
Association of Acute Headache of COVID-19 and Anxiety/Depression Symptoms in Adults Undergoing Post-COVID-19 Rehabilitation

 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings and Participants
2.2. Outcome Measures
2.2.1. Survey
2.2.2. Depression and Anxiety Symptoms
2.2.3. Assessment of Stress Level
2.2.4. Quality of Life Assessment
2.3. Data Analysis
3. Results
3.1. Participants Characteristics
3.2. Between-Group Comparison
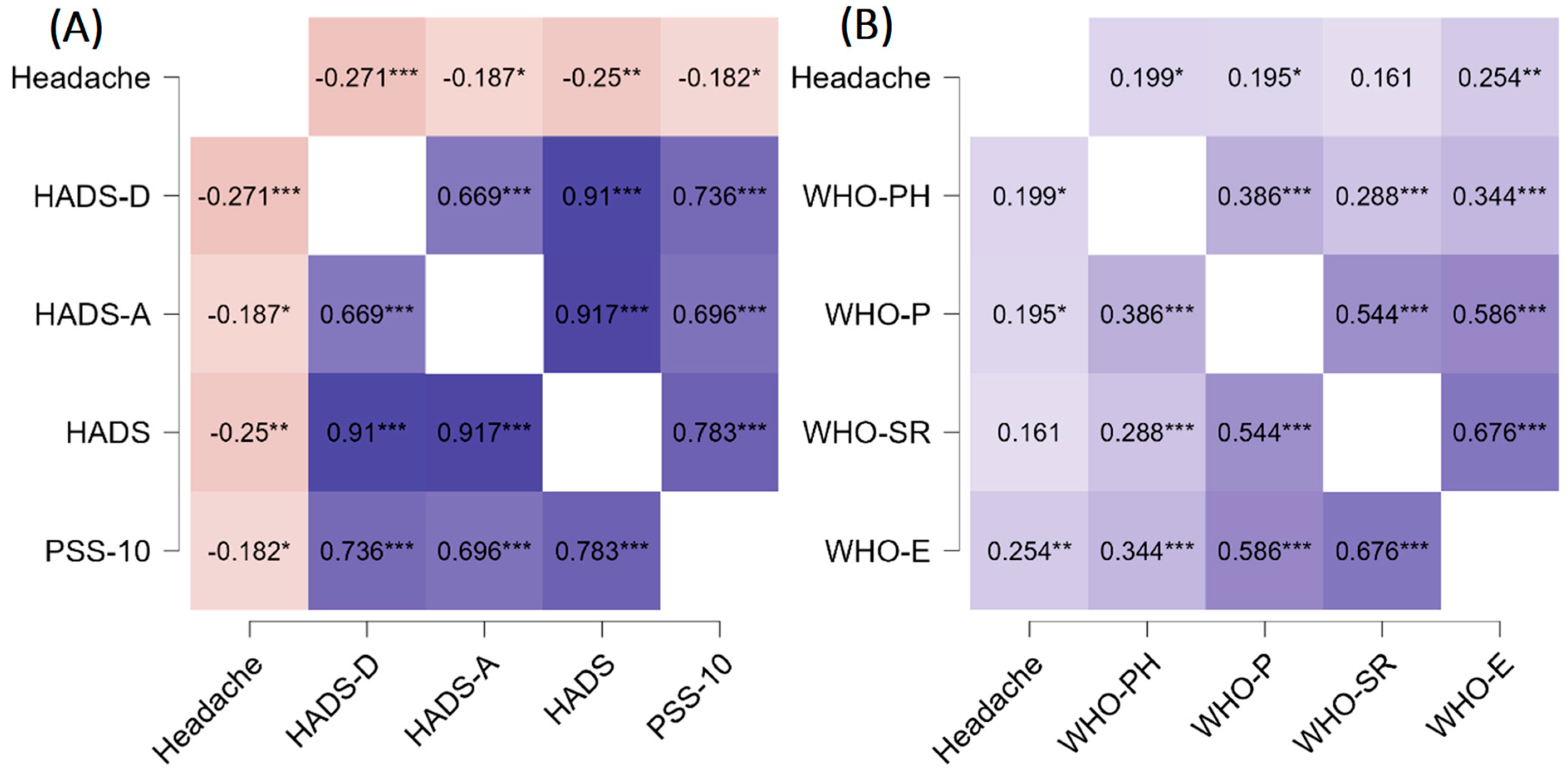
3.3. Correlations in the Data Set
3.4. Predictors
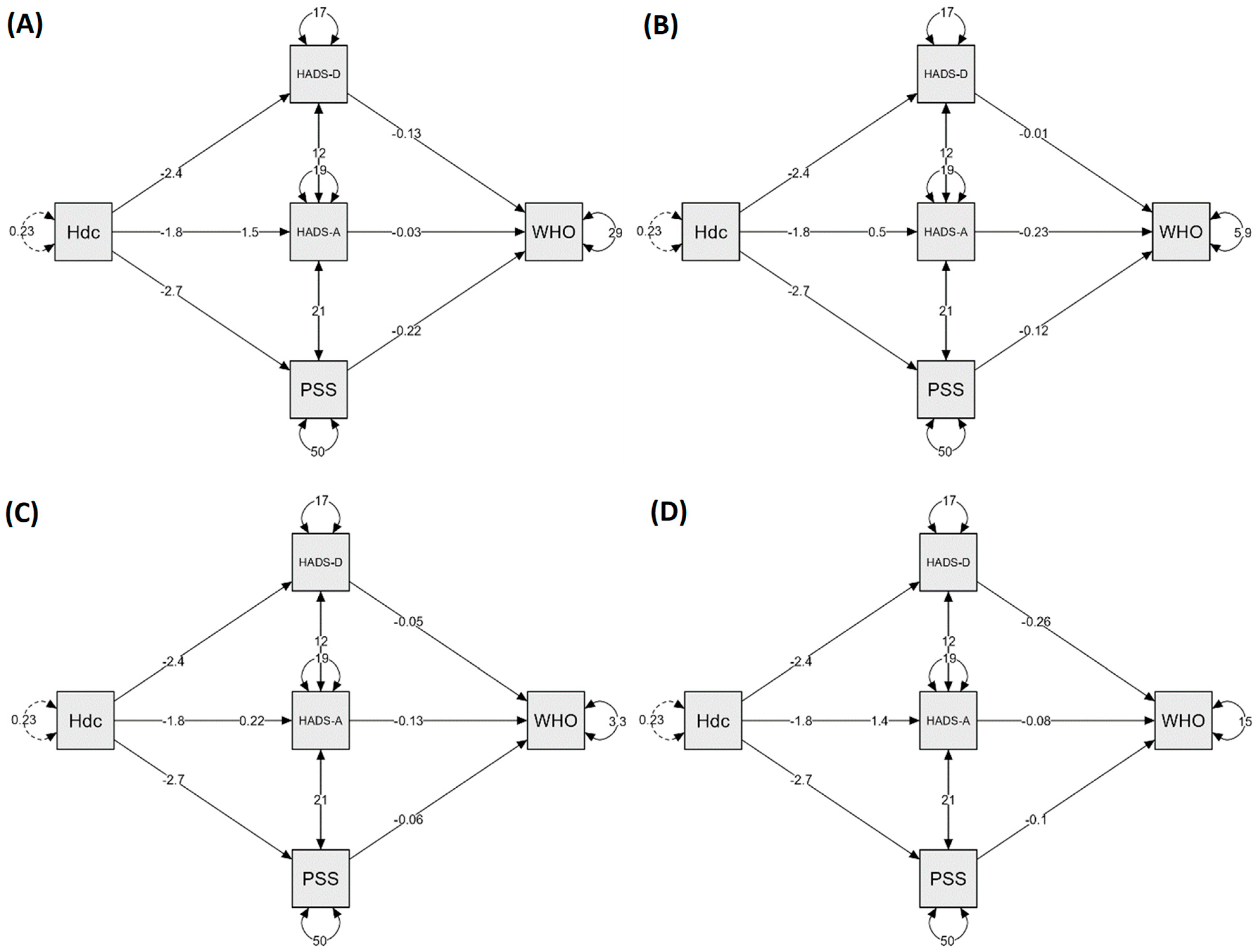
3.5. Mediation Analysis
4. Discussion
4.1. Limitation
4.2. Open Questions and Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed]
- García-Azorín, D.; Sierra, Á.; Trigo, J.; Alberdi, A.; Blanco, M.; Calcerrada, I.; Cornejo, A.; Cubero, M.; Gil, A.; García-Iglesias, C.; et al. Frequency and Phenotype of Headache in Covid-19: A Study of 2194 Patients. Sci. Rep. 2021, 11, 14674. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Hospitalizations. Available online: https://gis.cdc.gov/grasp/covidnet/covid19_5.html (accessed on 10 May 2022).
- Pinzon, R.T.; Wijaya, V.O.; Buana, R.B.; Al Jody, A.; Nunsio, P.N. Neurologic Characteristics in Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 565. [Google Scholar] [CrossRef] [PubMed]
- Bolay, H.; Gül, A.; Baykan, B. COVID-19 Is a Real Headache! Headache 2020, 60, 1415–1421. [Google Scholar] [CrossRef]
- Moro, E.; Priori, A.; Beghi, E.; Helbok, R.; Campiglio, L.; Bassetti, C.L.; Bianchi, E.; Maia, L.F.; Ozturk, S.; Cavallieri, F.; et al. The International European Academy of Neurology Survey on Neurological Symptoms in Patients with COVID-19 Infection. Eur. J. Neurol. 2020, 27, 1727–1737. [Google Scholar] [CrossRef]
- Magdy, R.; Hussein, M.; Ragaie, C.; Abdel-Hamid, H.M.; Khallaf, A.; Rizk, H.I.; Dahshan, A. Characteristics of Headache Attributed to COVID-19 Infection and Predictors of Its Frequency and Intensity: A Cross Sectional Study. Cephalalgia 2020, 40, 1422–1431. [Google Scholar] [CrossRef]
- Rocha-Filho, P.A.S.; Magalhães, J.E. Headache Associated with COVID-19: Frequency, Characteristics and Association with Anosmia and Ageusia. Cephalalgia 2020, 40, 1443–1451. [Google Scholar] [CrossRef]
- CDC Coronavirus Disease 2019 (COVID-19)—Symptoms. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 10 May 2022).
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition (Beta Version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef]
- De Marinis, M.; Welch, K.M. Headache Associated with Non-Cephalic Infections: Classification and Mechanisms. Cephalalgia 1992, 12, 197–201. [Google Scholar] [CrossRef]
- Tirozzi, A.; Santonastaso, F.; de Gaetano, G.; Iacoviello, L.; Gialluisi, A. Does COVID-19 Increase the Risk of Neuropsychiatric Sequelae? Evidence from a Mendelian Randomization Approach. World J. Psychiatry 2022, 12, 536–540. [Google Scholar] [CrossRef]
- Yuan, K.; Zheng, Y.-B.; Wang, Y.-J.; Sun, Y.-K.; Gong, Y.-M.; Huang, Y.-T.; Chen, X.; Liu, X.-X.; Zhong, Y.; Su, S.-Z.; et al. A Systematic Review and Meta-Analysis on Prevalence of and Risk Factors Associated with Depression, Anxiety and Insomnia in Infectious Diseases, Including COVID-19: A Call to Action. Mol. Psychiatry 2022, 1–9. [Google Scholar] [CrossRef]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Ognyanova, K.; Santillana, M.; Baum, M.A.; Lazer, D.; Druckman, J.; Della Volpe, J. Association of Acute Symptoms of COVID-19 and Symptoms of Depression in Adults. JAMA Netw. Open 2021, 4, e213223. [Google Scholar] [CrossRef]
- Lampl, C.; Thomas, H.; Tassorelli, C.; Katsarava, Z.; Laínez, J.M.; Lantéri-Minet, M.; Rastenyte, D.; Ruiz de la Torre, E.; Stovner, L.J.; Andrée, C.; et al. Headache, Depression and Anxiety: Associations in the Eurolight Project. J. Headache Pain 2016, 17, 59. [Google Scholar] [CrossRef]
- Ljubisavljevic, M.; Ignjatovic, A.; Djordjevic, V.; Pesic, M.H.; Ljubisavljevic, S. Depression, Anxiety, Stress, and Health-Related Quality of Life Among Patients With Medication Overuse Headache in a Tertiary Headache Center: A Cross-Sectional Study. J. Neuropsychiatry Clin. Neurosci. 2021, 33, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Palacios-Ceña, D.; Florencio, L.L.; Guerrero, A.L.; García-Azorín, D.; Hernández-Barrera, V.; Arendt-Nielsen, L. The Presence of Headache at Onset in SARS-CoV-2 Infection Is Associated with Long-Term Post-COVID Headache and Fatigue: A Case-Control Study. Cephalalgia 2021, 41, 1332–1341. [Google Scholar] [CrossRef]
- Silva Andrade, B.; Siqueira, S.; de Assis Soares, W.R.; de Souza Rangel, F.; Santos, N.O.; Dos Santos Freitas, A.; Ribeiro da Silveira, P.; Tiwari, S.; Alzahrani, K.J.; Góes-Neto, A.; et al. Long-COVID and Post-COVID Health Complications: An Up-to-Date Review on Clinical Conditions and Their Possible Molecular Mechanisms. Viruses 2021, 13, 700. [Google Scholar] [CrossRef]
- Caronna, E.; Alpuente, A.; Torres-Ferrus, M.; Pozo-Rosich, P. Toward a Better Understanding of Persistent Headache after Mild COVID-19: Three Migraine-like yet Distinct Scenarios. Headache 2021, 61, 1277–1280. [Google Scholar] [CrossRef]
- Caronna, E.; Ballvé, A.; Llauradó, A.; Gallardo, V.J.; Ariton, D.M.; Lallana, S.; López Maza, S.; Olivé Gadea, M.; Quibus, L.; Restrepo, J.L.; et al. Headache: A Striking Prodromal and Persistent Symptom, Predictive of COVID-19 Clinical Evolution. Cephalalgia 2020, 40, 1410–1421. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Navarro-Santana, M.; Gómez-Mayordomo, V.; Cuadrado, M.L.; García-Azorín, D.; Arendt-Nielsen, L.; Plaza-Manzano, G. Headache as an Acute and Post-COVID-19 Symptom in COVID-19 Survivors: A Meta-Analysis of the Current Literature. Eur. J. Neurol. 2021, 28, 3820–3825. [Google Scholar] [CrossRef]
- Al-Hashel, J.Y.; Abokalawa, F.; Alenzi, M.; Alroughani, R.; Ahmed, S.F. Coronavirus Disease-19 and Headache; Impact on Pre-Existing and Characteristics of de Novo: A Cross-Sectional Study. J. Headache Pain 2021, 22, 97. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The Validity of the Hospital Anxiety and Depression Scale. An Updated Literature Review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A.; WHOQOL Group. The World Health Organization’s WHOQOL-BREF Quality of Life Assessment: Psychometric Properties and Results of the International Field Trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Hatmi, Z.N. A Systematic Review of Systematic Reviews on the COVID-19 Pandemic. SN Compr. Clin. Med. 2021, 3, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Martelletti, P.; Bentivegna, E.; Spuntarelli, V.; Luciani, M. Long-COVID Headache. SN Compr. Clin. Med. 2021, 3, 1704–1706. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and Predictors of PTSS during COVID-19 Outbreak in China Hardest-Hit Areas: Gender Differences Matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef]
- Lipton, R.B.; Bigal, M.E. Migraine: Epidemiology, Impact, and Risk Factors for Progression. Headache J. Head Face Pain 2005, 45, S3–S13. [Google Scholar] [CrossRef]
- Baykan, B.; Ertas, M.; Karli, N.; Akat-Aktas, S.; Uzunkaya, O.; Zarifoglu, M.; Siva, A.; Saip, S.; MIRA-Neurology Study Group. The Burden of Headache in Neurology Outpatient Clinics in Turkey. Pain Pract. 2007, 7, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Pavlović, J.M. Headache in Women. Continuum 2021, 27, 686–702. [Google Scholar] [CrossRef] [PubMed]
- Bolay, H.; Ozge, A.; Saginc, P.; Orekici, G.; Uludüz, D.; Yalın, O.; Siva, A.; Bıçakçi, Ş.; Karakurum, B.; Öztürk, M. Gender Influences Headache Characteristics with Increasing Age in Migraine Patients. Cephalalgia 2015, 35, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.; Rizzoli, P.; Loder, E. The Prevalence and Impact of Migraine and Severe Headache in the United States: Updated Age, Sex, and Socioeconomic-Specific Estimates from Government Health Surveys. Headache 2021, 61, 60–68. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 147) | Participants with Headache (n = 96) | Participants without Headache (n = 51) | p Value * | |
|---|---|---|---|---|
| Gender, n (%) | ||||
| Female | 83 (56.46) | 66 (68.75) | 17 (33.33) | <0.001 |
| Male | 64 (43.54) | 30 (31.25) | 34 (66.67) | |
| Age, years, mean (SD) | 56.97 (9.86) | 55.47 (9.65) | 59.78 (9.72) | 0.01 |
| Body mass, kg, mean (SD) | 83.69 (17.07) | 82.14 (18.79) | 86.59 (12.95) | 0.02 |
| Body height, cm, mean (SD) | 168.13 (12.41) | 167.28 (7.51) | 171.67 (10.67) | 0.01 |
| BMI, mean (SD) | 29.28 (5.12) | 29.21 (5.70) | 29.42 (3.86) | 0.38 |
| Professional activity years, n (%) | 31.10 (9.08) | 29.94 (9.37) | 33.33 (8.13) | 0.041 |
| Education, n (%) | ||||
| Basic/vocational | 17 (11.56) | 9 (9.38) | 8 (15.69) | 0.10 |
| Secondary | 59 (40.14) | 34 (35.42) | 25 (49.02) | |
| Higher education | 68 (46.26) | 50 (52.08) | 18 (35.29) | |
| Missing | 3 (2.04) | 3 (3.13) | 0 (0.00) | |
| Current employment status, n (%) | ||||
| Professionally active | 96 (65.31) | 68 (70.83) | 28 (54.90) | 0.09 |
| Retirement | 42 (28.57) | 22 (22.92) | 20 (39.22) | |
| Sickness pension | 8 (5.44) | 6 (6.25) | 2 (3.92) | |
| Missing | 1 (0.68) | 0 (0.00) | 1 (1.96) | |
| Marital status, n (%) | ||||
| Married | 104 (70.75) | 64 (66.67) | 40 (78.43) | 0.28 |
| Single | 12 (8.16) | 10 (10.42) | 2 (3.92) | |
| Divorced | 15 (10.20) | 12 (12.50) | 3 (5.88) | |
| Widow | 11 (7.48) | 7 (7.29) | 4 (7.84) | |
| Missing | 5 (3.40) | 3 (3.13) | 2 (3.92) | |
| Type of profession, n (%) | ||||
| Intellectual | 51 (34.69) | 36 (37.50) | 15 (29.41) | 0.055 |
| Physical | 36 (24.49) | 18 (18.75) | 18 (35.29) | |
| Mixed | 39 (26.53) | 29 (30.21) | 10 (19.61) | |
| Missing | 21 (14.29) | 13 (13.54) | 8 (15.69) | |
| Hypertension, n (%) | ||||
| Yes | 70 (47.62) | 37 (38.54) | 33 (64.71) | 0.002 |
| No | 73 (49.66) | 56 (58.33) | 17 (33.33) | |
| Missing | 4 (2.72) | 3 (3.13) | 1 (1.96) | |
| Diabetes, n (%) | ||||
| Yes | 29 (19.73) | 18 (18.75) | 11 (21.57) | 0.64 |
| No | 117 (79.59) | 78 (81.25) | 39 (76.47) | |
| Missing | 1 (0.68) | 0 (0.00) | 1 (1.96) | |
| Subjective view of patient health before COVID-19, n (%) | ||||
| Good | 100 (68.03) | 62 (64.58) | 38 (1.96) | 0.48 |
| Neither good nor bad | 41 (27.89) | 29 (30.21) | 12 (23.53) | |
| Bad | 5 (3.40) | 4 (4.17) | 1 (1.96) | |
| Missing | 1 (0.68) | 1 (1.04) | 0 (0.00) | |
| Subjective view of the current patient’s health, n (%) | ||||
| Good | 11 (7.48) | 5 (5.21) | 6 (11.76) | 0.037 |
| Neither good nor bad | 99 (67.35) | 61 (63.54) | 38 (74.51) | |
| Bad | 37 (25.17) | 30 (31.25) | 7 (13.73) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Physical activity before COVID-19, n (%) | ||||
| Yes | 104 (70.75) | 69 (71.88) | 35 (68.63) | 0.68 |
| No | 43 (29.25) | 27 (28.13) | 16 (31.37) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| COVID-19 treatment in, n (%) | ||||
| Home | 65 (44.22) | 53 (55.21) | 12 (23.53) | <0.001 |
| Hospital | 81 (55.10) | 42 (43.75) | 39 (76.47) | |
| Missing | 1 (0.68) | 1 (1.04) | 0 (0.00) | |
| Need for oxygen therapy, n (%) | ||||
| Yes | 81 (55.10) | 46 (47.92) | 35 (68.63) | 0.01 |
| No | 66 (44.90) | 50 (52.08) | 16 (31.37) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Subjective view of the intensity of the COVID-19 symptoms, n (%) | ||||
| Asymptomatic | 2 (1.36) | 1 (1.04) | 1 (1.96) | 0.18 |
| Mild | 9 (6.12) | 3 (3.13) | 6 (11.76) | |
| Moderate | 44 (29.93) | 31 (32.29) | 13 (25.49) | |
| Severe | 92 (62.59) | 61 (63.54) | 31 (60.78) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Abdominal pain during COVID-19, n (%) | ||||
| Yes | 37 (25.17) | 31 (32.29) | 6 (11.76) | 0.006 |
| No | 110 (74.83) | 65 (67.71) | 45 (88.24) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Muscle pain during COVID-19, n (%) | ||||
| Yes | 108 (73.47) | 82 (85.43) | 26 (50.98) | <0.001 |
| No | 39 (26.54) | 14 (14.58) | 25 (49.02) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Loss of smell and taste during COVID-19, n (%) | ||||
| Yes | 90 (61.22) | 67 (69.79) | 23 (45.10) | 0.003 |
| No | 57 (38.78) | 29 (30.21) | 28 (54.90) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Other symptoms, n (%) | ||||
| None | 73 (49.66) | 41 (42.71) | 32 (62.75) | 0.23 |
| Hair loss | 3 (2.04) | 3 (3.13) | 0 (0.00) | |
| Diarrhea/vomiting | 15 (10.20) | 12 (12.50) | 3 (5.88) | |
| Dyspnea | 16 (10.88) | 10 (10.42) | 6 (11.76) | |
| Weakness | 18 (12.24) | 14 (14.58) | 4 (7.84) | |
| Nonspecific pain | 21 (14.29) | 15 (15.63) | 6 (11.76) | |
| Skin rash | 1 (0.68) | 1 (1.04) | 0 (0.00) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Persisting pulmonary complications, n (%) | ||||
| Yes | 126 (85.71) | 83 (86.46) | 43 (84.31) | 0.72 |
| No | 21 (14.29) | 13 (13.54) | 8 (15.69) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Persisting cardiac complications, n (%) | ||||
| Yes | 38 (25.85) | 27 (28.13) | 11 (21.57) | 0.39 |
| No | 109 (74.15) | 69 (71.88) | 40 (78.43) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Persisting neurological complications, n (%) | ||||
| Yes | 54 (36.73) | 43 (44.79) | 11 (21.57) | 0.005 |
| No | 93 (63.27) | 53 (55.21) | 40 (78.43) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Persisting mental complications, n (%) | ||||
| Yes | 64 (43.54) | 47 (48.96) | 17 (33.33) | 0.07 |
| No | 83 (56.46) | 49 (51.04) | 34 (66.67) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Persisting other complications, n (%) | ||||
| Brak | 104 (70.75) | 68 (70.83) | 36 (70.59) | 0.60 |
| Hair loss | 5 (3.40) | 4 (4.17) | 1 (1.96) | |
| Diarrhea/vomiting | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Dyspnea | 1 (0.68) | 1 (1.04) | 0 (0.00) | |
| Weakness | 14 (9.52) | 8 (8.33) | 6 (11.76) | |
| Nonspecific pain | 16 (10.88) | 9 (9.38) | 7 (13.73) | |
| Skin rash | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Memory loss | 7 (4.76) | 6 (6.25) | 1 (1.96) | |
| Missing | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Participants with Headache (n = 96) | Participants without Headache (n = 51) | Mean Diff. | t | Cohen’s d | p Value | |||
|---|---|---|---|---|---|---|---|---|
| Variable | Mean | SD | Mean | SD | ||||
| HADS total | 17.07 | 8.27 | 12.90 | 6.67 | 4.17 | 3.33 | 0.55 | 0.001 |
| HADS-D | 8.90 | 4.42 | 6.47 | 3.54 | 2.43 | 3.39 | 0.61 | <0.001 |
| HADS-A | 8.18 | 4.65 | 6.43 | 3.87 | 1.75 | 2.29 | 0.41 | 0.023 |
| PSS-10 | 20.25 | 7.59 | 17.51 | 6.08 | 2.74 | 2.23 | 0.40 | 0.028 |
| WHOQOL-BREF domains | ||||||||
| Physical health | 19.77 | 6.78 | 22.22 | 3.07 | −2.45 | −2.44 | 0.46 | 0.016 |
| Psychological | 19.81 | 3.23 | 21.06 | 2.51 | −1.25 | −2.40 | 0.43 | 0.018 |
| Social relationships | 10.97 | 2.35 | 11.69 | 1.53 | −0.72 | −1.97 | 0.36 | 0.051 |
| Environmental | 27.80 | 4.59 | 30.20 | 3.94 | −2.39 | −3.16 | 0.56 | 0.002 |
| Variable | B | Beta | t | p Value | F | R2 |
|---|---|---|---|---|---|---|
| HADS-D | 0.01 | 8.64 | 0.11 | |||
| Gender | −1.69 | −0.20 | −2.34 | |||
| Headache | −1.83 | −0.20 | −2.44 | |||
| HADS-A | 0.023 | 5.26 | 0.04 | |||
| Headache | −1.75 | −0.19 | −2.29 | |||
| HADS | 0.002 | 6.53 | 0.07 | |||
| Gender | −2.48 | −0.15 | −1.81 | |||
| Headache | −3.30 | −0.20 | −2.33 | |||
| PSS-10 | −2.74 | −0.18 | −2.23 | 0.001 | 12.28 | 0.08 |
| Gender | −4.05 | −0.28 | −3.50 |
| Total Effect | Direct Effect | Indirect Effect | Percentage Mediation | ||||
|---|---|---|---|---|---|---|---|
| Variable | Effect Size (95% CI) | p Value | Effect Size (95% CI) | p Value | Effect Size (95% CI) | p Value | |
| Physical health | 2.44 (0.50, 4.39) | 0.01 | 1.48 (−0.41, 3.37) | 0.12 | 0.96 (0.10, 1.83) | 0.03 | 39.34 |
| Psychological | 1.25 (0.23, 2.26) | 0.02 | 0.50 (−0.36, 1.36) | 0.26 | 0.75 (0.12, 1.38) | 0.02 | 60.00 |
| Social relationships | 0.72 (0.01, 1.43) | 0.04 | 0.22 (−0.42, 0.87) | 0.49 | 0.49 (0.10, 0.88) | 0.01 | 68.06 |
| Environmental | 2.39 (0.92, 3.87) | 0.001 | 1.35 (−0.03, 2.73) | 0.05 | 1.04 (0.29, 1.79) | 0.006 | 43.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurek, J.; Cieślik, B.; Szary, P.; Rutkowski, S.; Szczegielniak, J.; Szczepańska-Gieracha, J.; Gajda, R. Association of Acute Headache of COVID-19 and Anxiety/Depression Symptoms in Adults Undergoing Post-COVID-19 Rehabilitation. J. Clin. Med. 2022, 11, 5002. https://doi.org/10.3390/jcm11175002
Mazurek J, Cieślik B, Szary P, Rutkowski S, Szczegielniak J, Szczepańska-Gieracha J, Gajda R. Association of Acute Headache of COVID-19 and Anxiety/Depression Symptoms in Adults Undergoing Post-COVID-19 Rehabilitation. Journal of Clinical Medicine. 2022; 11(17):5002. https://doi.org/10.3390/jcm11175002
Chicago/Turabian StyleMazurek, Justyna, Błażej Cieślik, Patryk Szary, Sebastian Rutkowski, Jan Szczegielniak, Joanna Szczepańska-Gieracha, and Robert Gajda. 2022. "Association of Acute Headache of COVID-19 and Anxiety/Depression Symptoms in Adults Undergoing Post-COVID-19 Rehabilitation" Journal of Clinical Medicine 11, no. 17: 5002. https://doi.org/10.3390/jcm11175002