
New Insights on the Minimal-Invasive Therapy of Cervical Cancer

 ,
,
Abstract
:1. Introduction
2. Data before 2018
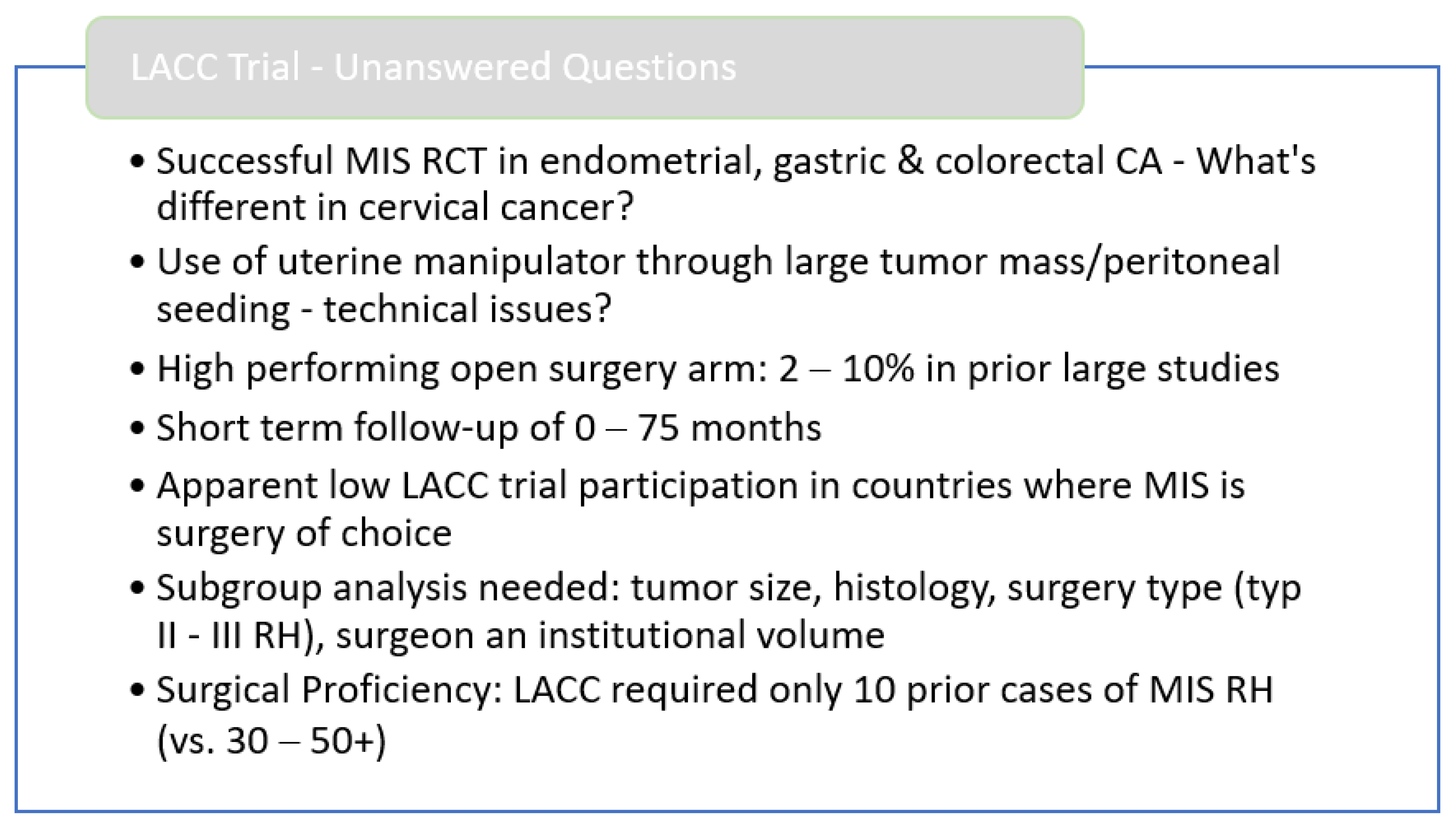
3. The LACC-Trial
4. Data after 2018
5. Theoretical Considerations
- (1)
- The CO2-Theory.
- (2)
- The most interesting critical point has been the theory that during a laparoscopic (or robotic) procedure, it is not possible to completely “isolate” the tumor mass from the abdominal cavity, allowing for the mechanical “entry” of cancer cells into the peritoneal cavity.
- (3)
- One of the most significant points of discussion is whether the cutoff of two centimeters is real. Again, different publications tell different stories. Although the original publications of the LACC trial and the epidemiological study of Alexander Melamed MD, MPH clearly see a cutoff at 2 cm and further studies from other centers seem to confirm this [37,38,39], other retrospective studies have failed to find such a limit [29,40].
6. Moral Considerations
7. Ongoing Studies
8. Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, T.; Zaitsu, M.; Oki, I.; Haruyama, Y.; Nishida, K.; Uchiyama, K.; Sairenchi, T.; Kobashi, G. Recent Increasing Incidence of Early-Stage Cervical Cancers of the Squamous Cell Carcinoma Subtype among Young Women. Int. J. Environ. Res. Public Health 2020, 17, 7401. [Google Scholar] [CrossRef] [PubMed]
- Cezar, C.; Becker, S.; di Spiezio Sardo, A.; Herrmann, A.; Larbig, A.; Tanos, V.; De La Roche, L.A.T.; Verhoeven, H.C.; Wallwiener, M.; De Wilde, R.L. Laparoscopy or laparotomy as the way of entrance in myoma enucleation. Arch. Gynecol. Obstet. 2017, 296, 709–720. [Google Scholar] [CrossRef]
- Panico, G.; Campagna, G.; Vacca, L.; Caramazza, D.; Iannone, V.; Rossitto, C.; Rumolo, V.; Scambia, G.; Ercoli, A. Minimally invasive surgery in urogynecology: A comparison of standard laparoscopic, minilaparoscopic, percutaneous surgical system, and robotic sacral colpopexy. Minerva Med. 2021, 112, 483–491. [Google Scholar] [CrossRef]
- Cusimano, M.C.; Simpson, A.N.; Dossa, F.; Liani, V.; Kaur, Y.; Acuna, S.A.; Robertson, D.; Satkunaratnam, A.; Bernardini, M.Q.; Ferguson, S.E.; et al. Laparoscopic and robotic hysterectomy in endometrial cancer patients with obesity: A systematic review and meta-analysis of conversions and complications. Am. J. Obstet. Gynecol. 2019, 221, 410–428.e19. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, M.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Zaccarini, F.; Santy, A.; Dabi, Y.; Lavoue, V.; Carcopino, X.; Bendifallah, S.; Benbara, A.; Collinet, P.; Canlorbe, G.; Raimond, E.; et al. Comparison of survival outcomes between laparoscopic and abdominal radical hysterectomy for early-stage cervical cancer: A French multicentric study. J. Gynecol. Obstet Hum. Reprod. 2021, 50, 102046. [Google Scholar] [CrossRef]
- Kelley, W.E. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. J. Soc. Laparoendosc. Surg. 2008, 12, 351–357. [Google Scholar]
- Nezhat, F.R.; Sirota, I. Perioperative outcomes of robotic assisted laparoscopic surgery versus conventional laparoscopy surgery for advanced-stage endometriosis. J. Soc. Laparoendosc. Surg. 2014, 18, e2014.00094. [Google Scholar] [CrossRef] [Green Version]
- Conrad, L.B.; Ramirez, P.T.; Burke, W.; Naumann, R.W.; Ring, K.L.; Munsell, M.F.; Frumovitz, M. Role of Minimally Invasive Surgery in Gynecologic Oncology: An Updated Survey of Members of the Society of Gynecologic Oncology. Int. J. Gynecol. Cancer 2015, 25, 1121–1127. [Google Scholar] [CrossRef]
- Gil-Moreno, A.; Carbonell-Socias, M.; Salicrú, S.; Centeno-Mediavilla, C.; Franco-Camps, S.; Colas, E.; Oaknin, A.; Pérez-Benavente, A.; Díaz-Feijoo, B. Radical Hysterectomy: Efficacy and Safety in the Dawn of Minimally Invasive Techniques. J. Minim. Invasive Gynecol. 2019, 26, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Bafort, C.; Beebeejaun, Y.; Tomassetti, C.; Bosteels, J.; Duffy, J.M. Laparoscopic surgery for endometriosis. Cochrane Database Syst. Rev. 2020, 10, CD011031. [Google Scholar] [CrossRef]
- Holloway, R.W.; Abu-Rustum, N.R.; Backes, F.J.; Boggess, J.F.; Gotlieb, W.H.; Lowery, W.J.; Rossi, E.C.; Tanner, E.J.; Wolsky, R.J. Sentinel lymph node mapping and staging in endometrial cancer: A Society of Gynecologic Oncology literature review with consensus recommendations. Gynecol Oncol. 2017, 146, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Knisely, A.; Gamble, C.R.; St Clair, C.M.; Panico, G.; Campagna, G.; Vacca, L.; Caramazza, D.; Iannone, V.; Rossitto, C.; Rumolo, V.; et al. The Role of Minimally Invasive Surgery in the Care of Women with Ovarian Cancer: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Papadia, A.; Garbade, A.; Gasparri, M.L.; Wang, J.; Radan, A.P.; Mueller, M.D. Minimally invasive surgery does not impair overall survival in stage IIIC endometrial cancer patients. Arch. Gynecol. Obstet. 2020, 301, 585–590. [Google Scholar] [CrossRef]
- Gala, R.B.; Margulies, R.; Steinberg, A.; Murphy, M.; Lukban, J.; Jeppson, P.; Aschkenazi, S.; Olivera, C.; South, M.; Lowenstein, L.; et al. Systematic review of robotic surgery in gynecology: Robotic techniques compared with laparoscopy and laparotomy. J. Minim. Invasive Gynecol. 2014, 21, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Twijnstra, A.R.H.; Kolkman, W.; Trimbos-Kemper, G.C.M.; Jansen, F.W. Implementation of advanced laparoscopic surgery in gynecology: National overview of trends. J. Minim. Invasive Gynecol. 2010, 17, 487–492. [Google Scholar] [CrossRef]
- Cho, J.E.; Shamshirsaz, A.H.A.; Nezhat, C.; Nezhat, C.; Nezhat, F. New technologies for reproductive medicine: Laparoscopy, endoscopy, robotic surgery and gynecology. A review of the literature. Minerva Ginecol. 2010, 62, 137–167. [Google Scholar]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Meder, C.H.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 127, 404–416. [Google Scholar] [CrossRef]
- Wallin, E.; Flöter Rådestad, A.; Falconer, H. Introduction of robot-assisted radical hysterectomy for early stage cervical cancer: Impact on complications, costs and oncologic outcome. Acta Obstet. Gynecol. Scand. 2017, 96, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sert, B.M.; Boggess, J.F.; Ahmad, S.; Jackson, A.; Stavitzski, N.; Dahl, A.; Holloway, R. Robot-assisted versus open radical hysterectomy: A multi-institutional experience for early-stage cervical cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2016, 42, 513–522. [Google Scholar] [CrossRef]
- Zanagnolo, V.; Minig, L.; Rollo, D.; Tomaselli, T.; Aletti, G.; Bocciolone, L.; Landoni, F.; Rebollo, J.M.C.; Maggioni, A. Clinical and Oncologic Outcomes of Robotic Versus Abdominal Radical Hysterectomy for Women With Cervical Cancer: Experience at a Referral Cancer Center. Int. J. Gynecol. Cancer 2016, 26, 568–574. [Google Scholar] [CrossRef]
- Cibula, D.; Pinkavova, I.; Dusek, L.; Slama, J.; Zikan, M.; Fischerová, D.; Freitag, P.; Dundr, P. Local control after tailored surgical treatment of early cervical cancer. Int. J. Gynecol. Cancer 2011, 21, 690–698. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M.; Horn, L.C.; Manthey, M.; Braumann, U.D.; Wolf, U.; Teichmann, G.; Frauenschläger, K.; Dornhöfer, N.; Einenkel, J. Resection of the embryologically defined uterovaginal (Müllerian) compartment and pelvic control in patients with cervical cancer: A prospective analysis. Lancet Oncol. 2009, 10, 683–692. [Google Scholar] [CrossRef]
- Nie, J.C.; Yan, A.Q.; Liu, X.S. Robotic-Assisted Radical Hysterectomy Results in Better Surgical Outcomes Compared With the Traditional Laparoscopic Radical Hysterectomy for the Treatment of Cervical Cancer. Int. J. Gynecol. Cancer 2017, 27, 1990–1999. [Google Scholar] [CrossRef]
- Chiantera, V.; Vizzielli, G.; Lucidi, A.; Gallotta, V.; Petrillo, M.; Legge, F.; Fagotti, A.; Sehouli, J.; Scambia, G.; Muallem, M.Z. Laparoscopic radical hysterectomy in cervical cancer as total mesometrial resection (L-TMMR): A multicentric experience. Gynecol. Oncol. 2015, 139, 47–51. [Google Scholar] [CrossRef]
- Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Arévalo-Serrano, J.; Căpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. SUCCOR study: An international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1269–1277. [Google Scholar] [CrossRef]
- Chen, X.; Zhao, N.; Ye, P.; Chen, J.; Nan, X.; Zhao, H.; Zhou, K.; Zhang, Y.; Xue, J.; Zhou, H.; et al. Comparison of laparoscopic and open radical hysterectomy in cervical cancer patients with tumor size ≤2 cm. Int J. Gynecol Cancer 2020, 30, 564–571. [Google Scholar] [CrossRef] [Green Version]
- Uppal, S.; Gehrig, P.A.; Peng, K.; Bixel, K.L.; Matsuo, K.; Vetter, M.H.; Rose, S.L.; Davidson, B.A.; Paige Cisa, M.; Brunette, L.L.; et al. Rose Recurrence Rates in Patients with Cervical Cancer Treated with Abdominal Versus Minimally Invasive Radical Hysterectomy: A Multi-Institutional Retrospective Review Study. J. Clin. Oncol. 2020, 38, 1030–1040. [Google Scholar] [CrossRef]
- Martin-Hirsch, P.; Wood, N.; Whitham, N.L.; Macdonald, R.; Kirwan, J.; Anagnostopoulos, A.; Hutson, R.; Theophilou, G.; Otify, M.; Smith, M.; et al. Survival of women with early-stage cervical cancer in the UK treated with minimal access and open surgery. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 956–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, P.T.; Schnack, T.H.; Frøding, L.P.; Bjørn, S.F.; Lajer, H.; Markauskas, A.; Jochumsen, K.M.; Fuglsang, K.; Dinesen, J.; Søgaard, C.H.; et al. Survival after a nationwide adoption of robotic minimally invasive surgery for early-stage cervical cancer-A population-based study. Eur. J. Cancer Oxf. Engl. 1990 2020, 128, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Brandt, B.; Sioulas, V.; Basaran, D.; Kuhn, T.; LaVigne, K.; Gardner, G.J.; Sonoda, Y.; Chi, D.S.; Roche, K.C.L.; Mueller, J.J.; et al. Minimally invasive surgery versus laparotomy for radical hysterectomy in the management of early-stage cervical cancer: Survival outcomes. Gynecol. Oncol. 2020, 156, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Pedone Anchora, L.; Bizzarri, N.; Gallotta, V.; Chiantera, V.; Fanfani, F.; Fagotti, A.; Cosentino, F.; Vizzielli, G.; Carbone, V.; Ferrandina, G.; et al. Impact of surgeon learning curve in minimally invasive radical hysterectomy on early stage cervical cancer patient survival. Facts Views Vis. Obgyn. 2021, 13, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Touhami, O.; Plante, M. Minimally Invasive Surgery for Cervical Cancer in Light of the LACC Trial: What Have We Learned? Curr. Oncol. Tor. Ont. 2022, 29, 1093–1106. [Google Scholar] [CrossRef] [PubMed]
- Torné, A.; Pahisa, J.; Ordi, J.; Fusté, P.; Díaz-Feijóo, B.; Glickman, A.; Paredes, P.; Rovirosa, A.; Gaba, L.; Saco, A.; et al. Oncological Results of Laparoscopically Assisted Radical Vaginal Hysterectomy in Early-Stage Cervical Cancer: Should We Really Abandon Minimally Invasive Surgery? Cancers 2021, 13, 846. [Google Scholar] [CrossRef] [PubMed]
- Nitecki, R.; Ramirez, P.T.; Frumovitz, M.; Krause, K.J.; Tergas, A.I.; Wright, J.D.; Rauh-Hain, J.A.; Melamed, A. Survival after minimally invasive vs open radical hysterectomy for early-stage cervical cancer: A systematic review and meta-analysis. JAMA Oncol. 2020, 6, 1019–1027. [Google Scholar] [CrossRef]
- Pedone Anchora, L.; Turco, L.C.; Bizzarri, N.; Capozzi, V.A.; Lombisani, A.; Chiantera, V.; De Felice, F.; Gallotta, V.; Cosentino, F.; Fagotti, A.; et al. How to Select Early-Stage Cervical Cancer Patients Still Suitable for Laparoscopic Radical Hysterectomy: A Propensity-Matched Study. Ann. Surg. Oncol. 2020, 27, 1947–1955. [Google Scholar] [CrossRef]
- Kim, S.I.; Lee, J.; Hong, J.; Lee, S.J.; Park, D.C.; Yoon, J.H. Comparison of abdominal and minimally invasive radical hysterectomy in patients with early stage cervical cancer. Int. J. Med. Sci. 2021, 18, 1312–1317. [Google Scholar] [CrossRef]
- Pareja, R. Safety of minimally invasive radical hysterectomy in cervical tumors <2 cm. Int. J. Gynecol. Cancer 2020, 30, 572–574. [Google Scholar] [CrossRef] [Green Version]
- Chao, X.; Li, L.; Wu, M.; Ma, S.; Tan, X.; Zhong, S.; Lang, J.; Cheng, A.; Li, W. Efficacy of different surgical approaches in the clinical and survival outcomes of patients with early-stage cervical cancer: Protocol of a phase III multicentre randomised controlled trial in China. BMJ Open 2019, 9, e029055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falconer, H.; Palsdottir, K.; Stalberg, K.; Dahm-Kähler, P.; Ottander, U.; Lundin, E.S.; Wijk, L.; Kimmig, R.; Jensen, P.T.; Eriksson, A.G.Z.; et al. Robot-assisted approach to cervical cancer (RACC): An international multi-center, open-label randomized controlled trial. Int. J. Gynecol. Cancer 2019, 29, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Marie Plante. The SHAPE Trial. Available online: http://www.gcig.igcs.org/Spring2012/2012_june_shape_trial.pdf (accessed on 26 January 2019).


{kind=link}
| Trial | Open | MIS/Robot | ||||
|---|---|---|---|---|---|---|
| N | Recurrences | RR (%) | N | Recurrences | RR (%) | |
| LACC 2018 | 312 | 7 | 2.2 | 319 | 24 | 7.5 |
| Shiah et al., 2017 | 202 | 21 | 10.4 | 109 | 11 | 10.1 |
| Wallin et al., 2017 | 155 | 16 | 10.3 | 149 | 20 | 13.4 |
| Sert et al., 2016 | 232 | 21 | 9.0 | 259 | 23 | 9.0 |
| Zanagnolo et al., 2016 | 104 | 11 | 10.6 | 203 | 18 | 8.8 |
| Laparotomy | Laparoscopy | ||
|---|---|---|---|
| Cibula et al., 2011 | Hockel et al., 2009 | Nie et al., 2017 | Chiantera et al., 2016 |
| IA-IIB | IB-IIB | IA1-IIA2 | IA2-IB1 |
| Radical hysterectomies | TMMR | Robot vs Laparoscopic RH | L-TMMR |
| Median FU 55 months | Median FU 41 months | Median FU: not reported | Median FU 18 months |
| 120 IB1 | 159 IB1–IIA (total 212) | IB1 592 | IB1: 61 |
| Adjuvant treatment 6.4% | Adjuvant treatment 3.7% (No RT) | Adjuvant treatment 40% robotic and 55% laparoscopic | Adjuvant treatment 36.6% |
| Recurrences in IB1: 3/120 (2.5%) | Recurrences 3/159 (1.9%) | Recurrences in 32/856 (3.7%) (0 recurrences in robotic arm) | Recurrences 2/71 (2.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasimli, K.; Wilhelm, L.; Becker, S.; De Wilde, R.L.; Tahmasbi Rad, M. New Insights on the Minimal-Invasive Therapy of Cervical Cancer. J. Clin. Med. 2022, 11, 4919. https://doi.org/10.3390/jcm11164919
Gasimli K, Wilhelm L, Becker S, De Wilde RL, Tahmasbi Rad M. New Insights on the Minimal-Invasive Therapy of Cervical Cancer. Journal of Clinical Medicine. 2022; 11(16):4919. https://doi.org/10.3390/jcm11164919
Chicago/Turabian StyleGasimli, Khayal, Lisa Wilhelm, Sven Becker, Rudy Leon De Wilde, and Morva Tahmasbi Rad. 2022. "New Insights on the Minimal-Invasive Therapy of Cervical Cancer" Journal of Clinical Medicine 11, no. 16: 4919. https://doi.org/10.3390/jcm11164919