


Uneven Meibomian Gland Dropout in Patients with Meibomian Gland Dysfunction and Demodex Infestation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Diagnosis of MGD and Demodex Infestation
2.3. Ocular Surface Examination
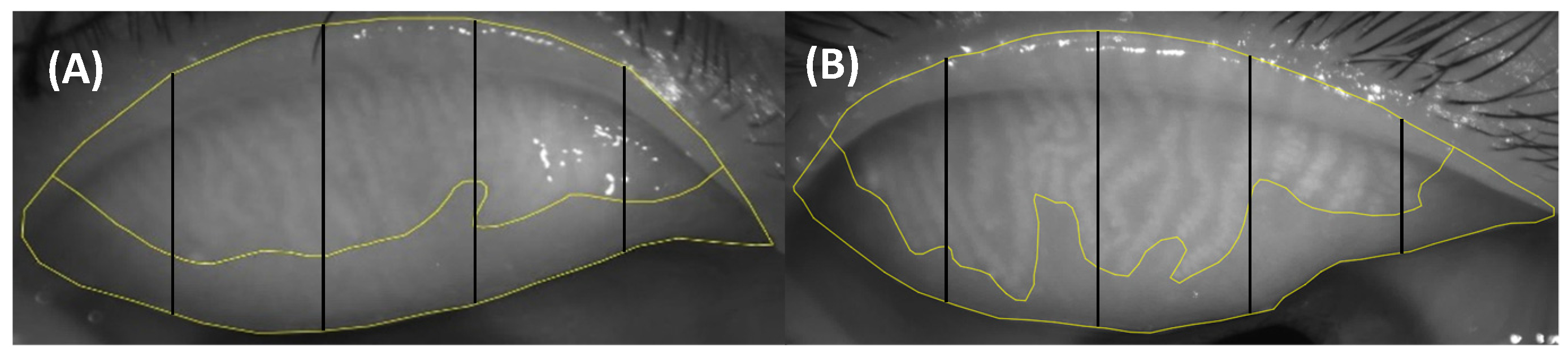
2.4. Uneven Atrophy Score (UAS)
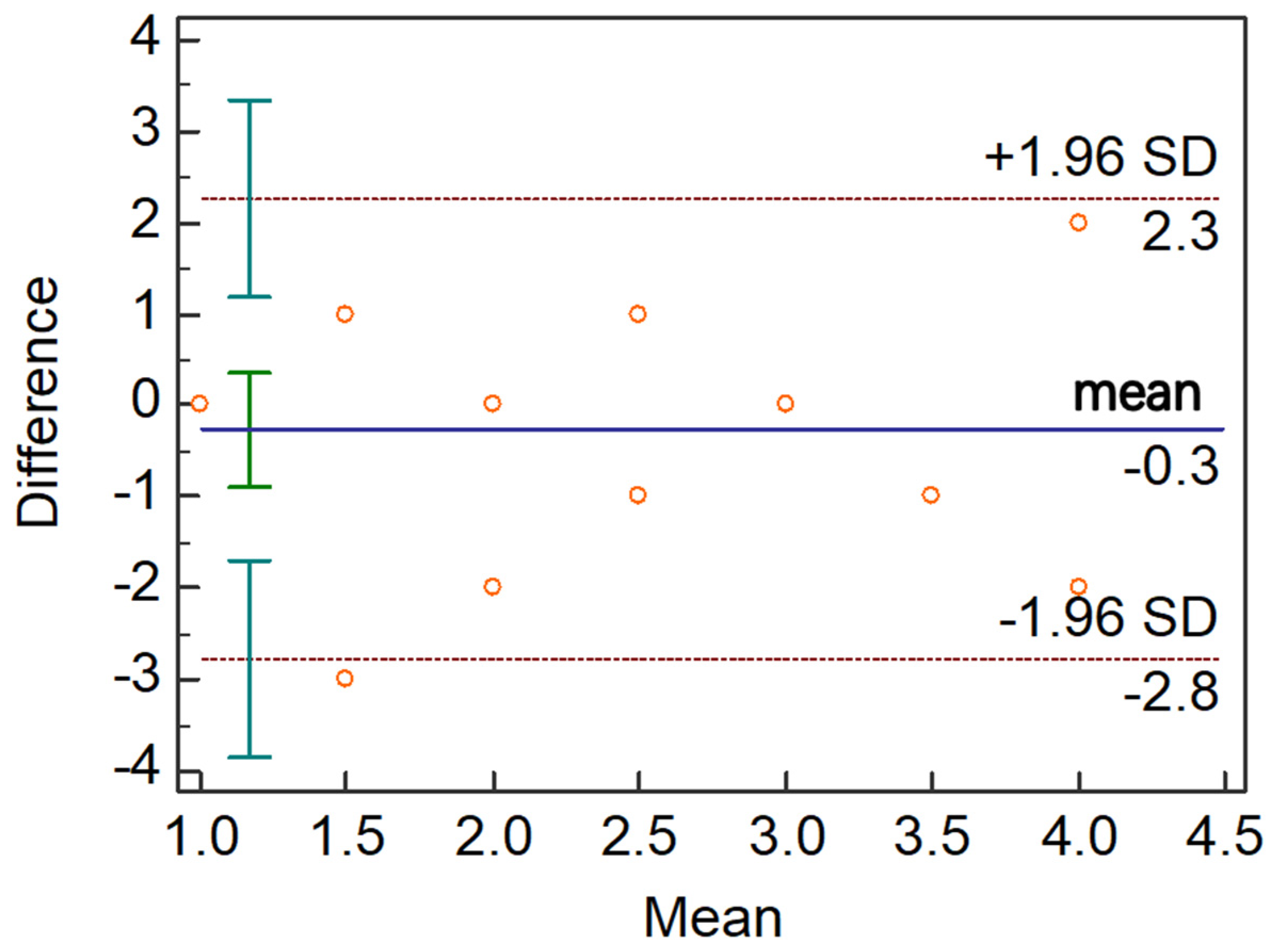
2.5. Repeatability of UAS
2.6. Statistical Analysis
3. Results
3.1. Basic Characteristics and Ocular Surface Parameters
3.2. Uneven Atrophy Score between Three Groups
3.3. Correlations between Uneven Atrophy Score and Ocular Surface Parameters
3.4. The Intra-Observer Repeatability of UAS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, X.B.; Ding, Y.H.; He, W. The association between demodex infestation and ocular surface manifestations in meibomian gland dysfunction. Int. J. Ophthalmol. 2018, 11, 589–592. [Google Scholar] [PubMed]
- Basta-Juzbasić, A.; Subić, J.S.; Ljubojević, S. Demodex folliculorum in development of dermatitis rosaceiformis steroidica and rosacea-related diseases. Clin. Dermatol. 2002, 20, 135–140. [Google Scholar]
- Cheng, A.M.S.; Sheha, H.; Tseng, S.C.G. Recent advances on ocular Demodex infestation. Curr. Opin. Ophthalmol. 2015, 26, 295–300. [Google Scholar]
- Kabatas, N.; Dogan, A.S.; Kabatas, E.U.; Acar, M.; Bicer, T.; Gurdal, C. The Effect of Demodex Infestation on Blepharitis and the Ocular Symptoms. Eye Contact Lens 2017, 43, 64–67. [Google Scholar]
- Yildiz-Tas, A.; Arici, C.; Mergen, B.; Sahin, A. In Vivo Confocal Microscopy in Blepharitis Patients with Ocular Demodex Infestation. Ocul. Immunol. Inflamm. 2021, 1, 1–6. [Google Scholar] [CrossRef]
- Kheirkhah, A.; Casas, V.; Li, W.; Raju, V.K.; Tseng, S.C. Corneal manifestations of ocular demodex infestation. Am. J. Ophthalmol. 2007, 143, 743–749. [Google Scholar]
- English, F.P.; Nutting, W.B. Demodicosis of ophthalmic concern. Am. J. Ophthalmol. 1981, 91, 362–372. [Google Scholar]
- Liang, L.; Liu, Y.; Ding, X.; Ke, H.; Chen, C.; Tseng, S.C.G. Significant correlation between meibomian gland dysfunction and keratitis in young patients with Demodex brevis infestation. Br. J. Ophthalmol. 2018, 102, 1098–1102. [Google Scholar] [PubMed]
- Rabensteiner, D.F.; Aminfar, H.; Boldin, I.; Nitsche-Resch, M.; Berisha, B.; Schwantzer, G.; Horwath-Winter, J. Demodex Mite Infestation and its Associations with Tear Film and Ocular Surface Parameters in Patients with Ocular Discomfort. Am. J. Ophthalmol. 2019, 204, 7–12. [Google Scholar]
- Lee, S.H.; Chun, Y.S.; Kim, J.H.; Kim, E.S.; Kim, J.C. The relationship between demodex and ocular discomfort. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2906–2911. [Google Scholar]
- Cheng, S.N.; Jiang, F.G.; Chen, H.; Gao, H.; Huang, Y.K. Intense Pulsed Light Therapy for Patients with Meibomian Gland Dysfunction and Ocular Demodex Infestation. Curr. Med. Sci. 2019, 3, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.Y.; Di Pascuale, M.A.; Li, W.; Liu, D.T.; Baradaran-Rafii, A.; Elizondo, A.; Kawakita, T.; Raju, V.K.; Tseng, S.C. High prevalence of Demodex in eyelashes with cylindrical dandruff. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3089–3094. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Ding, X.; Tseng, S.C. High prevalence of demodex brevis infestation in chalazia. Am. J. Ophthalmol. 2014, 157, 342–348.e1. [Google Scholar] [PubMed]
- English, F.P.; Cohn, D.; Groeneveld, E.R. Demodectic mites and chalazion. Am. J. Ophthalmol. 1985, 100, 482–483. [Google Scholar] [CrossRef]
- Pan, S.; Chen, Y. A clinical study on the correlation between demodex infestation and ocular surface changes in patients with meibomian gland dysfunction. Indian J. Ophthalmol. 2021, 69, 2389–2394. [Google Scholar]
- Huo, Y.N.; Mo, Y.P.; Wu, Y.Y.; Fang, F.; Jin, X.M. Therapeutic effect of intense pulsed light with optimal pulse technology on meibomian gland dysfunction with and without ocular Demodex infestation. Ann. Transl. Med. 2021, 9, 238. [Google Scholar] [CrossRef]
- Zhang, Z.H.; Lin, X.L.; Yu, X.X.; Fu, Y.N.; Chen, X.Y.; Yang, W.H.; Dai, Q. Meibomian Gland Density: An Effective Evaluation Index of Meibomian Gland Dysfunction Based on Deep Learning and Transfer Learning. J. Clin. Med. 2022, 11, 2396. [Google Scholar] [CrossRef]
- Lin, X.L.; Fu, Y.N.; Li, L.; Chen, C.Q.; Chen, X.W.; Mao, Y.Y.; Lian, H.L.; Yang, W.H.; Dai, Q. A Novel Quantitative Index of Meibomian Gland Dysfunction, the Meibomian Gland Tortuosity. Transl. Vis. Sci. Technol. 2020, 9, 34. [Google Scholar]
- Yin, Y.; Gong, L. Uneven Meibomian Gland Dropout Over the Tarsal Plate and its Correlation with Meibomian Gland Dysfunction. Cornea 2015, 3, 1200–1205. [Google Scholar] [CrossRef]
- Li, Y.; Lu, J.; Zhou, Q.Z.; Wang, C.X.; Zeng, Q.Y.; Chen, T.H.; Liu, C.; Kang, Y.W.; Li, S.W. Analysis of Clinical and Regional Distribution Characteristics of Obstructive Meibomian Gland Dysfunction in China: A Multicenter Study. Curr. Eye Res. 2020, 45, 1373–1379. [Google Scholar] [CrossRef]
- Asian Dry Eye Association China Branch. Expert Consensus on diagnosis and Treatment of Demodex blepharitis in China (2018). Zhonghua Yan Ke Za Zhi 2020, 57, 564–572. [Google Scholar]
- Arita, R.; Itoh, K.; Maeda, S.; Maeda, K.; Furuta, A.; Fukuoka, S.; Tomidokoro, A.; Amano, S. Proposed diagnostic criteria for obstructive meibomian gland dysfunction. Ophthalmology 2009, 116, 2058–2063.e1. [Google Scholar] [CrossRef] [PubMed]
- Adil, M.Y.; Xiao, J.; Olafsson, J.; Chen, X.; Lagali, N.S.; Raeder, S.; Utheim, O.A.; Dartt, D.A.; Utheim, T.P. Meibomian Gland Morphology Is a Sensitive Early Indicator of Meibomian Gland Dysfunction. Am. J. Ophthalmol. 2019, 200, 16–25. [Google Scholar] [CrossRef]
- Georgala, S.; Katoulis, A.C.; Kylafis, G.D.; Koumantaki-Mathioudaki, E.; Georgala, C.; Aroni, K. Increased density of Demodex folliculorum and evidence of delayed hypersensitivity reaction in subjects with papulopustular rosacea. J. Eur. Acad. Dermatol. Venereol. 2001, 15, 441–444. [Google Scholar] [CrossRef]
- Forton, F.; Germaux, M.A.; Brasseur, T.; De Liever, A.; Laporte, M.; Mathys, C.; Sass, U.; Stene, J.J.; Thibaut, S.; Tytgat, M.; et al. Demodicosis and rosacea: Epidemiology and significance in daily dermatologic practice. J. Am. Acad. Dermatol. 2005, 52, 74–87. [Google Scholar] [CrossRef]
- Gao, Y.Y.; Di Pascuale, M.A.; Elizondo, A.; Tseng, S.C. Clinical treatment of ocular demodecosis by lid scrub with tea tree oil. Cornea 2007, 26, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, C.; Balci, O.; Demirci, G.; Odabasi, M.; Ozsutcu, M.; Nurozler Tabakci, B. Comparison of Biomicroscopy and Light Microscopy Findings in Demodex Diagnosis in Patients with Chronic Blepharitis. Eye Contact Lens 2020, 46, 297–300. [Google Scholar] [CrossRef]
- Karincaoglu, Y.; Bayram, N.; Aycan, O.; Esrefoglu, M. The clinical importance of demodex folliculorum presenting with nonspecific facial signs and symptoms. J. Dermatol. 2004, 31, 618–626. [Google Scholar] [CrossRef]
- Gao, H.; Chen, H.; Xie, H.T.; Xu, K.K.; Shi, B.J.; Huang, Y.K. Changes in Meibum Lipid Composition with Ocular Demodex Infestation. Transl. Vis. Sci. Technol. 2021, 10, 6. [Google Scholar] [CrossRef]
- Liang, X.; Li, Y.; Xiong, K.; Chen, S.; Li, Z.; Zhang, Z.; Xia, Z.; Yi, G.; Fu, M. Demodex Infection Changes Ocular Surface Microbial Communities, in Which Meibomian Gland Dysfunction May Play a Role. Ophthalmol. Ther. 2021, 10, 601–617. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Control Group | Demodex-Negative MGD Group | Demodex-Positive MGD Group | p-Value 1 | p-Value 2 | p-Value 3 | |
|---|---|---|---|---|---|---|
| Age (years), Median (IQR) | 25.0 (22.0, 32.0) | 40.0 (30.0, 48.0) | 38.5 (28.0, 55.5) | <0.001 | <0.001 | 1.000 |
| Eyes, n | 43 | 49 | 66 | - | - | - |
| Gender, (n, male/female) | 18/25 | 19/30 | 20/46 | - | - | - |
| OSDI, Median (IQR) | 2.08 (1.19, 8.33) | 37.50 (25.00, 54.55) | 26.05 (13.02, 41.67) | <0.001 | <0.001 | 0.120 |
| TMH (mm), Median (IQR) | 0.20 (0.18, 0.24) | 0.22 (0.18, 0.26) | 0.20 (0.18, 0.24) | 0.466 | 0.799 | 0.569 |
| TBUT (seconds), Median (IQR) | 8.00 (5.00, 15.00) | 2.83 (1.60, 3.08) | 2.00 (1.00, 3.00) | <0.001 | <0.001 | 1.000 |
| CFS (0–20), Median (IQR) | 0.00 (0.00, 0.00) | 0.00 (0.00, 2.00) | 0.00 (0.00, 2.00) | 0.044 | 0.150 | 0.424 |
| Lid margin score (0–4), Median (IQR) | 0.00 (0.00, 1.00) | 2.00 (2.00, 2.00) | 2.00 (2.00, 3.00) | <0.001 | <0.001 | 0.442 |
| Meibograde (0–6), Median (IQR) | 1.00 (0.00, 1.00) | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | <0.001 | <0.001 | 1.000 |
| Normal Control Group | Demodex Negative Group | Demodex Positive Group | p-Value 1 | p-Value 2 | p-Value 3 | * p-Value 1 | * p-Value 2 | * p-Value 3 | |
|---|---|---|---|---|---|---|---|---|---|
| UAS of upper eyelid | 1.00 (0.00, 1.00) | 2.00 (1.00, 3.00) | 3.00 (2.00, 4.00) | 0.021 | <0.001 | 0.037 | 0.100 | <0.001 | 0.042 |
| UAS of lower eyelid | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | 4.00 (3.00, 6.00) | 0.707 | 0.085 | 0.045 | 0.502 | 0.213 | 0.020 |
| UAS of both eyelids | 3.00 (2.00, 4.00) | 3.00 (2.00, 3.00) | 5.00 (4.00, 6.00) | 0.301 | 0.006 | 0.014 | 0.531 | 0.001 | 0.003 |
| Meibograde of upper eyelid | 0.00 (0.00, 0.00) | 1.00 (0.00, 1.00) | 1.00 (0.00, 1.00) | <0.001 | <0.001 | 1.000 | <0.001 | <0.001 | 0.547 |
| Meibograde of lower eyelid | 1.00 (0.00, 1.00) | 1.00 (1.00, 2.00) | 1.00 (1.00, 2.00) | <0.001 | <0.001 | 1.000 | <0.001 | <0.001 | 0.677 |
| Meibograde of both eyelids | 1.00 (0.00, 1.00) | 2.00 (0.00, 3.00) | 2.00 (1.00, 3.00) | <0.001 | <0.001 | 1.000 | <0.001 | <0.001 | 0.960 |
| UAS | Normal Control Group (n = 43) | Demodex Negative Group (n = 49) | Demodex Positive Group (n = 66) | |
|---|---|---|---|---|
| upper eyelid | 0–3 | 42 (97.67%) | 42 (85.71%) | 49 (74.24%) |
| 4–6 | 1 (2.33%) | 7 (14.29%) | 17 (25.76%) | |
| 7–9 | 0 | 0 | 0 | |
| 10–12 | 0 | 0 | 0 | |
| lower eyelid | 0–3 | 39 (90.70%) | 43 (87.76%) | 55 (83.33%) |
| 4–6 | 4 (9.30%) | 6 (12.24%) | 11 (16.67%) | |
| 7–9 | 0 | 0 | 0 | |
| 10–12 | 0 | 0 | 0 | |
| both eyelids | 0–3 | 21 (48.84%) | 14 (28.57%) | 9 (13.64%) |
| 4–6 | 21 (48.84%) | 28 (57.14%) | 42 (63.64%) | |
| 7–9 | 1 (2.33%) | 7 (14.29%) | 14 (21.21%) | |
| 10–12 | 0 | 0 | 1 (1.52%) |
| R-Value | OSDI | TMH | TBUT | CFS | Lid Margin Score | Meibograde |
|---|---|---|---|---|---|---|
| UAS of upper eyelid | 0.293 ‡ | 0.037 | −0.304 ‡ | −0.063 | 0.298 ‡ | 0.329 ‡ |
| UAS of lower eyelid | 0.001 | 0.058 | −0.080 | 0.030 | 0.175 * | 0.245 * |
| UAS of both eyelids | 0.209 * | 0.064 | −0.248 * | −0.008 | 0.287 ‡ | 0.356 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.; Fu, Y.; Lian, H.; Wang, D.; Zhang, Z.; Dai, Q. Uneven Meibomian Gland Dropout in Patients with Meibomian Gland Dysfunction and Demodex Infestation. J. Clin. Med. 2022, 11, 5085. https://doi.org/10.3390/jcm11175085
Yu X, Fu Y, Lian H, Wang D, Zhang Z, Dai Q. Uneven Meibomian Gland Dropout in Patients with Meibomian Gland Dysfunction and Demodex Infestation. Journal of Clinical Medicine. 2022; 11(17):5085. https://doi.org/10.3390/jcm11175085
Chicago/Turabian StyleYu, Xinxin, Yana Fu, Hengli Lian, Dandan Wang, Zuhui Zhang, and Qi Dai. 2022. "Uneven Meibomian Gland Dropout in Patients with Meibomian Gland Dysfunction and Demodex Infestation" Journal of Clinical Medicine 11, no. 17: 5085. https://doi.org/10.3390/jcm11175085