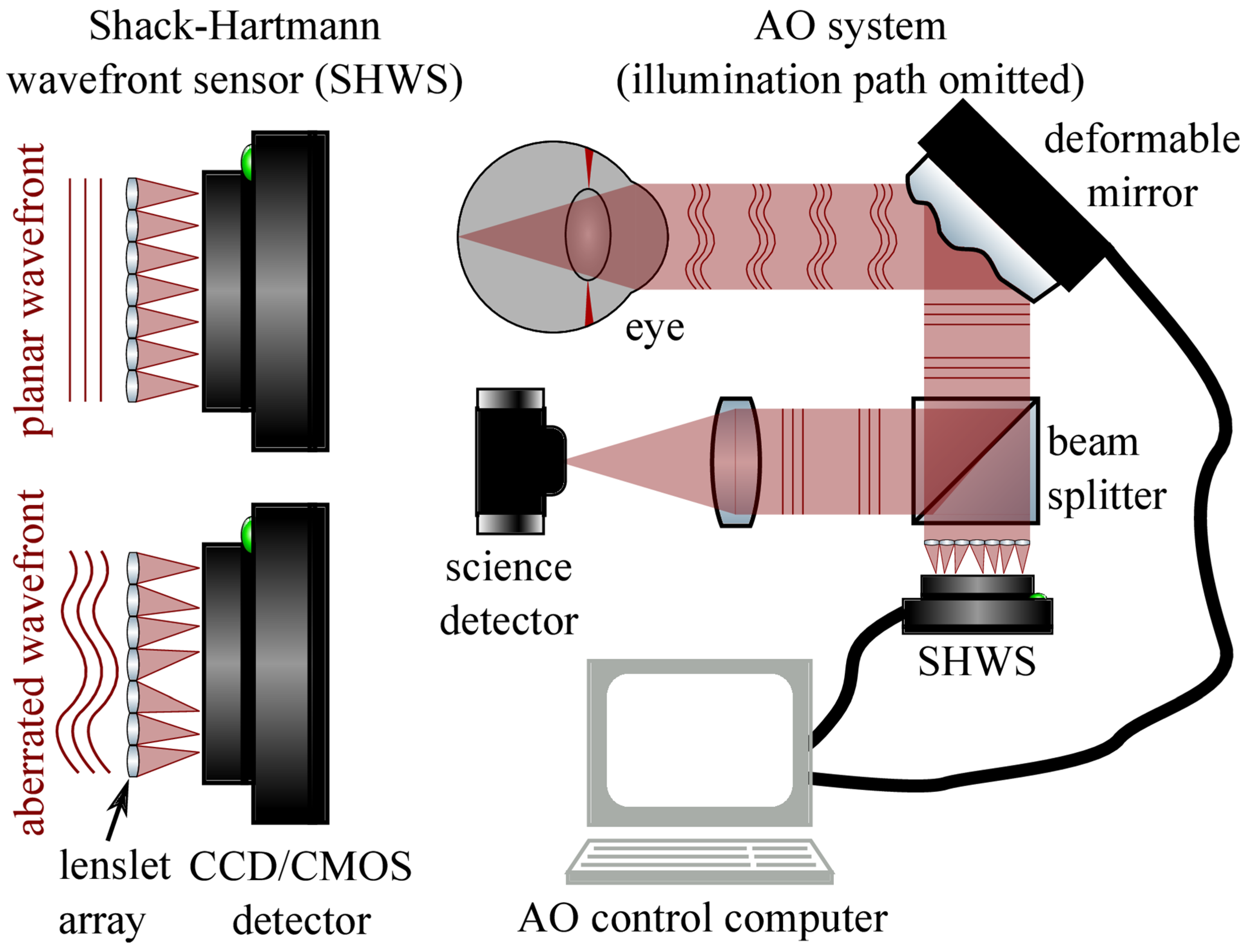
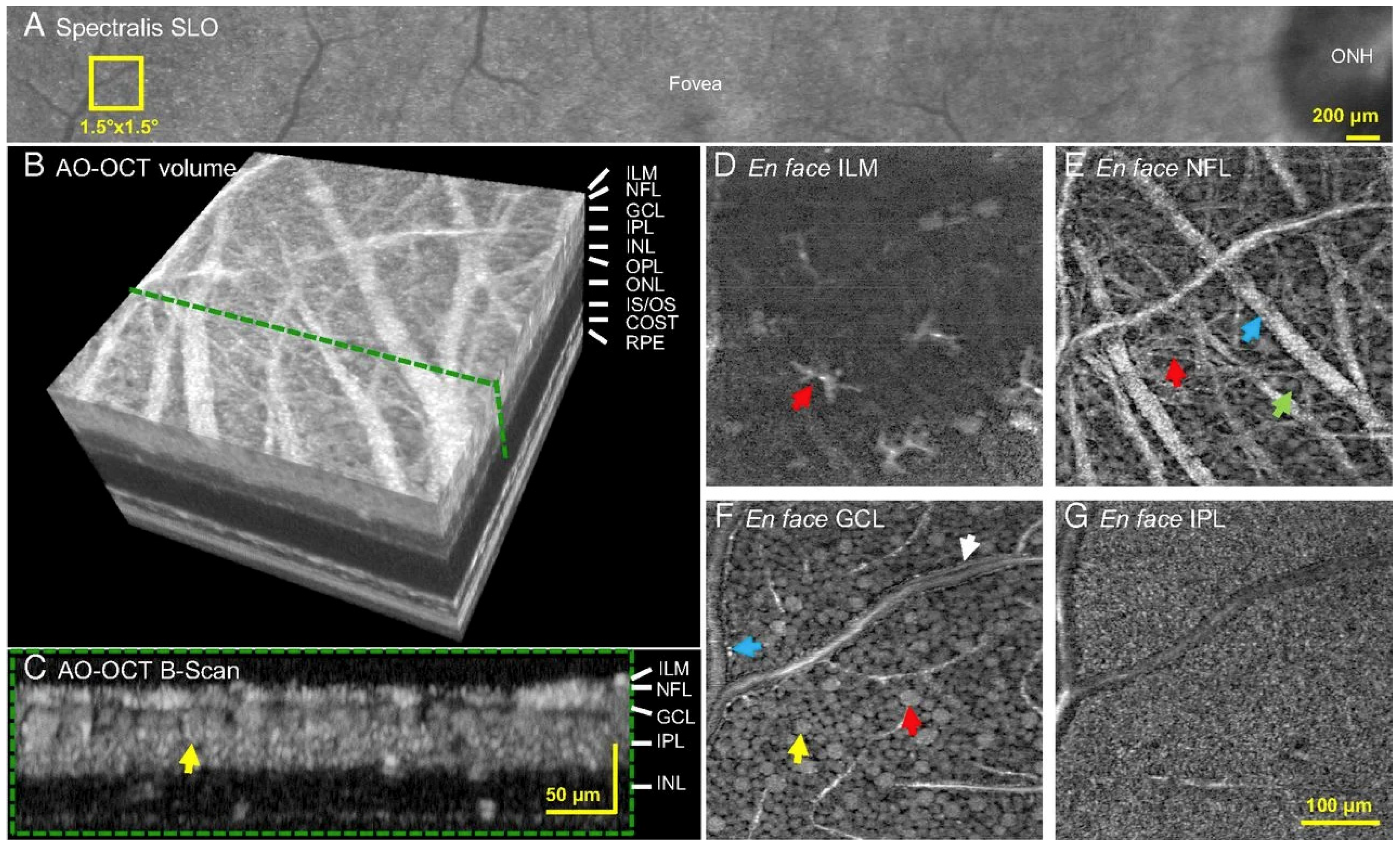
4. Adaptive Optics (AO) in OCT (AO-OCT)
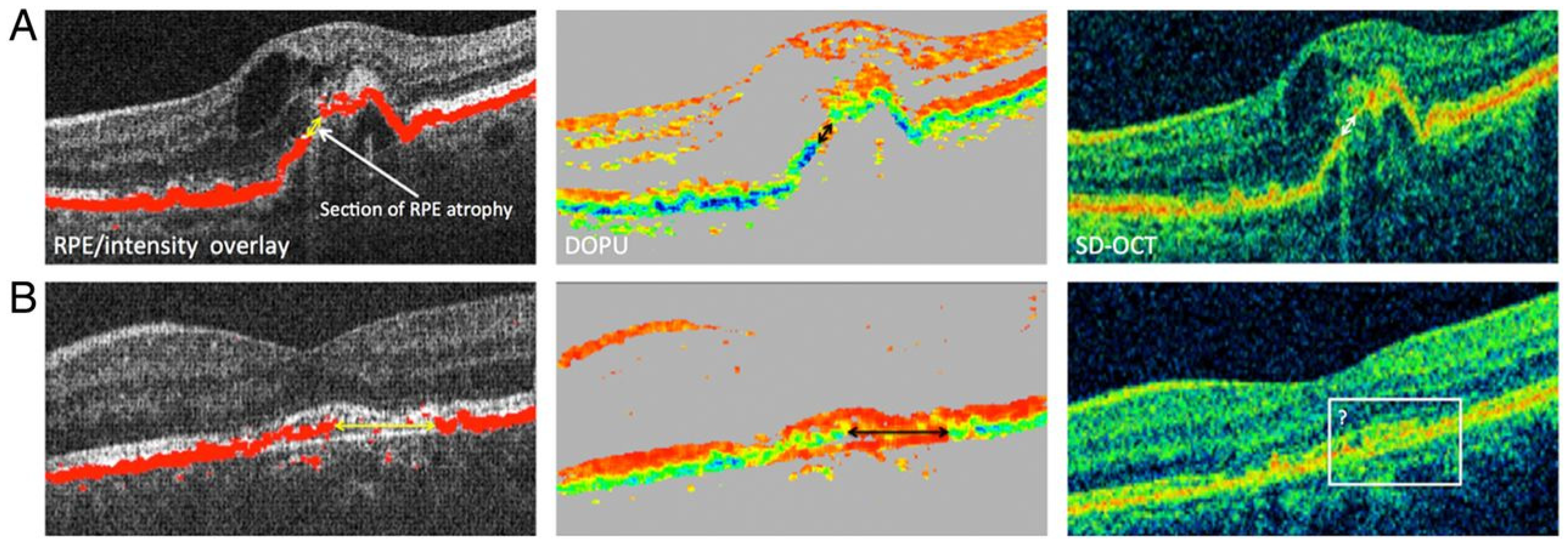
5. Polarization-Sensitive (PS) OCT
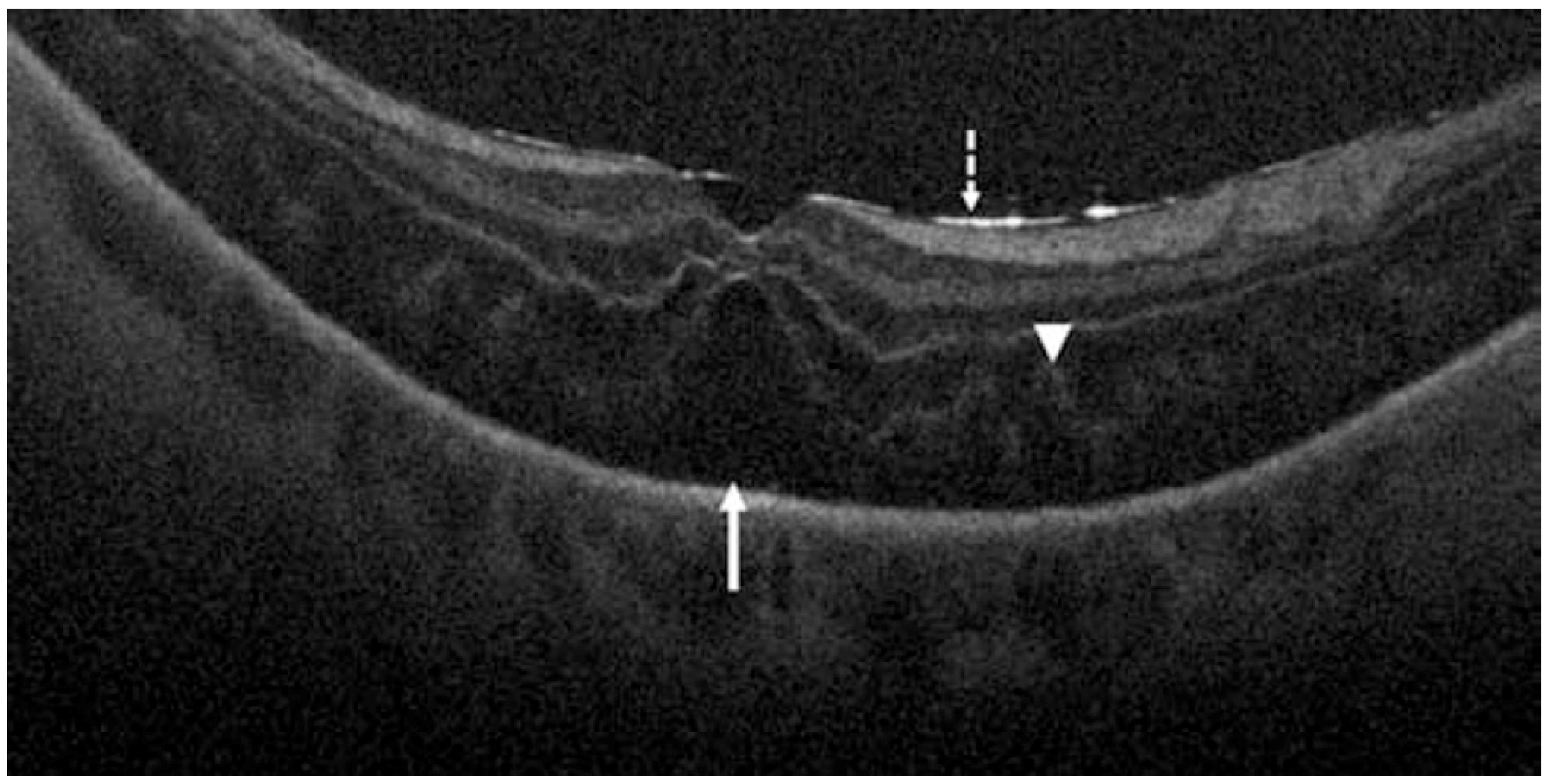
6. High-Resolution OCT (High-Res OCT)
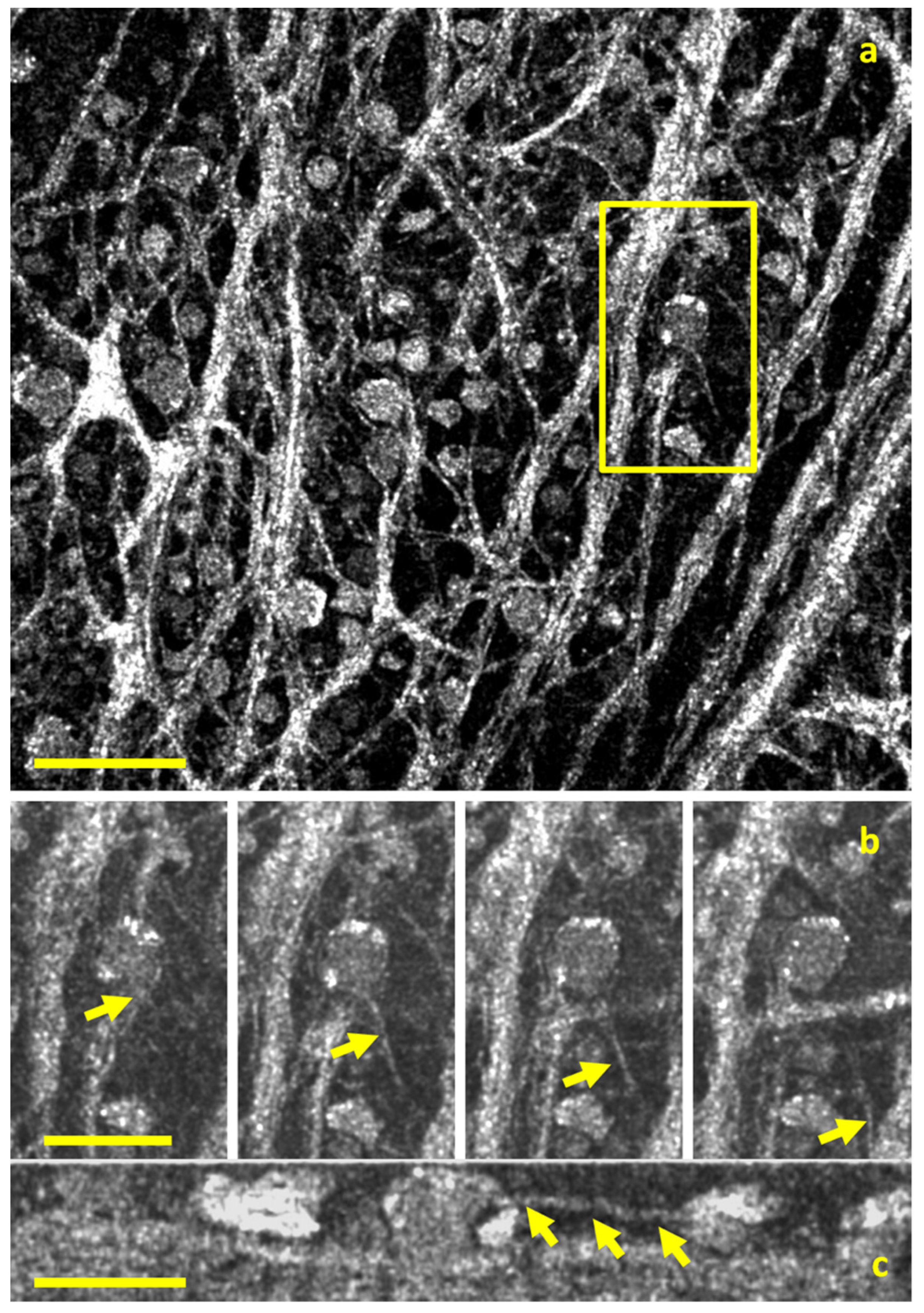
7. Full-Field OCT (FFOCT) and Dynamic FFOCT (D-FFOCT)
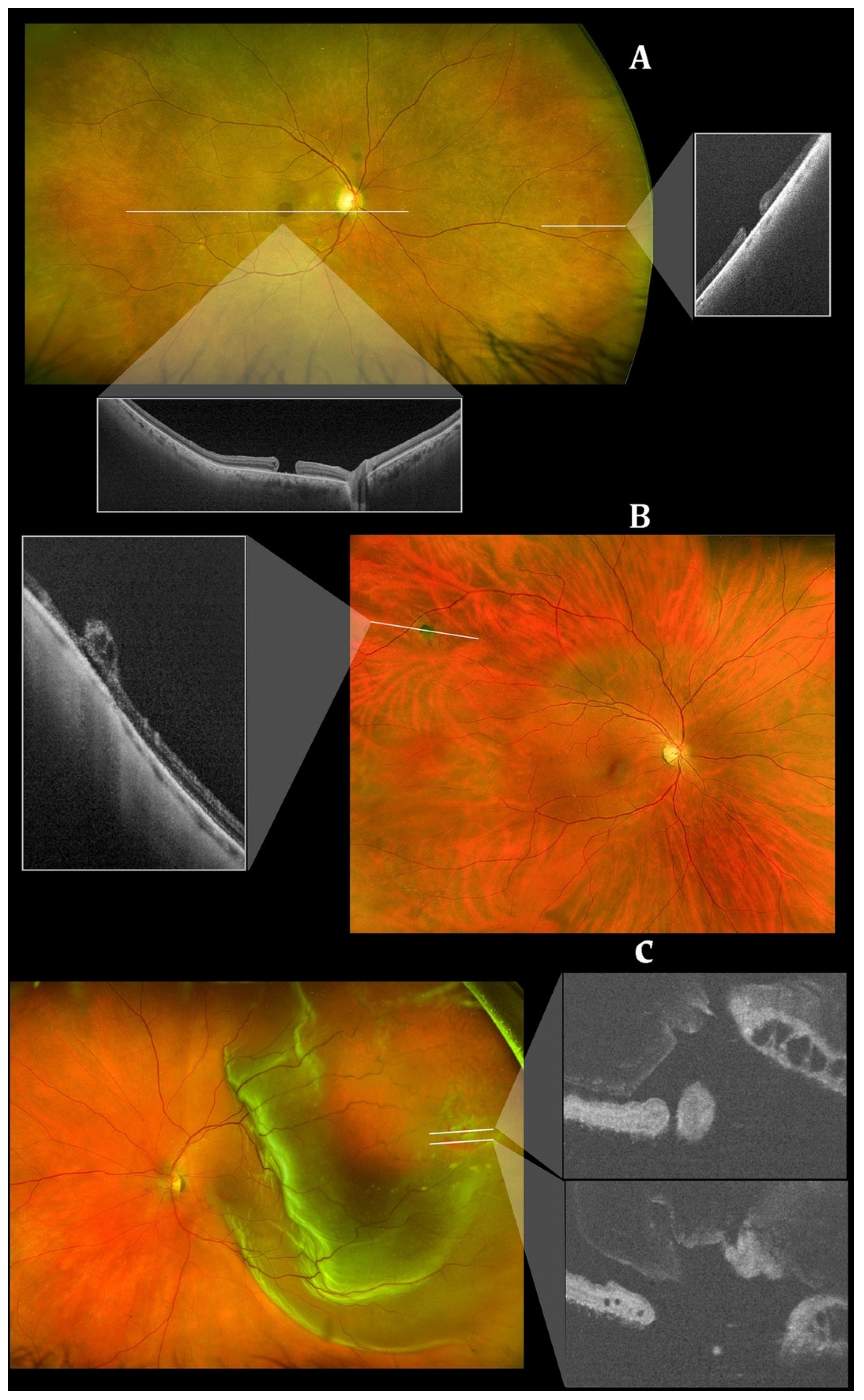
8. Wide-Field and Ultrawide-Field OCT (WF-OCT and UWF-OCT)
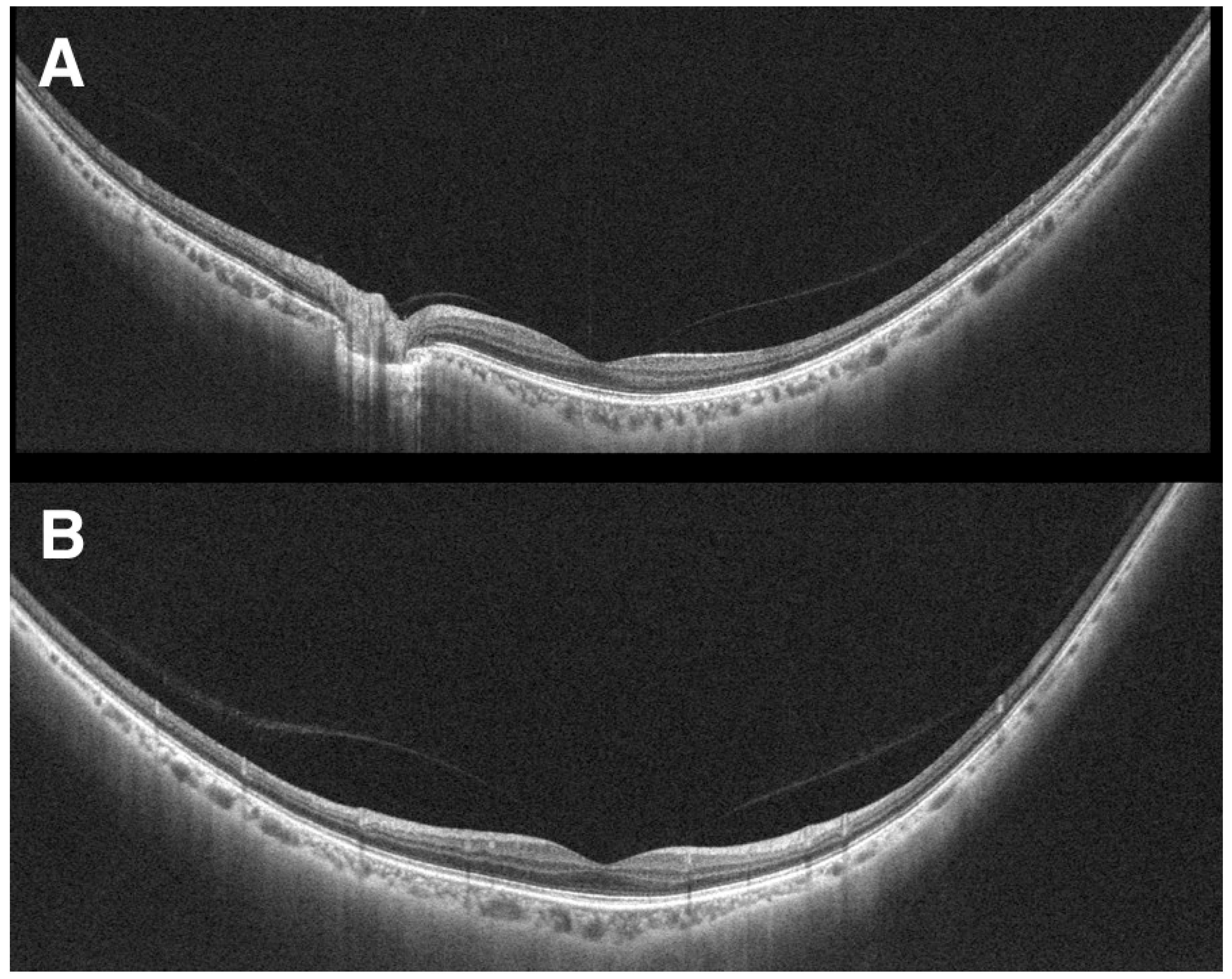
9. Hand-Held and Intraoperative OCT (iOCT)
10. At-Home OCT
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Stahl, A. The Diagnosis and Treatment of Age-Related Macular Degeneration. Dtsch Arztebl Int. 2020, 117, 513–520. [Google Scholar] [CrossRef]
- Semeraro, F.; Morescalchi, F.; Russo, A.; Gambicorti, E.; Pilotto, A.; Parmeggiani, F.; Bartollino, S.; Costagliola, C. Central Serous Chorioretinopathy: Pathogenesis and Management. Clin. Ophthalmol. 2019, 13, 2341–2352. [Google Scholar] [CrossRef]
- Boned-Murillo, A.; Albertos-Arranz, H.; Diaz-Barreda, M.D.; Orduna-Hospital, E.; Sánchez-Cano, A.; Ferreras, A.; Cuenca, N.; Pinilla, I. Optical Coherence Tomography Angiography in Diabetic Patients: A Systematic Review. Biomedicines 2021, 10, 88. [Google Scholar] [CrossRef]
- Majumdar, S.; Tripathy, K. Macular Hole. In StatPearls; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Metrangolo, C.; Donati, S.; Mazzola, M.; Fontanel, L.; Messina, W.; D’Alterio, G.; Rubino, M.; Radice, P.; Premi, E.; Azzolini, C. OCT Biomarkers in Neovascular Age-Related Macular Degeneration: A Narrative Review. J. Ophthalmol. 2021, 2021, 9994098. [Google Scholar] [CrossRef]
- Dhurandhar, D.S.; Singh, S.R.; Sahoo, N.K.; Goud, A.; Lupidi, M.; Chhablani, J. Identifying central serous chorioretinopathy biomarkers in coexisting diabetic retinopathy: A multimodal imaging study. Br. J. Ophthalmol. 2020, 104, 904–909. [Google Scholar] [CrossRef]
- Sahoo, N.K.; Ong, J.; Selvam, A.; Maltsev, D.; Sacconi, R.; Venkatesh, R.; Reddy, N.G.; Madan, S.; Tombolini, B.; Lima, L.H.; et al. Longitudinal follow-up and outcome analysis in central serous chorioretinopathy. Eye 2022, 1–7. [Google Scholar] [CrossRef]
- Corradetti, G.; Corvi, F.; Nittala, M.G.; Nassisi, M.; Alagorie, A.R.; Scharf, J.; Lee, M.Y.; Sadda, S.R.; Sarraf, D. Natural history of incomplete retinal pigment epithelial and outer retinal atrophy in age-related macular degeneration. Can. J. Ophthalmol. 2021, 56, 325–334. [Google Scholar] [CrossRef]
- Nassisi, M.; Fan, W.; Shi, Y.; Lei, J.; Borrelli, E.; Ip, M.; Sadda, S.R. Quantity of Intraretinal Hyperreflective Foci in Patients With Intermediate Age-Related Macular Degeneration Correlates With 1-Year Progression. Investig. Ophthalmol. Vis. Sci. 2018, 59, 3431–3439. [Google Scholar] [CrossRef]
- Lei, J.; Balasubramanian, S.; Abdelfattah, N.S.; Nittala, M.G.; Sadda, S.R. Proposal of a simple optical coherence tomography-based scoring system for progression of age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1551–1558. [Google Scholar] [CrossRef]
- Nassisi, M.; Lei, J.; Abdelfattah, N.S.; Karamat, A.; Balasubramanian, S.; Fan, W.; Uji, A.; Marion, K.M.; Baker, K.; Huang, X.; et al. OCT Risk Factors for Development of Late Age-Related Macular Degeneration in the Fellow Eyes of Patients Enrolled in the HARBOR Study. Ophthalmology 2019, 126, 1667–1674. [Google Scholar] [CrossRef]
- Gabriele, M.L.; Wollstein, G.; Ishikawa, H.; Kagemann, L.; Xu, J.; Folio, L.S.; Schuman, J.S. Optical coherence tomography: History, current status, and laboratory work. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2425–2436. [Google Scholar] [CrossRef]
- Aumann, S.; Donner, S.; Fischer, J.; Muller, F. Optical Coherence Tomography (OCT): Principle and Technical Realization. In High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics; Bille, J.F., Ed.; Springer Nature: Cham, Switzerland, 2019; pp. 59–85. [Google Scholar]
- Ohno-Matsui, K.; Fang, Y.; Morohoshi, K.; Jonas, J.B. Optical Coherence Tomographic Imaging of Posterior Episclera and Tenon’s Capsule. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3389–3394. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Shi, C.; Shen, M.; Lu, F. Advances in retina imaging as potential biomarkers for early diagnosis of Alzheimer’s disease. Transl. Neurodegener. 2021, 10, 6. [Google Scholar] [CrossRef]
- Povazay, B.; Bizheva, K.; Unterhuber, A.; Hermann, B.; Sattmann, H.; Fercher, A.F.; Drexler, W.; Apolonski, A.; Wadsworth, W.J.; Knight, J.C.; et al. Submicrometer axial resolution optical coherence tomography. Opt. Lett. 2002, 27, 1800–1802. [Google Scholar] [CrossRef]
- Zhang, T.; Kho, A.M.; Yiu, G.; Srinivasan, V.J. Visible Light Optical Coherence Tomography (OCT) Quantifies Subcellular Contributions to Outer Retinal Band 4. Transl. Vis. Sci. Technol. 2021, 10, 30. [Google Scholar] [CrossRef]
- Miller, D.T.; Kocaoglu, O.P.; Wang, Q.; Lee, S. Adaptive optics and the eye (super resolution OCT). Eye 2011, 25, 321–330. [Google Scholar] [CrossRef]
- Zawadzki, R.J.; Jones, S.M.; Olivier, S.S.; Zhao, M.; Bower, B.A.; Izatt, J.A.; Choi, S.; Laut, S.; Werner, J.S. Adaptive-optics optical coherence tomography for high-resolution and high-speed 3D retinal in vivo imaging. Opt. Express 2005, 13, 8532–8546. [Google Scholar] [CrossRef]
- Sayegh, R.G.; Zotter, S.; Roberts, P.K.; Kandula, M.M.; Sacu, S.; Kreil, D.P.; Baumann, B.; Pircher, M.; Hitzenberger, C.K.; Schmidt-Erfurth, U. Polarization-Sensitive Optical Coherence Tomography and Conventional Retinal Imaging Strategies in Assessing Foveal Integrity in Geographic Atrophy. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5246–5255. [Google Scholar] [CrossRef]
- De Boer, J.F.; Hitzenberger, C.K.; Yasuno, Y. Polarization sensitive optical coherence tomography—A review [Invited]. Biomed. Opt. Express 2017, 8, 1838–1873. [Google Scholar] [CrossRef] [Green Version]
- Imaging that Enlightens. Deeper insights into retinal structures with High-Resolution OCT. Ophthalmologist. 2020. Available online: https://theophthalmologist.com/subspecialties/imaging-that-enlightens (accessed on 1 August 2022).
- Spaide, R.F.; Lally, D.R. High Resolution Spectral Domain Optical Coherence Tomography of Multiple Evanescent White Dot Syndrome. Retin. Cases Brief Rep. 2021. [Google Scholar] [CrossRef]
- Grieve, K.; Thouvenin, O.; Sengupta, A.; Borderie, V.M.; Paques, M. Appearance of the Retina With Full-Field Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT96–OCT104. [Google Scholar] [CrossRef]
- Mece, P.; Scholler, J.; Groux, K.; Boccara, C. High-resolution in-vivo human retinal imaging using full-field OCT with optical stabilization of axial motion. Biomed. Opt. Express 2020, 11, 492–504. [Google Scholar] [CrossRef]
- Povazay, B.; Hermann, B.; Hofer, B.; Kajić, V.; Simpson, E.; Bridgford, T.; Drexler, W. Wide-field optical coherence tomography of the choroid in vivo. Investig. Ophthalmol. Vis. Sci. 2009, 50, 1856–1863. [Google Scholar] [CrossRef]
- Takahashi, H.; Tanaka, N.; Shinohara, K.; Yokoi, T.; Yoshida, T.; Uramoto, K.; Ohno-Matsui, K. Ultra-Widefield Optical Coherence Tomographic Imaging of Posterior Vitreous in Eyes With High Myopia. Am. J. Ophthalmol. 2019, 206, 102–112. [Google Scholar] [CrossRef]
- Ni, S.; Wei, X.; Ng, R.; Ostmo, S.; Chiang, M.F.; Huang, D.; Jia, Y.; Campbell, J.P.; Jian, Y. High-speed and widefield handheld swept-source OCT angiography with a VCSEL light source. Biomed. Opt. Express 2021, 12, 3553–3570. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Tao, Y.K.; Srivastava, S.K. The value of intraoperative optical coherence tomography imaging in vitreoretinal surgery. Curr. Opin. Ophthalmol. 2014, 25, 221–227. [Google Scholar] [CrossRef]
- Nahen, K.; Benyamini, G.; Loewenstein, A. Evaluation of a Self-Imaging SD-OCT System for Remote Monitoring of Patients with Neovascular Age Related Macular Degeneration. Klin. Mon. Für Augenheilkd. 2020, 237, 1410–1418. [Google Scholar] [CrossRef]
- Kim, J.E.; Tomkins-Netzer, O.; Elman, M.J.; Lally, D.R.; Goldstein, M.; Goldenberg, D.; Shulman, S.; Benyamini, G.; Loewenstein, A. Evaluation of a self-imaging SD-OCT system designed for remote home monitoring. BMC Ophthalmol. 2022, 22, 261. [Google Scholar] [CrossRef]
- Shu, X.; Beckmann, L.; Zhang, H. Visible-light optical coherence tomography: A review. J. Biomed Opt. 2017, 22, 1–14. [Google Scholar] [CrossRef]
- Yi, J.; Wei, Q.; Liu, W.; Backman, V.; Zhang, H.F. Visibl.le-light optical coherence tomography for retinal oximetry. Opt. Lett. 2013, 38, 1796–1798. [Google Scholar] [CrossRef]
- Yi, J.; Liu, W.; Chen, S.; Backman, V.; Sheibani, N.; Sorenson, C.M.; Fawzi, A.A.; Linsenmeier, R.A.; Zhang, H.F. Visible light optical coherence tomography measures retinal oxygen metabolic response to systemic oxygenation. Light Sci. Appl. 2015, 4, e334. [Google Scholar] [CrossRef]
- Rubinoff, I.; Miller, D.A.; Kuranov, R.; Wang, Y.; Fang, R.; Volpe, N.J.; Zhang, H.F. High-speed balanced-detection visible-light optical coherence tomography in the human retina using subpixel spectrometer calibration. IEEE Trans. Med. Imaging 2022. [Google Scholar] [CrossRef]
- Rubinoff, I.; Beckmann, L.; Wang, Y.; Fawzi, A.A.; Liu, X.; Tauber, J.; Jones, K.; Ishikawa, H.; Schuman, J.S.; Kuranov, R.; et al. Speckle reduction in visible-light optical coherence tomography using scan modulation. Neurophotonics 2019, 6, 041107. [Google Scholar] [CrossRef]
- Pi, S.; Hormel, T.T.; Wei, X.; Cepurna, W.; Morrison, J.C.; Jia, Y. Imaging retinal structures at cellular-level resolution by visible-light optical coherence tomography. Opt. Lett. 2020, 45, 2107–2110. [Google Scholar] [CrossRef]
- Zhang, T.; Kho, A.M.; Srinivasan, V.J. Morphometry of Inner Plexiform Layer (IPL) Stratification in the Human Retina With Visible Light Optical Coherence Tomography. Front. Cell Neuro Sci. 2021, 15, 655096. [Google Scholar] [CrossRef]
- Zhang, T.; Kho, A.M.; Srinivasan, V.J. Water wavenumber calibration for visible light optical coherence tomography. J. Biomed. Opt. 2020, 25, 090501. [Google Scholar] [CrossRef]
- Babcock, H.W. The possibility of compensating astronomical seeing. In Publications of the Astronomical Society of the Pacific, 386th ed.; The Astronomical Society of the Pacific: San Francisco, WI, USA, 1953; Volume 65, pp. 229–236. [Google Scholar]
- Liang, J.; Williams, D.R.; Miller, D.T. Supernormal vision and high-resolution retinal imaging through adaptive optics. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 1997, 14, 2884–2892. [Google Scholar] [CrossRef]
- Roorda, A.; Romero-Borja, F.; Donnelly Iii, W.; Queener, H.; Hebert, T.; Campbell, M. Adaptive optics scanning laser ophthalmoscopy. Opt. Express 2002, 10, 405–412. [Google Scholar] [CrossRef]
- Akyol, E.; Hagag, A.M.; Sivaprasad, S.; Lotery, A.J. Adaptive optics: Principles and applications in ophthalmology. Eye 2021, 35, 244–264. [Google Scholar] [CrossRef]
- Jonnal, R.S.; Kocaoglu, O.P.; Zawadzki, R.J.; Liu, Z.; Miller, D.T.; Werner, J.S. A Review of Adaptive Optics Optical Coherence Tomography: Technical Advances, Scientific Applications, and the Future. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT51-68. [Google Scholar] [CrossRef]
- Roorda, A.; Williams, D.R. The arrangement of the three cone classes in the living human eye. Nature 1999, 397, 520–522. [Google Scholar] [CrossRef]
- Kadomoto, S.; Muraoka, Y.; Uji, A.; Ooto, S.; Kawai, K.; Ishikura, M.; Nishigori, N.; Akagi, T.; Tsujikawa, A. Human Foveal Cone and Müller Cells Examined by Adaptive Optics Optical Coherence Tomography. Transl. Vis. Sci. Technol. 2021, 10, 17. [Google Scholar] [CrossRef]
- Fernández, E.; Drexler, W. Influence of ocular chromatic aberration and pupil size on transverse resolution in ophthalmic adaptive optics optical coherence tomography. Opt. Express 2005, 13, 8184–8197. [Google Scholar] [CrossRef]
- Shirazi, M.F.; Brunner, E.; Laslandes, M.; Pollreisz, A.; Hitzenberger, C.K.; Pircher, M. Visualizing human photoreceptor and retinal pigment epithelium cell mosaics in a single volume scan over an extended field of view with adaptive optics optical coherence tomography. Biomed. Opt. Express 2020, 11, 4520–4535. [Google Scholar] [CrossRef]
- Liu, Z.; Kurokawa, K.; Zhang, F.; Lee, J.J.; Miller, D.T. Imaging and quantifying ganglion cells and other transparent neurons in the living human retina. Proc. Natl. Acad. Sci. USA 2017, 114, 12803–12808. [Google Scholar] [CrossRef]
- Adie, S.G.; Graf, B.W.; Ahmad, A.; Carney, P.S.; Boppart, S.A. Computational adaptive optics for broadband optical interferometric tomography of biological tissue. Proc. Natl. Acad. Sci. USA 2012, 109, 7175–7180. [Google Scholar] [CrossRef]
- Ralston, T.S.; Marks, D.L.; Carney, P.S.; Boppart, S.A. Interferometric synthetic aperture microscopy. Nat. Phys. 2007, 3, 129–134. [Google Scholar] [CrossRef]
- Lee, B.; Lee, J.; Jeong, S.; Kang, W.; Oh, W.-Y. Video-rate computational adaptive optics optical coherence tomography with a stretched-pulse mode-locked laser. In European Conference on Biomedical Optics; Optical Society of America: Washington, DC, USA, 2021. [Google Scholar]
- Wang, J.; Chaney, E.J.; Aksamitiene, E.; Marjanovic, M.; Boppart, S.A. Computational adaptive optics for polarization-sensitive optical coherence tomography. Opt. Lett. 2021, 46, 2071–2074. [Google Scholar] [CrossRef]
- Ruiz-Lopera, S.; Restrepo, R.; Cuartas-Vélez, C.; Bouma, B.E.; Uribe-Patarroyo, N. Computational adaptive optics in phase-unstable optical coherence tomography. Opt. Lett. 2020, 45, 5982–5985. [Google Scholar] [CrossRef]
- Liu, L.; Wu, Z.; Qi, M.; Li, Y.; Zhang, M.; Liao, D.; Gao, P. Application of Adaptive Optics in Ophthalmology. Photonics 2022, 9, 288. [Google Scholar] [CrossRef]
- Camino, A.; Ng, R.; Huang, J.; Guo, Y.; Ni, S.; Jia, Y.; Huang, D.; Jian, Y. Depth-resolved optimization of a real-time sensorless adaptive optics optical coherence tomography. Opt. Lett. 2020, 45, 2612–2615. [Google Scholar] [CrossRef]
- Zhu, D.; Wang, R.; Žurauskas, M.; Pande, P.; Bi, J.; Yuan, Q.; Wang, L.; Gao, Z.; Boppart, S.A. Automated fast computational adaptive optics for optical coherence tomography based on a stochastic parallel gradient descent algorithm. Opt. Express 2020, 28, 23306–23319. [Google Scholar] [CrossRef]
- Hofer, H.; Sredar, N.; Queener, H.; Li, C.; Porter, J. Wavefront sensorless adaptive optics ophthalmoscopy in the human eye. Opt. Express 2011, 19, 14160–14171. [Google Scholar] [CrossRef]
- Durech, E.; Newberry, W.; Franke, J.; Sarunic, M.V. Wavefront sensor-less adaptive optics using deep reinforcement learning. Biomed. Opt. Express 2021, 12, 5423–5438. [Google Scholar] [CrossRef]
- Iyer, R.R.; Sorrells, J.E.; Yang, L.; Chaney, E.J.; Spillman, D.R.; Tibble, B.E.; Renteria, C.A.; Tu, H.; Žurauskas, M.; Marjanovic, M.; et al. Label-free metabolic and structural profiling of dynamic biological samples using multimodal optical microscopy with sensorless adaptive optics. Sci. Rep. 2022, 12, 3438. [Google Scholar] [CrossRef]
- Pircher, M.; Zawadzki, R.J. Review of adaptive optics OCT (AO-OCT): Principles and applications for retinal imaging [Invited]. Biomed. Opt. Express 2017, 8, 2536–2562. [Google Scholar] [CrossRef]
- Hee, M.R.; Huang, D.; Swanson, E.A.; Fujimoto, J.G. Polarization-sensitive low-coherence reflectometer for birefringence characterization and ranging. JOSA B 1992, 9, 903–908. [Google Scholar] [CrossRef]
- Pircher, M.; Hitzenberger, C.K.; Schmidt-Erfurth, U. Polarization sensitive optical coherence tomography in the human eye. Prog. Retin. Eye Res. 2011, 30, 431–451. [Google Scholar] [CrossRef]
- Ueno, Y.; Mori, H.; Kikuchi, K.; Yamanari, M.; Oshika, T. Visualization of Anterior Chamber Angle Structures With Scattering- and Polarization-Sensitive Anterior Segment Optical Coherence Tomography. Transl. Vis. Sci. Technol. 2021, 10, 29. [Google Scholar] [CrossRef]
- Baumann, B.; Gotzinger, E.; Pircher, M.; Sattmann, H.; Schuutze, C.; Schlanitz, F.; Ahlers, C.; Schmidt-Erfurth, U.; Hitzenberger, C.K. Segmentation and quantification of retinal lesions in age-related macular degeneration using polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2010, 15, 061704. [Google Scholar] [CrossRef]
- Sharma, S.; Hartl, G.; Naveed, S.K.; Blessing, K.; Sharma, G.; Singh, K. Input polarization-independent polarization-sensitive optical coherence tomography using a depolarizer. Rev. Sci. Instrum. 2020, 91, 043706. [Google Scholar] [CrossRef]
- Tang, P.; Wang, R. Stable fiber-based polarization-sensitive optical coherence tomography using polarization maintaining common-path interferometer. J. Biomed. Opt. 2020, 25, 116009. [Google Scholar] [CrossRef]
- Abouraddy, A.F.; Nasr, M.B.; Saleh, B.E.A.; Sergienko, A.V.; Teich, M.C. Quantum-Optical Coherence Tomography with Dispersion Cancellation; American Physical Society: College Park, MD, USA, 2002. [Google Scholar]
- Booth, M.C.; Di Giuseppe, G.; Saleh, B.E.A.; Sergienko, A.V.; Teich, M.C. Polarization-sensitive quantum-optical coherence tomography. Phys. Rev. A 2004, 69, 043815. [Google Scholar] [CrossRef]
- Sukharenko, V.; Bikorimana, S.; Dorsinville, R. Birefringence and scattering characterization using polarization sensitive quantum optical coherence tomography. Opt. Lett. 2021, 46, 2799–2802. [Google Scholar] [CrossRef]
- Schutze, C.; Teleky, K.; Baumann, B.; Pircher, M.; Gotzinger, E.; Hitzenberger, C.K.; Schmidt-Erfurth, U. Polarisation-sensitive OCT is useful for evaluating retinal pigment epithelial lesions in patients with neovascular AMD. Br. J. Ophthalmol. 2016, 100, 371–377. [Google Scholar] [CrossRef]
- Schranz, M.; Roberts, P.K.; Motschi, A.R.; Hollaus, M.; Mylonas, G.; Sacu, S.; Pircher, M.; Hitzenberger, C.K.; Schmidt-Erfurth, U. Tracking of fibrosis growth in neovascular age related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2022, 63, 1025–F0272. [Google Scholar]
- Lejoyeux, R.; Benillouche, J.; Ong, J.; Errera, M.H.; Rossi, E.A.; Singh, S.R.; Dansingani, K.K.; da Silva, S.; Sinha, D.; Sahel, J.A.; et al. Choriocapillaris: Fundamentals and advancements. Prog. Retin. Eye Res. 2022, 87, 100997. [Google Scholar] [CrossRef]
- Scholler, J.; Mazlin, V.; Thouvenin, O.; Groux, K.; Xiao, P.; Sahel, J.A.; Fink, M.; Boccara, C.; Grieve, K. Probing dynamic processes in the eye at multiple spatial and temporal scales with multimodal full field OCT. Biomed. Opt. Express 2019, 10, 731–746. [Google Scholar] [CrossRef]
- Apelian, C.; Harms, F.; Thouvenin, O.; Boccara, A.C. Dynamic full field optical coherence tomography: Subcellular metabolic contrast revealed in tissues by interferometric signals temporal analysis. Biomed. Opt. Express 2016, 7, 1511–1524. [Google Scholar] [CrossRef]
- Thouvenin, O.; Fink, M.; Boccara, C. Dynamic multimodal full-field optical coherence tomography and fluorescence structured illumination microscopy. J. Biomed. Opt. 2017, 22, 26004. [Google Scholar] [CrossRef]
- Singh, R.; Cuzzani, O.; Binette, F.; Sternberg, H.; West, M.D.; Nasonkin, I.O. Pluripotent Stem Cells for Retinal Tissue Engineering: Current Status and Future Prospects. Stem Cell Rev. Rep. 2018, 14, 463–483. [Google Scholar] [CrossRef]
- Ahmad, I.; Teotia, P.; Erickson, H.; Xia, X. Recapitulating developmental mechanisms for retinal regeneration. Prog. Retin. Eye Res. 2020, 76, 100824. [Google Scholar] [CrossRef]
- Wright, L.S.; Pinilla, I.; Saha, J.; Clermont, J.M.; Lien, J.S.; Borys, K.D.; Capowski, E.E.; Phillips, M.J.; Gamm, D.M. VSX2 and ASCL1 Are Indicators of Neurogenic Competence in Human Retinal Progenitor Cultures. PLoS ONE 2015, 10, e0135830. [Google Scholar] [CrossRef] [PubMed]
- Scholler, J.; Groux, K.; Goureau, O.; Sahel, J.A.; Fink, M.; Reichman, S.; Boccara, C.; Grieve, K. Dynamic full-field optical coherence tomography: 3D live-imaging of retinal organoids. Light Sci. Appl. 2020, 9, 140. [Google Scholar] [CrossRef] [PubMed]
- Groux, K.; Verschueren, A.; Nanteau, C.; Clémençon, M.; Fink, M.; Sahel, J.A.; Boccara, C.; Paques, M.; Reichman, S.; Grieve, K. Dynamic full-field optical coherence tomography allows live imaging of retinal pigment epithelium stress model. Commun. Biol. 2022, 5, 575. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Xu, J.; Wang, R.K. Long-range and wide field of view optical coherence tomography for in vivo 3D imaging of large volume object based on akinetic programmable swept source. Biomed. Opt. Express 2016, 7, 4734–4748. [Google Scholar] [CrossRef]
- Pomerantzeff, O. Equator-plus camera. Investig. Ophthalmol. 1975, 14, 401–406. [Google Scholar]
- Neubauer, A.S.; Yu, A.; Haritoglou, C.; Ulbig, M.W. Peripheral retinal changes in acute retinal necrosis imaged by ultra widefield scanning laser ophthalmoscopy. Acta Ophthalmol. Scand. 2005, 83, 758–760. [Google Scholar] [CrossRef]
- Choudhry, N.; Golding, J.; Manry, M.W.; Rao, R.C. Ultra-Widefield Steering-Based Spectral-Domain Optical Coherence Tomography Imaging of the Retinal Periphery. Ophthalmology 2016, 123, 1368–1374. [Google Scholar] [CrossRef]
- Everett, M.; Magazzeni, S.; Schmoll, T.; Kempe, M. Optical coherence tomography: From technology to applications in ophthalmology. Transl. Biophotonics 2021, 3, e202000012. [Google Scholar] [CrossRef]
- Klein, T.; Wieser, W.; Eigenwillig, C.M.; Biedermann, B.R.; Huber, R. Megahertz OCT for ultrawide-field retinal imaging with a 1050 nm Fourier domain mode-locked laser. Opt. Express 2011, 19, 3044–3062. [Google Scholar] [CrossRef] [PubMed]
- Gresores, N.J.; Singer, M.; Cairns, A.M.; Sinai, M.J.; Sadda, S.R. Evaluation of a Combined Ultra-wide Field SLO with SD OCT. Investig. Ophthalmol. 2018, 59, 664. [Google Scholar]
- NIDEK Co., L. NIDEK Launches the Mirante SLO Model. Available online: https://www.nidek-intl.com/news-event/news/entry-4046.html (accessed on 1 August 2022).
- NIDEK. Scanning Laser Ophthalmoscope Mirante SLO/OCT Mirante SLO; NIDEK: Gamagori, Japan, 2022. [Google Scholar]
- SPECTRALIS Inc., H.E. Available online: https://business-lounge.heidelbergengineering.com/us/en/products/spectralis/spectralis/ (accessed on 1 August 2022).
- Choudhry, N.; Sodhi, S. Peripheral OCT Imaging in Practice. Retina Today. 2021. Available online: https://retinatoday.com/articles/2021-apr/peripheral-oct-imaging-in-practice (accessed on 1 August 2022).
- Optos. Silverstone. Optos Products. 2022. Available online: https://www.Opt.os.com/products/silverstone/ (accessed on 1 August 2022).
- Optos. Monaco. Optos Products. 2022. Available online: https://www.Opt.os.com/products/Monaco/ (accessed on 1 August 2022).
- Sodhi, S.K.; Golding, J.; Trimboli, C.; Choudhry, N. Feasibility of peripheral OCT imaging using a novel integrated SLO ultra-widefield imaging swept-source OCT device. Int. Ophthalmol. 2021, 41, 2805–2815. [Google Scholar] [CrossRef] [PubMed]
- Uji, A.; Yoshimura, N. Application of extended field imaging to optical coherence tomography. Ophthalmology 2015, 122, 1272–1274. [Google Scholar] [CrossRef]
- Mishra, D.K.; Shanmugam, M.P.; Ramanjulu, R.; Sagar, P. Comparison of standard and "innovative wide-field" optical coherence tomography images in assessment of vitreoretinal interface in proliferative diabetic retinopathy: A pilot study. Indian J. Ophthalmol. 2021, 69, 99–102. [Google Scholar] [CrossRef]
- Mori, K.; Kanno, J.; Gehlbach, P.L. Retinochoroidal Morphology Described by Wide-Field Montage Imaging of Spectral Domain Optical Coherence Tomography. Retina 2016, 36, 375–384. [Google Scholar] [CrossRef]
- De Pretto, L.R.; Moult, E.M.; Alibhai, A.Y.; Carrasco-Zevallos, O.M.; Chen, S.; Lee, B.; Witkin, A.J.; Baumal, C.R.; Reichel, E.; de Freitas, A.Z.; et al. Controlling for Artifacts in Widefield Optical Coherence Tomography Angiography Measurements of Non-Perfusion Area. Sci. Rep. 2019, 9, 9096. [Google Scholar] [CrossRef]
- Ong, J.; Hariprasad, S.M.; Chhablani, J. A Guide to Accessible Artificial Intelligence and Machine Learning for the 21st Century Retina Specialist. Ophthalmic Surg. Lasers Imaging Retin. 2021, 52, 361–365. [Google Scholar] [CrossRef]
- Rakocz, N.; Chiang, J.N.; Nittala, M.G.; Corradetti, G.; Tiosano, L.; Velaga, S.; Thompson, M.; Hill, B.L.; Sankararaman, S.; Haines, J.L.; et al. Automated identification of clinical features from sparsely annotated 3-dimensional medical imaging. NPJ Digit. Med. 2021, 4, 44. [Google Scholar] [CrossRef]
- Zhang, G.; Fu, D.J.; Liefers, B.; Faes, L.; Glinton, S.; Wagner, S.; Struyven, R.; Pontikos, N.; Keane, P.A.; Balaskas, K. Clinically relevant deep learning for detection and quantification of geographic atrophy from optical coherence tomography: A model development and external validation study. Lancet Digit. Health 2021, 3, e665–e675. [Google Scholar] [CrossRef]
- Kolb, J.P.; Klein, T.; Kufner, C.L.; Wieser, W.; Neubauer, A.S.; Huber, R. Ultra-widefield retinal MHz-OCT imaging with up to 100 degrees viewing angle. Biomed. Opt. Express 2015, 6, 1534–1552. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Chu, K.K.; Kim, S.; Crose, M.; Cox, B.; Jelly, E.T.; Ulrich, J.N.; Wax, A. First Clinical Application of Low-Cost OCT. Transl. Vis. Sci. Technol. 2019, 8, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, W.; Kim, J.; Jeon, M.; Chaney, E.J.; Stewart, C.N.; Boppart, S.A. Handheld optical coherence tomography scanner for primary care diagnostics. IEEE Trans. Biomed. Eng. 2011, 58, 741–744. [Google Scholar] [CrossRef]
- Rufai, S.R. Handheld optical coherence tomography removes barriers to imaging the eyes of young children. Eye 2022, 36, 907–908. [Google Scholar] [CrossRef]
- Nicholson, R.; Osborne, D.; Fairhead, L.; Beed, L.; Hill, C.M.; Lee, H. Segmentation of the foveal and parafoveal retinal architecture using handheld spectral-domain optical coherence tomography in children with Down syndrome. Eye 2022, 36, 963–968. [Google Scholar] [CrossRef]
- Maldonado, R.S.; Izatt, J.A.; Sarin, N.; Wallace, D.K.; Freedman, S.; Cotten, C.M.; Toth, C.A. Optimizing hand-held spectral domain optical coherence tomography imaging for neonates, infants, and children. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2678–2685. [Google Scholar] [CrossRef]
- Malone, J.D.; El-Haddad, M.T.; Yerramreddy, S.S.; Oguz, I.; Tao, Y.K. Handheld spectrally encoded coherence tomography and reflectometry for motion-corrected ophthalmic optical coherence tomography and optical coherence tomography angiography. Neurophotonics 2019, 6, 041102. [Google Scholar] [CrossRef]
- Chopra, R.; Wagner, S.K.; Keane, P.A. Optical coherence tomography in the 2020s-outside the eye clinic. Eye 2021, 35, 236–243. [Google Scholar] [CrossRef]
- Wang, K.L.; Chen, X.; Stinnett, S.; Tai, V.; Winter, K.P.; Tran-Viet, D.; Toth, C.A. Understanding the variability of handheld spectral-domain optical coherence tomography measurements in supine infants. PLoS ONE 2019, 14, e0225960. [Google Scholar] [CrossRef]
- Kanyo, E.; Knapp, A.; Ehlers, J.P. The Emerging Role of Intraoperative OCT for Retinal Surgery. Retinal Phys. 2021. Available online: https://www.retinalphysician.com/issues/2021/november-december-2021/the-emerging-role-of-intraoperative-oct-for-retina (accessed on 1 August 2022).
- Dayani, P.N.; Maldonado, R.; Farsiu, S.; Toth, C.A. Intraoperative use of handheld spectral domain optical coherence tomography imaging in macular surgery. Retina 2009, 29, 1457–1468. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, J.P.; Dupps, W.J.; Kaiser, P.K.; Goshe, J.; Singh, R.P.; Petkovsek, D.; Srivastava, S.K. The Prospective Intraoperative and Perioperative Ophthalmic ImagiNg with Optical CoherEncE TomogRaphy (PIONEER) Study: 2-year results. Am. J. Ophthalmol. 2014, 158, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, J.P.; Modi, Y.S.; Pecen, P.E.; Goshe, J.; Dupps, W.J.; Rachitskaya, A.; Sharma, S.; Yuan, A.; Singh, R.; Kaiser, P.K.; et al. The DISCOVER Study 3-Year Results: Feasibility and Usefulness of Microscope-Integrated Intraoperative OCT during Ophthalmic Surgery. Ophthalmology 2018, 125, 1014–1027. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Uchida, A.; Srivastava, S.K. The Integrative Surgical Therater: Combining Intraoperative Optical Coherence Tomography and 3D Digital Visualization for Vitreoretinal Surgery in the DISCOVER Study. Retina 2018, 38 (Suppl. 1), S88–S96. [Google Scholar] [CrossRef] [PubMed]
- Ray, R.; Baranano, D.E.; Fortun, J.A.; Schwent, B.J.; Cribbs, B.E.; Bergstrom, C.S.; Hubbard, G.B., 3rd; Srivastava, S.K. Intraoperative microscope-mounted spectral domain optical coherence tomography for evaluation of retinal anatomy during macular surgery. Ophthalmology 2011, 118, 2212–2217. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Petkovsek, D.S.; Yuan, A.; Singh, R.P.; Srivastava, S.K. Intrasurgical assessment of subretinal tPA injection for submacular hemorrhage in the PIONEER study utilizing intraoperative OCT. Ophthalmic Surg. Lasers Imaging Retin. 2015, 46, 327–332. [Google Scholar] [CrossRef]
- Grewal, D.S.; Carrasco-Zevallos, O.M.; Gunther, R.; Izatt, J.A.; Toth, C.A.; Hahn, P. Intra-operative microscope-integrated swept-source optical coherence tomography guided placement of Argus II retinal prosthesis. Acta Ophthalmol. 2017, 95, e431–e432. [Google Scholar] [CrossRef]
- Liu, Y.; Holekamp, N.M.; Heier, J.S. Prospective, Longitudinal Study: Daily Self-Imaging with Home OCT for Neovascular Age-Related Macular Degeneration. Ophthalmol. Retin. 2022. [Google Scholar] [CrossRef]
- Chakravarthy, U.; Goldenberg, D.; Young, G.; Havilio, M.; Rafaeli, O.; Benyamini, G.; Loewenstein, A. Automated Identification of Lesion Activity in Neovascular Age-Related Macular Degeneration. Ophthalmology 2016, 123, 1731–1736. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Advances in OCT | Summary of Primary Advancement | References |
|---|---|---|
| Emerging Advances for Clinical Use | ||
| Visible-Light (Vis) OCT | Utilizes visible light illumination for OCT as opposed to commonly used near-infrared (NIR) light to capture fine details of the retina | [17,18] |
| Adaptive Optics (AO) OCT | Wavefront correcting component and computational controller software to compensate for aberrations and quality degradation, increasing the quality of OCT images. | [19,20] |
| Polarization Sensitive (PS) OCT | Measures and quantifies the polarization and depolarization of tissue for precision, high-quality imaging of retinal pigment epithelium layers | [21,22] |
| High-Resolution OCT (High-Res OCT) | Broadened bandwidth of the OCT light source to improve axial resolution and capture clearer details of the retinal microstructures and microvasculature. | [23,24] |
| Advances for Basic Science/Research | ||
| Full-Field (FF) and Dynamic Full-Field (DFF) OCT | Acquires images with charge coupled device cameras in 2D enface orientation at different depths for high resolution images at the cellular level. | [25,26] |
| Recent Advances in Available Technology | ||
| Wide-field (WF) and Ultrawide-field (UWF) OCT | Increased field of view to 40–55 degrees with wide-field OCT and up to 200 degrees with ultrawide-field OCT | [27,28] |
| Hand-Held and Intraoperative OCT (iOCT) | Hand-held OCT is portable OCT technology that is particularly useful for infants and bed ridden patients. Intraoperative OCT (microscope integrated) allows for image guidance and real-time feedback during ophthalmic surgery. | [29,30] |
| At-Home OCT | At-home, self-imaging OCT that allows for more frequent imaging and good agreement when compared to in-clinic OCT for more precise management of retinal diseases. | [31,32] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, J.; Zarnegar, A.; Corradetti, G.; Singh, S.R.; Chhablani, J. Advances in Optical Coherence Tomography Imaging Technology and Techniques for Choroidal and Retinal Disorders. J. Clin. Med. 2022, 11, 5139. https://doi.org/10.3390/jcm11175139
Ong J, Zarnegar A, Corradetti G, Singh SR, Chhablani J. Advances in Optical Coherence Tomography Imaging Technology and Techniques for Choroidal and Retinal Disorders. Journal of Clinical Medicine. 2022; 11(17):5139. https://doi.org/10.3390/jcm11175139
Chicago/Turabian StyleOng, Joshua, Arman Zarnegar, Giulia Corradetti, Sumit Randhir Singh, and Jay Chhablani. 2022. "Advances in Optical Coherence Tomography Imaging Technology and Techniques for Choroidal and Retinal Disorders" Journal of Clinical Medicine 11, no. 17: 5139. https://doi.org/10.3390/jcm11175139