
Potential Risk of Overtreatment in Patients with Type 2 Diabetes Aged 75 Years or Older: Data from a Population Database in Catalonia, Spain

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Eligibility Criteria
2.2. Study Variables
2.3. Statistical Methods
2.4. Ethics Committee Approval
3. Results
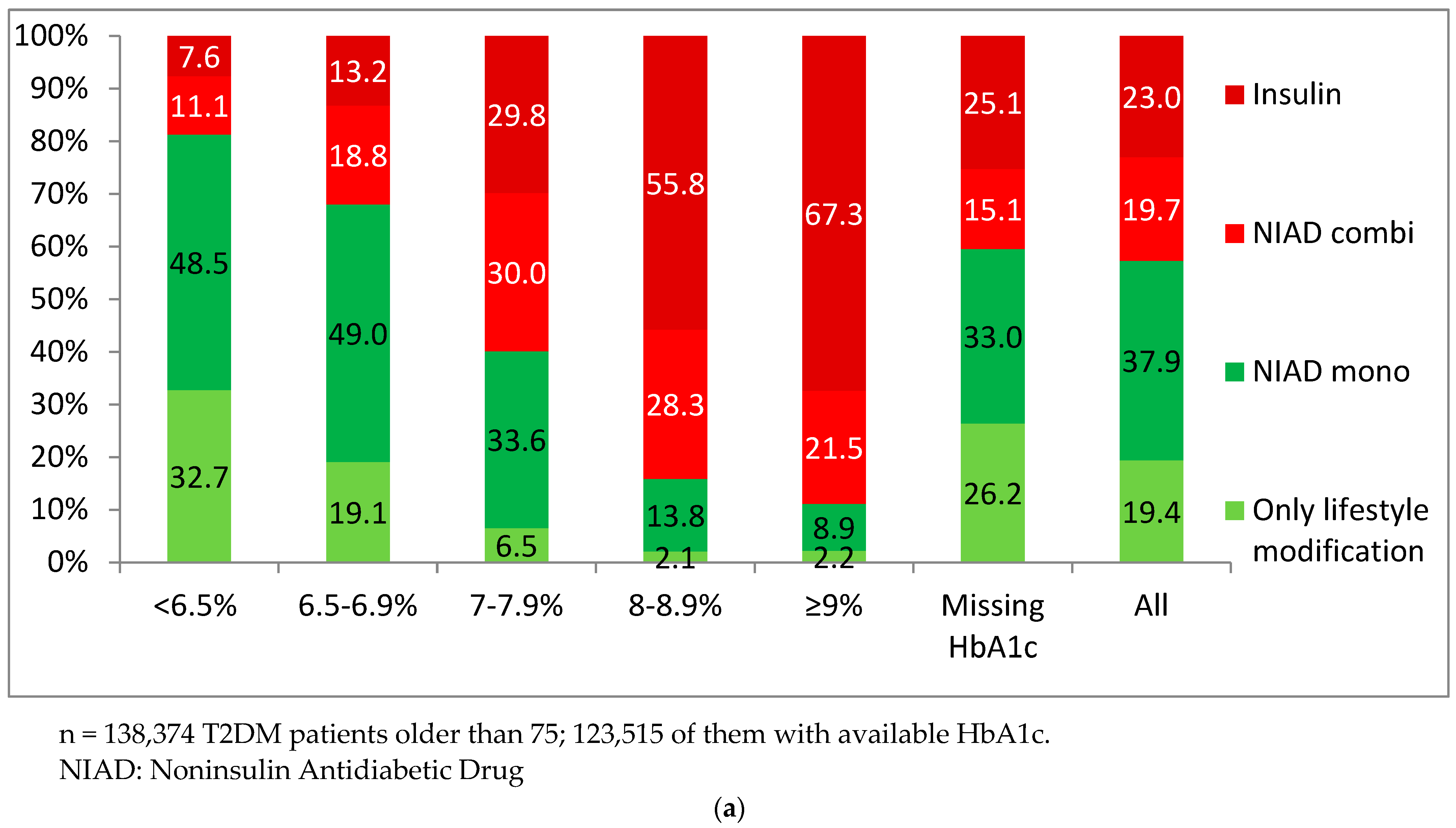
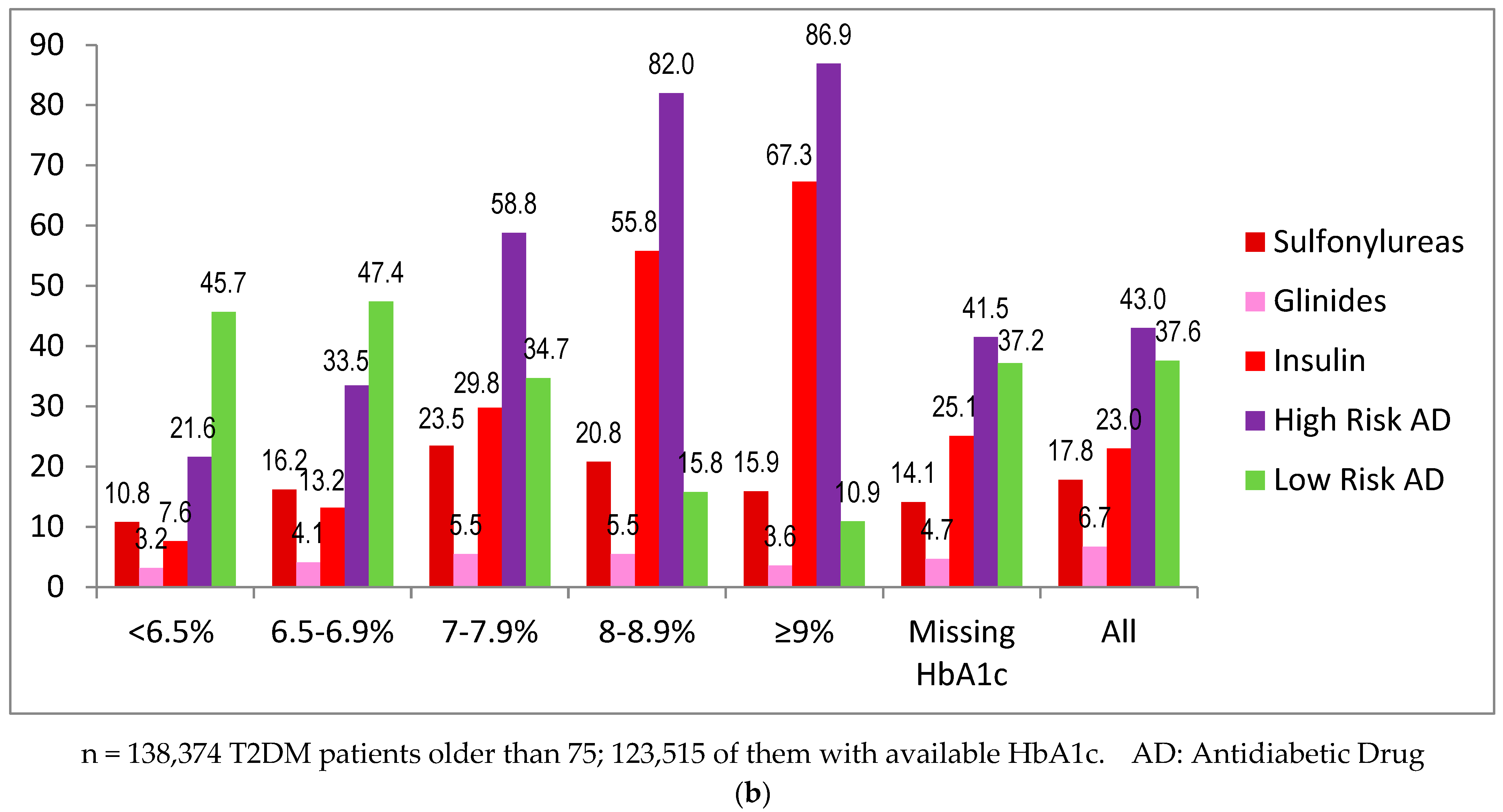
3.1. Antidiabetic Treatment
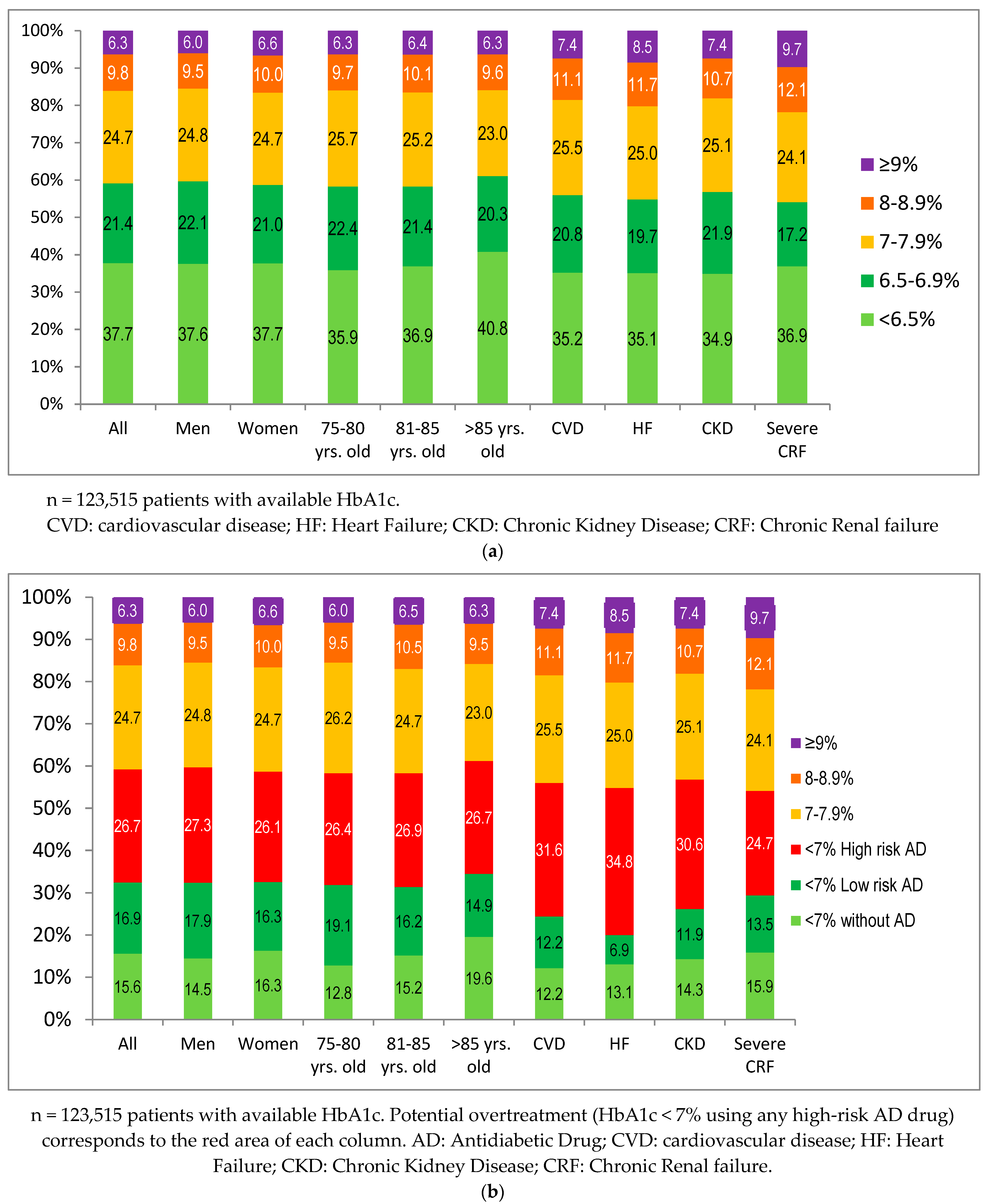
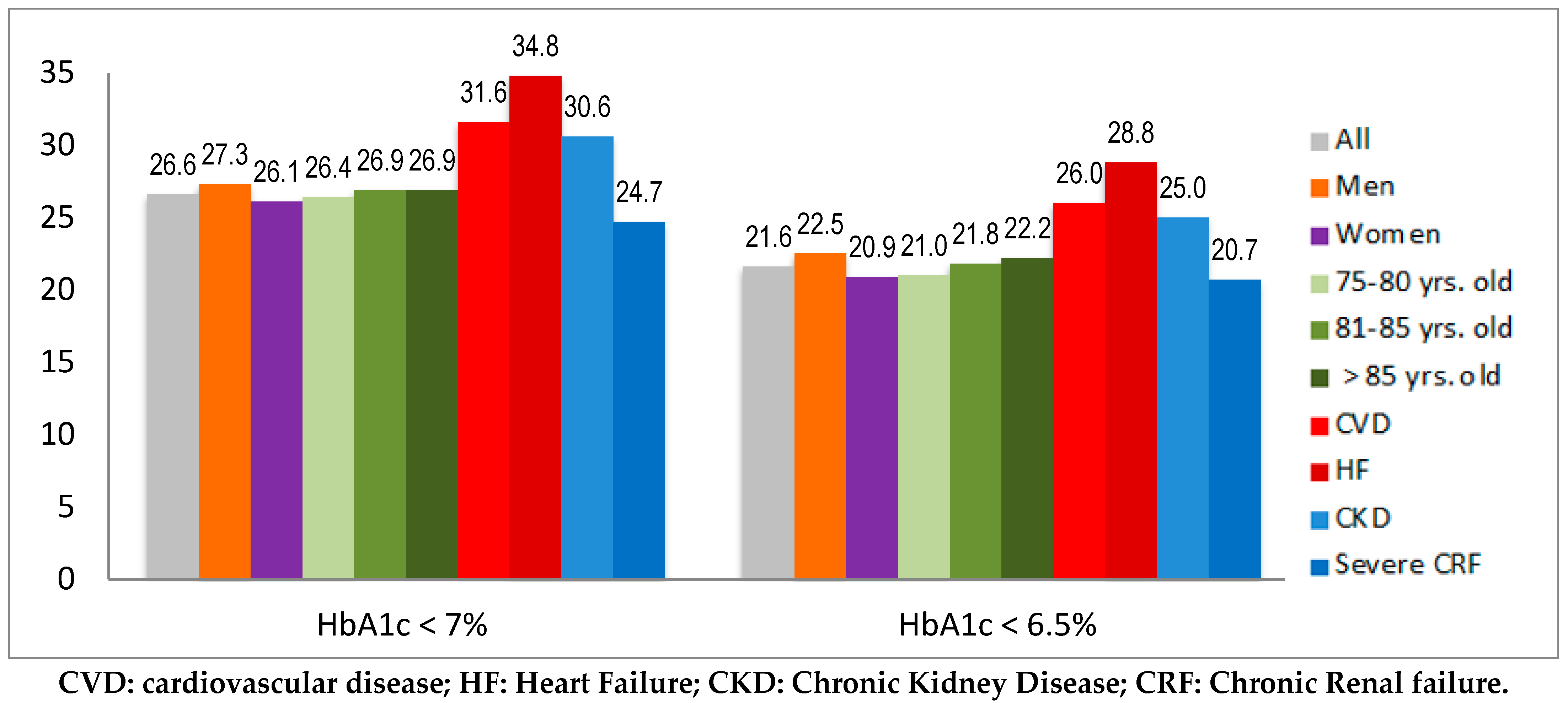
3.2. Potential Overtreatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; Available online: https://www.diabetesatlas.org (accessed on 9 May 2022).
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [PubMed]
- Mata Cases, M.; Artola Menéndez, S.; Díez Espino, J.; Ezkurra Loiola, P.; Franch Nadal, J.; García Soidán, F.J. Actualización de 2020 del algoritmo de tratamiento de la hiperglucemia en la diabetes mellitus tipo 2 de la RedGDPS. Diabetes Práct. 2020, 11, 41–76. [Google Scholar] [CrossRef]
- Seidu, S.; Cos, X.; Brunton, S.; Harris, S.; Jansson, S.; Mata-Cases, M.; Neijens, A.; Topsever, P.; Khunti, K. A Disease State Approach to the pharmacological management of Type 2 Diabetes in Primary Care: A Position Statement by Primary Care Diabetes Europe. Prim. Care Diabetes 2020, 15, 31–51. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 13 Older Adults: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S195–S207. [Google Scholar] [CrossRef] [PubMed]
- Strain, W.D.; Down, S.; Brown, P.; Puttanna, A.; Sinclair, A. Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes. Diabetes Ther. 2021, 12, 1227–1247. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.H.; Rodríguez-Mañas, L.; Morley, J.E.; Sinclair, A.J. Hypoglycemia in Older People—A Less Well Recognized Risk Factor for Frailty. Aging Dis. 2015, 6, 156. [Google Scholar] [CrossRef] [PubMed]
- Lipska, K.J.; Warton, E.M.; Huang, E.S.; Moffet, H.H.; Inzucchi, S.E.; Krumholz, H.M.; Karter, A.J. HbA1c and risk of severe hypoglycemia in type 2 diabetes: The Diabetes and Aging Study. Diabetes Care 2013, 36, 3535–3542. [Google Scholar] [CrossRef]
- Lipska, K.J.; Ross, J.S.; Wang, Y.; Inzucchi, S.E.; Minges, K.; Karter, A.J.; Huang, E.S.; Desai, M.; Gill, T. National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011. JAMA Intern. Med. 2014, 174, 1116–1124. [Google Scholar] [CrossRef]
- McCoy, R.G.; Lipska, K.J.; Yao, X.; Ross, J.S.; Montori, V.M.; Shah, N.D. Intensive Treatment and Severe Hypoglycemia among Adults with Type 2 Diabetes. JAMA Intern. Med. 2016, 176, 969–978. [Google Scholar] [CrossRef]
- Ling, S.; Zaccardi, F.; Lawson, C.; Seidu, S.I.; Davies, M.J.; Khunti, K. Glucose Control, Sulfonylureas, and Insulin Treatment in Elderly People with Type 2 Diabetes and Risk of Severe Hypoglycemia and Death: An Observational Study. Diabetes Care 2021, 44, 915–924. [Google Scholar] [CrossRef]
- Lipska, K.J.; Ross, J.S.; Miao, Y.; Shah, N.D.; Lee, S.J.; Steinman, M.A. Potential overtreatment of diabetes mellitus in older adults with tight glycemic control. JAMA Intern. Med. 2015, 175, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Al-Musawe, L.; Torre, C.; Guerreiro, J.P.; Rodrigues, A.T.; Raposo, J.F.; Mota-Filipe, H.; Martins, A.P. Overtreatment and undertreatment in a sample of elderly people with diabetes. Int. J. Clin. Pract. 2021, 75, e14847. [Google Scholar] [CrossRef] [PubMed]
- Sonmez, A.; Tasci, I.; Demirci, I.; Haymana, C.; Barcin, C.; Aydin, H.; Cetinkalp, S.; Ozturk, F.Y.; Gul, K.; Sabuncu, T.; et al. A Cross-Sectional Study of Overtreatment and Deintensification of Antidiabetic and Antihypertensive Medications in Diabetes Mellitus: The TEMD Overtreatment Study. Diabetes Ther. 2020, 11, 1045–1059. [Google Scholar] [CrossRef] [PubMed]
- Müller, N.; Khunti, K.; Kuss, O.; Lindblad, U.; Nolan, J.J.; Rutten, G.E.; Trento, M.; Porta, M.; Roth, J.; Charpentier, G.; et al. Is there evidence of potential overtreatment of glycaemia in elderly people with type 2 diabetes? Data from the GUIDANCE study. Acta Diabetol. 2017, 54, 209–214. [Google Scholar] [CrossRef]
- Hart, H.E.; Rutten, G.E.; Bontje, K.N.; Vos, R.C. Overtreatment of older patients with type 2 diabetes mellitus in primary care. Diabetes Obes. Metab. 2018, 20, 1066–1069. [Google Scholar] [CrossRef]
- Hambling, C.E.; Seidu, S.I.; Davies, M.J.; Khunti, K. Older people with Type 2 diabetes, including those with chronic kidney disease or dementia, are commonly overtreated with sulfonylurea or insulin therapies. Diabet. Med. 2017, 34, 1219–1227. [Google Scholar] [CrossRef]
- Arnold, S.V.; Lipska, K.J.; Wang, J.; Seman, L.; Mehta, S.N.; Kosiborod, M. Use of Intensive Glycemic Management in Older Adults with Diabetes Mellitus. J. Am. Geriatr. Soc. 2018, 66, 1190–1194. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Davies, M.J. Clinical inertia versus overtreatment in glycaemic management. Lancet Diabetes Endocrinol. 2018, 6, 266–268. [Google Scholar] [CrossRef]
- Aubert, C.E.; Lega, I.C.; Bourron, O.; Train, A.J.; Kullgren, J.T. When and how to deintensify type 2 diabetes care. BMJ 2021, 375, e066061. [Google Scholar] [CrossRef]
- Farrell, B.; Black, C.; Thompson, W.; McCarthy, L.; Rojas-Fernandez, C.; Lochnan, H.; Shamji, S.; Upshur, R.; Bouchard, M.; Welch, V. Deprescribing antihyperglycemic agents in older persons: Evidence-based clinical practice guideline. Can. Fam. Physician 2017, 63, 832–843. [Google Scholar] [PubMed]
- Makam, A.N.; Nguyen, O.K. An Evidence-Based Medicine Approach to Antihyperglycemic Therapy in Diabetes Mellitus to Overcome Overtreatment. Circulation 2017, 135, 180–195. [Google Scholar] [CrossRef] [PubMed]
- Seidu, S.; Kunutsor, S.K.; Topsever, P.; Hambling, C.E.; Cos, F.X.; Khunti, K. Deintensification in older patients with type 2 diabetes: A systematic review of approaches, rates and outcomes. Diabetes Obes. Metab. 2019, 21, 1668–1679. [Google Scholar] [CrossRef] [PubMed]
- Silverii, G.A.; Caldini, E.; Dicembrini, I.; Pieri, M.; Monami, M.; Mannucci, E. Deprescription in elderly patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2020, 170, 108498. [Google Scholar] [CrossRef] [PubMed]
- Sussman, J.B.; Kerr, E.A.; Saini, S.D.; Holleman, R.G.; Klamerus, M.L.; Min, L.C.; Vijan, S.; Hofer, T.P. Rates of Deintensification of Blood Pressure and Glycemic Medication Treatment Based on Levels of Control and Life Expectancy in Older Patients with Diabetes Mellitus. JAMA Intern. Med. 2015, 175, 1942–1949. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto-Honda, R.; Takahashi, Y.; Mori, Y.; Yamashita, S.; Yoshida, Y.; Kawazu, S.; Iwamoto, Y.; Kajio, H.; Yanai, H.; Mishima, S.; et al. Changes in Antidiabetic Drug Prescription and Glycemic Control Trends in Elderly Patients with Type 2 Diabetes Mellitus from 2005–2013: An Analysis of the National Center Diabetes Database (NCDD-03). Intern. Med. 2018, 57, 1229–1240. [Google Scholar] [CrossRef]
- Barrot-de la Puente, J.; Mata-Cases, M.; Franch-Nadal, J.; Mundet-Tudurí, X.; Casellas, A.; Fernandez-Real, J.M.; Mauricio, D. Older type 2 diabetic patients are more likely to achieve glycaemic and cardiovascular risk factors targets than younger patients: Analysis of a primary care database. Int. J. Clin. Pract. 2015, 69, 1486–1495. [Google Scholar] [CrossRef]
- Mata-Cases, M.; Vlacho, B.; Real, J.; Puig-Treserra, R.; Bundó, M.; Franch-Nadal, J.; Mauricio, D. Trends in the Degree of Control and Treatment of Cardiovascular Risk Factors in People with Type 2 Diabetes in a Primary Care Setting in Catalonia during 2007–2018. Front. Endocrinol. 2022, 12, 810757. [Google Scholar] [CrossRef]
- Mata-Cases, M.; Franch-Nadal, J.; Real, J.; Cedenilla, M.; Mauricio, D. Prevalence and coprevalence of chronic comorbid conditions in patients with type 2 diabetes in Catalonia: A population-based cross-sectional study. BMJ Open 2019, 9, e031281. [Google Scholar] [CrossRef]
- Mata-Cases, M.; Franch-Nadal, J.; Real, J.; Vlacho, B.; Gómez-García, A.; Mauricio, D. Evaluation of clinical and antidiabetic treatment characteristics of different sub-groups of patients with type 2 diabetes: Data from a Mediterranean population database. Prim. Care Diabetes 2021, 15, 588–595. [Google Scholar] [CrossRef]
- McCoy, R.G.; Lipska, K.J.; Van Houten, H.K.; Shah, N.D. Paradox of glycemic management: Multimorbidity, glycemic control, and high-risk medication use among adults with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001007. [Google Scholar] [CrossRef] [Green Version]
- DeCarlo, K.; Wallia, A.; Kang, R.H.; Cooper, A.; Cherupally, M.; Harris, S.A.; Aikman, C.; Liss, D.T.; Ackermann, R.T.; O’Brien, M.J. Initiating second-line antidiabetic medication among older adults with type 2 diabetes on Metformin. BMC Geriatr. 2022, 22, 97. [Google Scholar] [CrossRef] [PubMed]
- Overbeek, J.A.; Heintjes, E.M.; Prieto-Alhambra, D.; Blin, P.; Lassalle, R.; Hall, G.C.; Lapi, F.; Bianchini, E.; Hammar, N.; Bezemer, I.D.; et al. Type 2 Diabetes Mellitus Treatment Patterns Across Europe: A Population-based Multi-database Study. Clin. Ther. 2017, 39, 759–770. [Google Scholar] [CrossRef]
- Lipska, K.J.; Yao, X.; Herrin, J.; McCoy, R.G.; Ross, J.S.; Steinman, M.A.; Inzucchi, S.E.; Gill, T.M.; Krumholz, H.M.; Shah, N.D. Trends in Drug Utilization, Glycemic Control, and Rates of Severe Hypoglycemia, 2006–2013. Diabetes Care 2017, 40, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.M.; Henley, W.E.; McGovern, A.P.; Farmer, A.J.; Sattar, N.; Holman, R.R.; Pearson, E.R.; Hattersley, A.T.; Shields, B.M.; Jones, A.G.; et al. Time trends in prescribing of type 2 diabetes drugs, glycaemic response and risk factors: A retrospective analysis of primary care data, 2010–2017. Diabetes Obes. Metab. 2019, 21, 1576–1584. [Google Scholar] [CrossRef]
- Khunti, K.; Godec, T.R.; Medina, J.; Garcia-Alvarez, L.; Hiller, J.; Gomes, M.B.; Cid-Ruzafa, J.; Charbonnel, B.; Fenici, P.; Hammar, N.; et al. Patterns of glycaemic control in patients with type 2 diabetes mellitus initiating second-line therapy after metformin monotherapy: Retrospective data for 10,256 individuals from the United Kingdom and Germany. Diabetes. Obes. Metab. 2018, 20, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Nicolucci, A.; Charbonnel, B.; Gomes, M.B.; Khunti, K.; Kosiborod, M.; Shestakova, M.V.; Shimomura, I.; Watada, H.; Chen, H.; Cid-Ruzafa, J.; et al. Treatment patterns and associated factors in 14,668 people with type 2 diabetes initiating a second-line therapy: Results from the global DISCOVER study programme. Diabetes Obes. Metab. 2019, 21, 2474–2485. [Google Scholar] [CrossRef]
- Moreno-Juste, A.; Poblador-Plou, B.; Aza-Pascual-Salcedo, M.; González-Rubio, F.; Malo, S.; Librero López, J.; Pico-Soler, V.; Labrador, E.G.; Mucherino, S.; Orlando, V.; et al. Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data. Int. J. Environ. Res. Public Health 2020, 17, 3742. [Google Scholar] [CrossRef]
- Nunes, A.P.; Yang, J.; Radican, L.; Engel, S.S.; Kurtyka, K.; Tunceli, K.; Yu, S.; Iglay, K.; Doherty, M.C.; Dore, D.D. Assessing occurrence of hypoglycemia and its severity from electronic health records of patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2016, 121, 192–203. [Google Scholar] [CrossRef]
- Uzoigwe, C.; Hamersky, C.M.; Arbit, D.I.; Weng, W.; Radin, M.S. Assessing Prevalence of Hypoglycemia in a Medical Transcription Database. Diabetes Metab. Syndr. Obes. 2020, 13, 2209–2216. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall n = 138,374 | Men n = 61,449 | Women n = 76,925 | 75–80 Years Old n = 48,951 | 81–85 Years Old n = 47,278 | >85 Years Old n = 42,145 | CVD n = 44,668 | HF n = 17,986 | CKD n = 71,848 | Severe CRF n = 5272 |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean age, years (SD) | 82.6 (5.1) | 81.9 (4.8) | 83.2 (5.3) | 77.5 (1.5) | 82.9 (1.1) | 88.9 (3.1) | 83.1 (5.1) | 84.2 (5.3) | 83.5 (5.2) | 84.7 (5.4) |
| Gender (female), % | 55.6 | 0 | 100 | 49.2 | 55.1 | 63.5 | 44.3 | 59.6 | 57.1 | 59.8 |
| Mean diabetes duration, years (SD) | 11.2 (6.8) | 11.1 (6.6) | 11.3 (7.0) | 10.7 (6.4) | 11.4 (6.8) | 11.7 (7.1) | 12.0 (7.1) | 11.7 (7.1) | 11.8 (6.9) | 12.9 (7.2) |
| Mean HbA1c, % (SD) (n = 123,515) | 7.0 (1.1) | 7.0 (1.1) | 7.0 (1.1) | 7.0 (1.1) | 7.0 (1.1) | 7.0 (1.1) | 7.1 (1.1) | 7.1 (1.2) | 7.1 (1.1) | 7.1 (1.2) |
| Current smoker, % | 4.8 | 9.1 | 1.3 | 6.9 | 4.5 | 2.6 | 5.6 | 3.3 | 4.5 | 3.7 |
| Mean BMI, kg/m2 (SD) (n = 117,212) | 28.9 (3.9) | 28.2 (3.9) | 29.5 (5.2) | 29.6 (4.8) | 28.9(4.7) | 27.9 (4.5) | 28.5 (4.5) | 30.0 (5.4) | 29.1 (4.8) | 29.4 (5.2) |
| Obesity (BMI > 30 kg/m2), % (n = 117,212) | 36.1 | 29.2 | 41.9 | 41.1 | 36.7 | 28.5 | 33.0 | 16.9 | 37.9 | 41.2 |
| Hypertension, % | 84.4 | 80.3 | 87.7 | 82.5 | 84.9 | 86.1 | 85.9 | 89.2 | 89.5 | 91.6 |
| Hyperlipidemia, % | 60.4 | 56.3 | 63.7 | 63.8 | 61.1 | 55.7 | 63.0 | 60.4 | 61.8 | 60.9 |
| CVD, % | 32.3 | 40.5 | 25.7 | 29.2 | 32.6 | 35.6 | - | 49.4 | 37.1 | 45.3 |
| HF, % | 13.0 | 11.8 | 13.9 | 8.9 | 12.6 | 18.2 | 19.9 | - | 17.8 | 33.2 |
| Retinopathy, % | 15.8 | 15.0 | 16.4 | 15.4 | 16.2 | 15.8 | 18.8 | 19.6 | 17.8 | 22.1 |
| Neuropathy, % | 10.0 | 8.4 | 11.3 | 10.5 | 10.45 | 8.8 | 11.4 | 11.8 | 10.8 | 9.0 |
| CKD (eGFR < 60 mL/min/1.73 m2 or albuminuria > 30 mg/g), % | 51.9 | 50.2 | 53.3 | 42.1 | 53.8 | 62.5 | 59.7 | 71.1 | - | - |
| Severe chronic renal failure (eGFR < 30 mL/min/1.73 m2), % (n = 124,748) | 7.6 | 7.0 | 8.2 | 4.6 | 7.1 | 11.8 | 10.7 | 19.3 | - | - |
| Antidiabetic Treatment | ||||||||||
| Only lifestyle modification, % | 19.4 | 18.0 | 20.6 | 15.6 | 18.5 | 25.0 | 17.0 | 18.9 | 17.9 | 20.1 |
| Non-insulin antidiabetic drug monotherapy, % | 37.9 | 38.6 | 37.4 | 38.4 | 37.8 | 37.5 | 34.3 | 31.8 | 35.2 | 25.7 |
| Non-insulin antidiabetic drug combination, % | 19.7 | 21.7 | 18.0 | 23.1 | 20.0 | 15.3 | 18 | 13.7 | 18.6 | 7.8 |
| Insulin (alone or in combination), % | 23.0 | 21.7 | 24.0 | 22.9 | 23.7 | 22.3 | 30.6 | 35.7 | 28.3 | 46.5 |
| Sulfonylureas, % | 17.8 | 18.8 | 17.8 | 19.9 | 17.8 | 15.3 | 16.4 | 13.8 | 16.9 | 17.2 |
| Glinides, % | 6.7 | 6.8 | 6.6 | 6.0 | 6.9 | 7.4 | 7.6 | 8.9 | 8.6 | 4.6 |
| High-risk antidiabetics, % | 43.5 | 43.3 | 43.6 | 44.5 | 44.1 | 41.6 | 49.8 | 53.1 | 49.0 | 66.0 |
| Only low-risk antidiabetics, % | 37.6 | 38.7 | 35.8 | 39.9 | 37.4 | 33.4 | 33.2 | 28.0 | 33.1 | 13.1 |
| Overall n = 138,374 | CVD n = 39,928 | HF n = 17,986 | CKD n = 71,848 | Severe CRF (eGFR < 30 mL/min) n = 5272 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 75–80 yrs. n = 17,504 | 81–85 yrs. n = 15,766 | >85 yrs. n = 12,398 | 75–80 yrs. n = 5506 | 81–85 yrs. n = 5994 | >85 yrs. n = 6486 | 75–80 yrs. n = 25,716 | 81–85 yrs. n = 24,219 | >85 yrs. n = 21,193 | 75–80 yrs. n = 1379 | 81–85 yrs. n = 1703 | >85 yrs. n = 2190 | ||
| Only lifestyle modification, % | 19.4 | 13.1 | 15.8 | 24.1 | 13.0 | 17.3 | 25.3 | 13.4 | 17.0 | 24.1 | 14.0 | 17.4 | 27.9 |
| Non-insulin antidiabetic drug monotherapy, % | 37.9 | 33.6 | 34.6 | 35.1 | 30.4 | 31.6 | 33.1 | 34.2 | 35.2 | 36.3 | 20.6 | 21.0 | 25.1 |
| Non-insulin antidiabetic drug combination, % | 19.7 | 21.0 | 18.0 | 13.9 | 16.0 | 14.3 | 11.1 | 22.2 | 18.7 | 14.4 | 5.6 | 4.6 | 5.6 |
| Insulin (alone or in combination), % | 23.0 | 32.3 | 31.6 | 26.9 | 30.6 | 33.3 | 36.1 | 30.2 | 29.0 | 25.2 | 59.8 | 57.0 | 41.5 |
| Sulfonylureas, % | 17.8 | 18.3 | 15.9 | 14.3 | 15.3 | 13.9 | 12.3 | 18.8 | 16.8 | 14.7 | 2.8 | 4.1 | 6.3 |
| Glinides, % | 6.7 | 6.9 | 7.8 | 8.2 | 8.1 | 9.0 | 9.4 | 8.0 | 8.8 | 9.1 | 17.0 | 18.6 | 16.3 |
| Any high-risk antidiabetic drug, % | 43.5 | 52.3 | 50.4 | 45.5 | 57.9 | 54.2 | 47.9 | 51.8 | 49.6 | 45.0 | 72.2 | 71.1 | 58.2 |
| Any low-risk antidiabetic drug, % | 37.6 | 34.6 | 33.8 | 31.3 | 29.1 | 28.5 | 26.8 | 34.8 | 33.4 | 30.9 | 13.8 | 11.5 | 13.9 |
| Overall | Women | Men | 75–80 yrs. | 81–85 yrs. | >85 yrs. | HbA1c < 6.5% | HbA1c 6.5–6.9% | HbA1c 7–7.9% | HbA1c 8–8.9% | HbA1c ≥ 9% | Missing HbA1c | eGFR > 60 mL/min | eGFR 30–59 mL/min | eGFR < 30 mL/min | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 13,8374 | n = 76,925 | n = 61,449 | n = 59,440 | n = 44,314 | n = 34,620 | n = 46,554 | n = 21,705 | n = 31,262 | n = 12,713 | n = 6858 | n = 19,282 | n = 74,817 | n = 43,292 | n = 5138 | |
| All patients, n (%) | 1596 (1.2) | 958 (1.2) | 638 (1.0) | 466 (1.0) | 424 (1.2) | 589 (1.4) | 301 (0.6) | 178 (0.8) | 446 (1.4) | 321 (2.5) | 186 (2.7) | 164 (0.9) | 682 (0.9) | 685 (1.6) | 134 (2.5) |
| Sulfonylurea, n (%) | 150 (0.6) | 90 (0.7) | 60 (0.5) | 53 (0.5) | 38 (0.6) | 49 (0.8) | 43 (0.8) | 24 (0.7) | 38 (0.5) | 21 (0.6) | 9 (0.6) | 15 (0.5) | 89 (0.6) | 51 (0.7) | 2 (0.8) |
| Glinides, n (%) | 139 (1.5) | 82 (1.6) | 57 (1.4) | 27 (0.9) | 41 (1.6) | 63 (2.0) | 19 (1.1) | 14 (1.3) | 42 (1.6) | 37 (2.3) | 15 (1.8) | 12 (0.9) | 44 (1.3) | 66 (1.6) | 20 (2.2) |
| Insulin, n (%) | 1168 (3.7) | 720 (3.9) | 448 (3.4) | 350 (3.1) | 312 (3.6) | 414 (4.4) | 132 (3.7) | 110 (3.9) | 350 (3.8) | 289 (4.1) | 178 (3.9) | 109 (2.5) | 481 (3.5) | 515 (3.9) | 106 (4.2) |
| Any high-risk AD, n (%) | 1343 (2.2) | 820 (2.4) | 523 (2.0) | 405 (1.9) | 360 (2.2) | 478 (2.7) | 192 (1.9) | 140 (1.9) | 397 (2.2) | 310 (3.0) | 182 (3.1) | 122 (1.5) | 569 (1.9) | 581 (2.7) | 120 (3.4) |
| Only low risk AD, n (%) | 253 (0.3) | 138 (0.3) | 115 (0.3) | 61 (0.2) | 64 (0.3) | 111 (0.5) | 109 (0.3) | 38 (0.3) | 49 (0.4) | 11 (0.5) | 4 (0.4) | 42 (0.4) | 113 (0.2) | 104 (0.5) | 14 (0.8) |
| Lifestyle modification, n (%) | 80 (0.3) | 51 (0.3) | 29 (0.3) | 11 (0.1) | 25 0.4) | 40 (0.4) | 42 (0.3) | 10 (0.2) | 6 (0.3) | 4 (1.5) | 0 (0.0) | 18 (0.4) | 26 (0.2) | 33 (0.4) | 9 (0.8) |
| NIAD monotherapy, n (%) | 198 (0.4) | 105 (0.4) | 93 (0.4) | 53 (0.3) | 46 (0.3) | 88 (0.6) | 93 (0.4) | 33 (0.3) | 36 (0.3) | 8 (0.5) | 2 (0.3) | 26 (0.4) | 92 (0.3) | 77 (0.5) | 16 (1.3) |
| NIAD combination, n (%) | 150 (0.6) | 82 (0.6) | 68 (0.5) | 52 (0.5) | 41 (0.6) | 47 (0.7) | 34 (0.7) | 25 (0.6) | 54 (0.6) | 20 (0.6) | 6 (0.4) | 11 (0.3) | 83 (0.5) | 60 (0.8) | 3 (1.1) |
| Insulin monotherapy, n (%) | 548 (4.6) | 332 (4.7) | 216 (4.5) | 141 (4.4) | 137 (4.2) | 231 (5.0) | 75 (4.2) | 52 (4.4) | 161 (5.0) | 127 (5.7) | 77 (5.3) | 56 (2.9) | 155 (4.3) | 281 (5.6) | 80 (4.3) |
| Insulin + NIAD, n (%) | 620 (3.1) | 388 (3.4) | 232 (2.7) | 209 (2.6) | 175 (3.2) | 183 (3.8) | 57 (3.2) | 58 (3.5) | 189 (3.1) | 162 (3.3) | 101 (3.2) | 53 (2.2) | 326 (3.2) | 234 (3.2) | 26 (3.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mata-Cases, M.; Mauricio, D.; Real, J.; Vlacho, B.; Romera-Liebana, L.; Molist-Brunet, N.; Cedenilla, M.; Franch-Nadal, J. Potential Risk of Overtreatment in Patients with Type 2 Diabetes Aged 75 Years or Older: Data from a Population Database in Catalonia, Spain. J. Clin. Med. 2022, 11, 5134. https://doi.org/10.3390/jcm11175134
Mata-Cases M, Mauricio D, Real J, Vlacho B, Romera-Liebana L, Molist-Brunet N, Cedenilla M, Franch-Nadal J. Potential Risk of Overtreatment in Patients with Type 2 Diabetes Aged 75 Years or Older: Data from a Population Database in Catalonia, Spain. Journal of Clinical Medicine. 2022; 11(17):5134. https://doi.org/10.3390/jcm11175134
Chicago/Turabian StyleMata-Cases, Manel, Didac Mauricio, Jordi Real, Bogdan Vlacho, Laura Romera-Liebana, Núria Molist-Brunet, Marta Cedenilla, and Josep Franch-Nadal. 2022. "Potential Risk of Overtreatment in Patients with Type 2 Diabetes Aged 75 Years or Older: Data from a Population Database in Catalonia, Spain" Journal of Clinical Medicine 11, no. 17: 5134. https://doi.org/10.3390/jcm11175134