
Ureteral Access Sheaths and Its Use in the Future: A Comprehensive Update Based on a Literature Review
 , , , , , ,
, , , , , , {kind=link}
Abstract
:1. Introduction
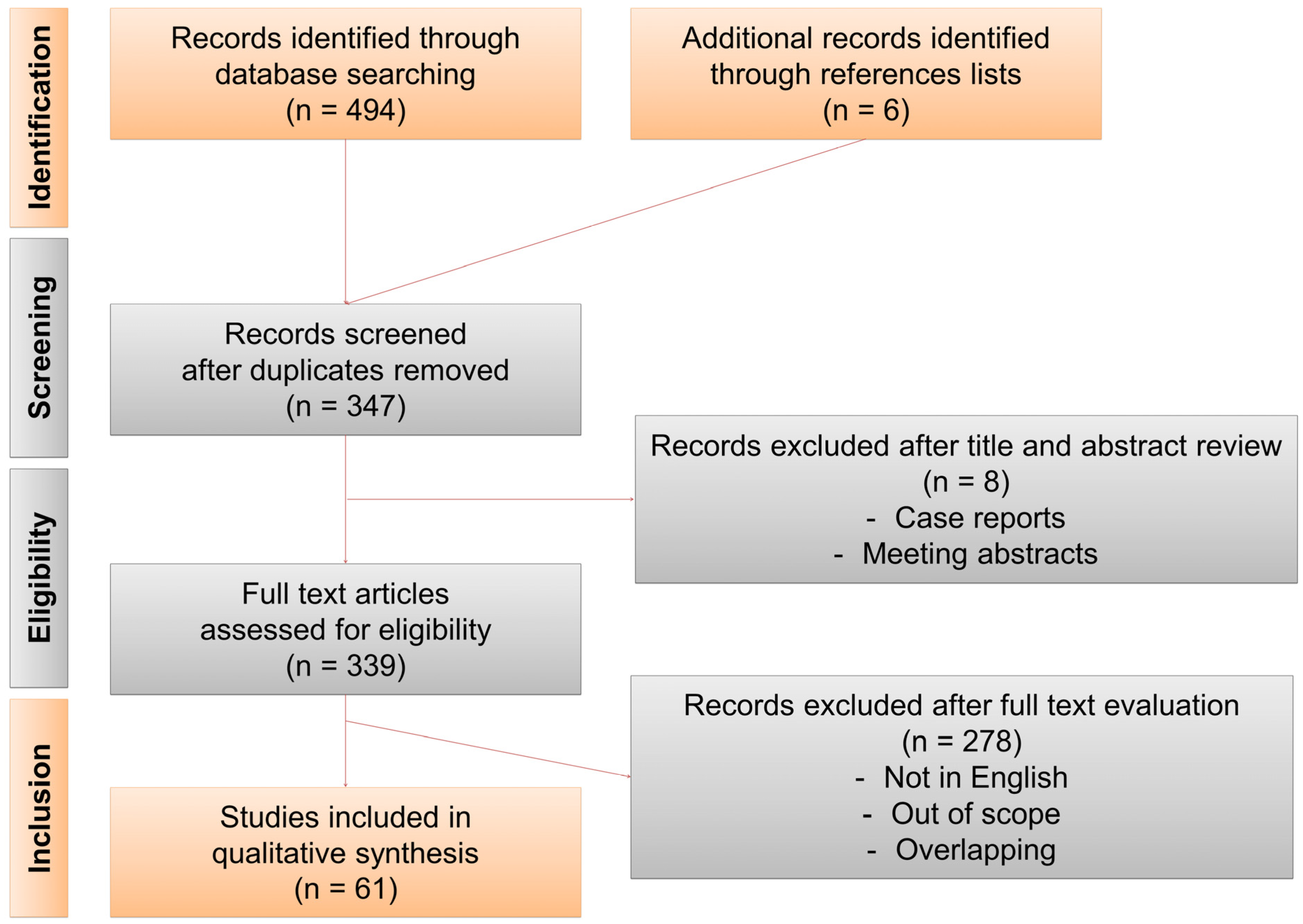
2. Methods
3. Results
3.1. Intrarenal Pressure (IRP)
3.2. Temperature
3.3. Stone Free Rates
3.4. Complications
3.4.1. Pain
3.4.2. Infections
3.4.3. Lesions
3.4.4. Strictures
3.5. UAS and the Three Game Changers
3.5.1. TFL
3.5.2. Small Digital Flexible Ureteroscope
3.5.3. Modified UAS with Pressure Control
3.6. Influence of Prestenting and Alpha Blockers
3.7. UAS and UTUC
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- De Coninck, V.; Keller, E.X.; Rodriguez-Monsalve, M.; Audouin, M.; Doizi, S.; Traxer, O. Systematic review of ureteral access sheaths: Facts and myths. BJU Int. 2018, 122, 959–969. [Google Scholar] [CrossRef]
- Huang, J.; Zhao, Z.; AlSmadi, J.K.; Liang, X.; Zhong, F.; Zeng, T.; Wu, W.; Deng, T.; Lai, Y.; Liu, L.; et al. Use of the ureteral access sheath during ureteroscopy: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0193600. [Google Scholar] [CrossRef] [PubMed]
- Keller, E.X.; De Coninck, V.; Traxer, O. Next-Generation Fiberoptic and Digital Ureteroscopes. Urol. Clin. N. Am. 2019, 46, 147–163. [Google Scholar] [CrossRef] [PubMed]
- Traxer, O.; Keller, E.X. Thulium fiber laser: The new player for kidney stone treatment? A comparison with Holmium:YAG laser. World. J. Urol. 2020, 38, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Traxer, O.; Corrales, M. Managing Urolithiasis with Thulium Fiber Laser: Updated Real-Life Results-A Systematic Review. J. Clin. Med. 2021, 10, 3390. [Google Scholar] [CrossRef]
- Agrawal, S.; Patil, A.; Sabnis, R.B.; Singh, A.G.; Ganpule, A.P.; Desai, M.R. Initial experience with slimmest single-use flexible ureteroscope Uscope PU3033A (PUSEN) in retrograde intrarenal surgery and its comparison with Uscope PU3022a: A single-center prospective study. World J. Urol. 2021, 39, 3957–3962. [Google Scholar] [CrossRef]
- Doizi, S.; Letendre, J.; Cloutier, J.; Ploumidis, A.; Traxer, O. Continuous monitoring of intrapelvic pressure during flexible ureteroscopy using a sensor wire: A pilot study. World J. Urol. 2021, 39, 555–561. [Google Scholar] [CrossRef]
- Huang, J.; Xie, D.; Xiong, R.; Deng, X.; Huang, C.; Fan, D.; Peng, Z.; Qin, W.; Zeng, M.; Song, L. The Application of Suctioning Flexible Ureteroscopy With Intelligent Pressure Control in Treating Upper Urinary Tract Calculi on Patients With a Solitary Kidney. Urology 2018, 111, 44–47. [Google Scholar] [CrossRef]
- Doizi, S.; Uzan, A.; Keller, E.X.; De Coninck, V.; Kamkoum, H.; Barghouthy, Y.; Ventimiglia, E.; Traxer, O. Comparison of intrapelvic pressures during flexible ureteroscopy, mini-percutaneous nephrolithotomy, standard percutaneous nephrolithotomy, and endoscopic combined intrarenal surgery in a kidney model. World J. Urol. 2021, 39, 2709–2717. [Google Scholar] [CrossRef]
- Patel, A.U.; Aldoukhi, A.H.; Majdalany, S.E.; Plott, J.; Ghani, K.R. Development and Testing of an Anatomic in vitro Kidney Model for Measuring Intrapelvic Pressure During Ureteroscopy. Urology 2021, 154, 83–88. [Google Scholar] [CrossRef]
- Patel, R.M.; Jefferson, F.A.; Owyong, M.; Hofmann, M.; Ayad, M.L.; Osann, K.; Okhunov, Z.; Landman, J.; Clayman, R.V. Characterization of intracalyceal pressure during ureteroscopy. World J. Urol. 2021, 39, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Loftus, C.; Byrne, M.; Monga, M. High pressure endoscopic irrigation: Impact on renal histology. Int. Braz. J. Urol. 2021, 47, 350–356. [Google Scholar] [CrossRef]
- Shrestha, A.; Gharti, B.B.; Adhikari, B. Perirenal Extravasation After Retrograde Intrarenal Surgery for Renal Stones: A Prospective Study. Cureus 2022, 14, e21283. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Xie, G.; Zheng, Z.; Liu, W.; Zhu, J.; Huang, T.; Lu, Y.; Cheng, Y. The Effect of Ratio of Endoscope-Sheath Diameter on Intrapelvic Pressure During Flexible Ureteroscopic Lasertripsy. J. Endourol. 2019, 33, 132–139. [Google Scholar] [CrossRef] [PubMed]
- MacCraith, E.; Yap, L.C.; Elamin, M.; Patterson, K.; Brady, C.M.; Hennessey, D.B. Evaluation of the Impact of Ureteroscope, Access Sheath, and Irrigation System Selection on Intrarenal Pressures in a Porcine Kidney Model. J. Endourol. 2021, 35, 512–517. [Google Scholar] [CrossRef]
- Sener, T.E.; Tanidir, Y.; Bin Hamri, S.; Sever, I.H.; Ozdemir, B.; Al-Humam, A.; Traxer, O. Effects of flexible ureteroscopy on renal blood flow: A prospective evaluation. Scand. J. Urol. 2018, 52, 213–218. [Google Scholar] [CrossRef]
- De Coninck, V.; Defraigne, C.; Traxer, O. Watt determines the temperature during laser lithotripsy. World J. Urol. 2021, 40, 1257–1258. [Google Scholar] [CrossRef]
- Okhunov, Z.; Jiang, P.; Afyouni, A.S.; Ayad, M.; Arada, R.; Brevik, A.; Akopian, G.; Patel, R.M.; Landman, J.; Clayman, R.V. Caveat Emptor: The Heat Is “ON”-An In Vivo Evaluation of the Thulium Fiber Laser and Temperature Changes in the Porcine Kidney During Dusting and Fragmentation Modes. J. Endourol. 2021, 35, 1716–1722. [Google Scholar] [CrossRef]
- Winship, B.; Terry, R.; Boydston, K.; Carlos, E.; Wollin, D.; Peters, C.; Li, J.; Preminger, G.; Lipkin, M. Holmium:Yttrium-Aluminum-Garnet Laser Pulse Type Affects Irrigation Temperatures in a Benchtop Ureteral Model. J. Endourol. 2019, 33, 896–901. [Google Scholar] [CrossRef]
- Belle, J.D.; Chen, R.; Srikureja, N.; Amasyali, A.; Keheila, M.; Baldwin, D.D. Does the Novel Thulium Fiber Laser Have a Higher Risk of Urothelial Thermal Injury than the Conventional Holmium Laser in an In Vitro Study? J. Endourol. 2022, in press. [CrossRef]
- Damar, E.; Senocak, C.; Ozbek, R.; Haberal, H.B.; Sadioglu, F.E.; Yordam, M.; Bozkurt, O.F. Does ureteral access sheath affect the outcomes of retrograde intrarenal surgery: A prospective study. Minim. Invasive Ther. Allied Technol. 2021, 31, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Yitgin, Y.; Yitgin, E.; Verep, S.; Gasimov, K.; Tefik, T.; Karakose, A. Is Access Sheath Essential for Safety and Effective Retrograde Intrarenal Stone Surgery? J. Coll. Physicians Surg. Pak. 2021, 31, 1202–1206. [Google Scholar] [PubMed]
- Lima, A.; Reeves, T.; Geraghty, R.; Pietropaolo, A.; Whitehurst, L.; Somani, B.K. Impact of ureteral access sheath on renal stone treatment: Prospective comparative non-randomised outcomes over a 7-year period. World J. Urol. 2020, 38, 1329–1333. [Google Scholar] [CrossRef]
- Meier, K.; Hiller, S.; Dauw, C.; Hollingsworth, J.; Kim, T.; Qi, J.; Telang, J.; Ghani, K.R.; Jafri, S.M.A. Understanding Ureteral Access Sheath Use Within a Statewide Collaborative and Its Effect on Surgical and Clinical Outcomes. J. Endourol. 2021, 35, 1340–1347. [Google Scholar] [CrossRef]
- Kahraman, O.; Dogan, H.S.; Asci, A.; Asi, T.; Haberal, H.B.; Tekgul, S. Factors associated with the stone-free status after retrograde intrarenal surgery in children. Int. J. Clin. Pract. 2021, 75, e14667. [Google Scholar] [CrossRef] [PubMed]
- Komeya, M.; Odaka, H.; Watanabe, T.; Kiuchi, H.; Ogawa, T.; Yao, M.; Matsuzaki, J. Gap between UAS and ureteroscope predicts renal stone-free rate after flexible ureteroscopy with the fragmentation technique. World J. Urol. 2021, 39, 2733–2739. [Google Scholar] [CrossRef]
- Hawken, S.R.; Hiller, S.C.; Daignault-Newton, S.; Ghani, K.R.; Hollingsworth, J.M.; Conrado, B.; Maitland, C.; Wenzler, D.L.; Ludlow, J.K.; Ambani, S.N.; et al. Opioid-Free Discharge is Not Associated With Increased Unplanned Healthcare Encounters After Ureteroscopy: Results From a Statewide Quality Improvement Collaborative. Urology 2021, 158, 57–65. [Google Scholar] [CrossRef]
- Oguz, U.; Sahin, T.; Senocak, C.; Ozyuvali, E.; Bozkurt, O.F.; Resorlu, B.; Unsal, A. Factors associated with postoperative pain after retrograde intrarenal surgery for kidney stones. Turk. J. Urol. 2017, 43, 303–308. [Google Scholar] [CrossRef]
- Inoue, T.; Hamamoto, S.; Okada, S.; Yamamichi, F.; Fujita, M.; Tominaga, K.; Fujisawa, M. Evaluating Predictive Factor of Systemic Inflammatory Response Syndrome and Postoperative Pain in Patients Without Ureteral Stent Placement After Ureteral Access Sheath Use in Flexible Ureteroscopy for Stone Management. J. Endourol. 2022, 36, 169–175. [Google Scholar] [CrossRef]
- Bozzini, G.; Bevilacqua, L.; Besana, U.; Calori, A.; Pastore, A.; Romero Otero, J.; Macchi, A.; Broggini, P.; Breda, A.; Gozen, A.; et al. Ureteral access sheath-related injuries vs. post-operative infections. Is sheath insertion always needed? A prospective randomized study to understand the lights and shadows of this practice. Actas Urol. Esp. 2021, 45, 576–581. [Google Scholar] [CrossRef]
- De Coninck, V.; Keller, E.X.; Somani, B.; Giusti, G.; Proietti, S.; Rodriguez-Socarras, M.; Rodriguez-Monsalve, M.; Doizi, S.; Ventimiglia, E.; Traxer, O. Complications of ureteroscopy: A complete overview. World J. Urol. 2020, 38, 2147–2166. [Google Scholar] [CrossRef] [PubMed]
- Mi, Q.; Meng, X.; Meng, L.; Chen, D.; Fang, S. Risk Factors for Systemic Inflammatory Response Syndrome Induced by Flexible Ureteroscope Combined with Holmium Laser Lithotripsy. Biomed. Res. Int. 2020, 2020, 6842479. [Google Scholar] [CrossRef] [PubMed]
- Lildal, S.K.; Andreassen, K.H.; Jung, H.; Pedersen, M.R.; Osther, P.J.S. Evaluation of ureteral lesions in ureterorenoscopy: Impact of access sheath use. Scand. J. Urol. 2018, 52, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Aykanat, C.; Balci, M.; Senel, C.; Ozercan, A.Y.; Coser, S.; Aslan, Y.; Guzel, O.; Asfuroglu, A.; Karabulut, E.; Tuncel, A. The Impact of Ureteral Access Sheath Size on Perioperative Parameters and Postoperative Ureteral Stricture in Retrograde Intrarenal Surgery. J. Endourol. 2022, 36, 1013–1017. [Google Scholar] [CrossRef] [PubMed]
- Fulla, J.; Prasanchaimontri, P.; Rizk, A.; Loftus, C.; Remer, E.M.; Monga, M. Ureteral Diameter as Predictor of Ureteral Injury during Ureteral Access Sheath Placement. J. Urol. 2021, 205, 159–164. [Google Scholar] [CrossRef]
- Stern, K.L.; Loftus, C.J.; Doizi, S.; Traxer, O.; Monga, M. A Prospective Study Analyzing the Association Between High-grade Ureteral Access Sheath Injuries and the Formation of Ureteral Strictures. Urology 2019, 128, 38–41. [Google Scholar] [CrossRef]
- Shvero, A.; Herzberg, H.; Zilberman, D.; Mor, Y.; Winkler, H.; Kleinmann, N. Is it safe to use a ureteral access sheath in an unstented ureter? BMC Urol. 2019, 19, 80. [Google Scholar] [CrossRef]
- Tracy, C.R.; Ghareeb, G.M.; Paul, C.J.; Brooks, N.A. Increasing the size of ureteral access sheath during retrograde intrarenal surgery improves surgical efficiency without increasing complications. World J. Urol. 2018, 36, 971–978. [Google Scholar] [CrossRef]
- Mosquera, L.; Pietropaolo, A.; Brewin, A.; Madarriaga, Y.Q.; de Knecht, E.L.; Jones, P.; Bujons, A.; Griffin, S.; Somani, B.K. Safety and Outcomes of using ureteric access sheath (UAS) for treatment of Pediatric renal stones: Outcomes from 2 tertiary endourology centers. Urology 2021, 157, 222–226. [Google Scholar] [CrossRef]
- Ulvik, O.; Harneshaug, J.R.; Gjengsto, P. Ureteral Strictures Following Ureteroscopic Stone Treatment. J. Endourol. 2021, 35, 985–990. [Google Scholar] [CrossRef]
- Corrales, M.; Traxer, O. Initial clinical experience with the new thulium fiber laser: First 50 cases. World J. Urol. 2021, 39, 3945–3950. [Google Scholar] [CrossRef] [PubMed]
- Enikeev, D.; Grigoryan, V.; Fokin, I.; Morozov, A.; Taratkin, M.; Klimov, R.; Kozlov, V.; Gabdullina, S.; Glybochko, P. Endoscopic lithotripsy with a SuperPulsed thulium-fiber laser for ureteral stones: A single-center experience. Int. J. Urol. 2021, 28, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Enikeev, D.; Taratkin, M.; Klimov, R.; Inoyatov, J.; Azilgareeva, C.; Ali, S.; Korolev, D.; Corrales, M.; Traxer, O.; Glybochko, P. Superpulsed Thulium Fiber Laser for Stone Dusting: In Search of a Perfect Ablation Regimen-A Prospective Single-Center Study. J. Endourol. 2020, 34, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Martov, A.G.; Ergakov, D.V.; Guseynov, M.; Andronov, A.S.; Plekhanova, O.A. Clinical Comparison of Super Pulse Thulium Fiber Laser and High-Power Holmium Laser for Ureteral Stone Management. J. Endourol. 2021, 35, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Geavlete, B.; Cozma, C.; Geavlete, P. The “no-touch” technique in the flexible ureteroscopic approach of renal stones. J. Med. Life 2021, 14, 481–486. [Google Scholar] [CrossRef]
- Geavlete, B.; Ene, C.; Iordache, V.; Geavlete, P. Initial Experience with the New Super Thin Single-use Pusen Flexible Ureteroscope 7.5 Fr in Renal Stones Endoscopic Treatment. Chirurgia 2021, 116, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Wang, D.; Zhang, T.; Wan, S.P. Modified Access Sheath for Continuous Flow Ureteroscopic Lithotripsy: A Preliminary Report of a Novel Concept and Technique. J. Endourol. 2016, 30, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Qiu, X.; Du, C.; Xie, D.; Liu, T.; Wang, G.; Song, L. The Comparison Study of Flexible Ureteroscopic Suctioning Lithotripsy With Intelligent Pressure Control Versus Minimally Invasive Percutaneous Suctioning Nephrolithotomy in Treating Renal Calculi of 2 to 3 cm in Size. Surg. Innov. 2019, 26, 528–535. [Google Scholar] [CrossRef]
- Deng, X.; Song, L.; Xie, D.; Fan, D.; Zhu, L.; Yao, L.; Wang, X.; Liu, S.; Zhang, Y.; Liao, X.; et al. A Novel Flexible Ureteroscopy with Intelligent Control of Renal Pelvic Pressure: An Initial Experience of 93 Cases. J. Endourol. 2016, 30, 1067–1072. [Google Scholar] [CrossRef]
- Chen, Y.; Li, C.; Gao, L.; Lin, L.; Zheng, L.; Ke, L.; Chen, J.; Kuang, R. Novel flexible vacuum-assisted ureteral access sheath (FV-UAS) can actively control intrarenal pressure and obtain a complete stone-free status. J. Endourol. 2022, in press.
- AlSmadi, J.K.; Li, X.; Zeng, G. Use of a modified ureteral access sheath in semi-rigid ureteroscopy to treat large upper ureteral stones is associated with high stone free rates. Asian J. Urol. 2019, 6, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Cui, Y.; Zeng, F.; Li, Y.; Chen, Z.; Hequn, C. Comparison of suctioning and traditional ureteral access sheath during flexible ureteroscopy in the treatment of renal stones. World J. Urol. 2019, 37, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Wang, Y.; Li, J.; Han, Z. Prestenting Versus Nonprestenting on the Outcomes of Flexible Ureteroscopy for Large Upper Urinary Stones: A Systematic Review and Meta-Analysis. Urol. Int. 2021, 105, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Law, Y.X.T.; Teoh, J.Y.C.; Castellani, D.; Lim, E.J.; Chan, E.O.T.; Wroclawski, M.; Pirola, G.M.; Giulioni, C.; Rubilotta, E.; Gubbioti, M.; et al. Role of pre-operative ureteral stent on outcomes of retrograde intra-renal surgery (RIRS): Systematic review and meta-analysis of 3831 patients and comparison of Asian and non-Asian cohorts. World J. Urol. 2022, 40, 1377–1389. [Google Scholar] [CrossRef]
- Jiang, P.; Afyouni, A.S.; Brevik, A.; Peta, A.; King, T.; Dinh, S.T.; Ayad, M.; Larson, K.; Limfueco, L.; Kosmala, C.M.; et al. The Impact of One Week of Pre-stenting on Porcine Ureteral Luminal Circumference. J. Endourol. 2022, 36, 885–890. [Google Scholar] [CrossRef]
- Kim, J.K.; Choi, C.I.; Lee, S.H.; Han, J.H.; Shim, Y.S.; Choo, M.S.; Young Endourological Study Group. Silodosin for Prevention of Ureteral Injuries Resulting from Insertion of a Ureteral Access Sheath: A Randomized Controlled Trial. Eur. Urol. Focus 2022, 8, 572–579. [Google Scholar] [CrossRef]
- Morley, C.; Hajiran, A.; Elbakry, A.A.; Al-Qudah, H.S.; Al-Omar, O. Evaluation of Preoperative Tamsulosin Role in Facilitating Ureteral Orifice Navigation for School-Age Pediatric Ureteroscopy. Res. Rep. Urol. 2020, 12, 563–568. [Google Scholar] [CrossRef]
- Erturhan, S.; Bayrak, O.; Sen, H.; Yilmaz, A.E.; Seckiner, I. Can alpha blockers facilitate the placement of ureteral access sheaths in retrograde intrarenal surgery? Turk. J. Urol. 2019, 45, 108–112. [Google Scholar] [CrossRef]
- Douglawi, A.; Ghoreifi, A.; Lee, R.; Yip, W.; Seyedian, S.S.L.; Ahmadi, H.; Cai, J.; Miranda, G.; Yu, W.; Bhanvadia, S.; et al. Bladder Recurrence Following Diagnostic Ureteroscopy in Patients Undergoing Nephroureterectomy for Upper Tract Urothelial Cancer: Is Ureteral Access Sheath Protective? Urology 2022, 160, 142–146. [Google Scholar] [CrossRef]
- Rehman, J.; Monga, M.; Landman, J.; Lee, D.I.; Felfela, T.; Conradie, M.C.; Srinivas, R.; Sundaram, C.P.; Clayman, R.V. Characterization of intrapelvic pressure during ureteropyeloscopy with ureteral access sheaths. Urology 2003, 61, 713–718. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Coninck, V.; Somani, B.; Sener, E.T.; Emiliani, E.; Corrales, M.; Juliebø-Jones, P.; Pietropaolo, A.; Mykoniatis, I.; Zeeshan Hameed, B.M.; Esperto, F.; et al. Ureteral Access Sheaths and Its Use in the Future: A Comprehensive Update Based on a Literature Review. J. Clin. Med. 2022, 11, 5128. https://doi.org/10.3390/jcm11175128
De Coninck V, Somani B, Sener ET, Emiliani E, Corrales M, Juliebø-Jones P, Pietropaolo A, Mykoniatis I, Zeeshan Hameed BM, Esperto F, et al. Ureteral Access Sheaths and Its Use in the Future: A Comprehensive Update Based on a Literature Review. Journal of Clinical Medicine. 2022; 11(17):5128. https://doi.org/10.3390/jcm11175128
Chicago/Turabian StyleDe Coninck, Vincent, Bhaskar Somani, Emre Tarik Sener, Esteban Emiliani, Mariela Corrales, Patrick Juliebø-Jones, Amelia Pietropaolo, Ioannis Mykoniatis, Belthangady M. Zeeshan Hameed, Francesco Esperto, and et al. 2022. "Ureteral Access Sheaths and Its Use in the Future: A Comprehensive Update Based on a Literature Review" Journal of Clinical Medicine 11, no. 17: 5128. https://doi.org/10.3390/jcm11175128