
Comparison of the Postoperative Outcomes of the Mini-Flap Bilateral Axillo-Breast Approach (BABA) and Conventional BABA Robot-Assisted Thyroidectomy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
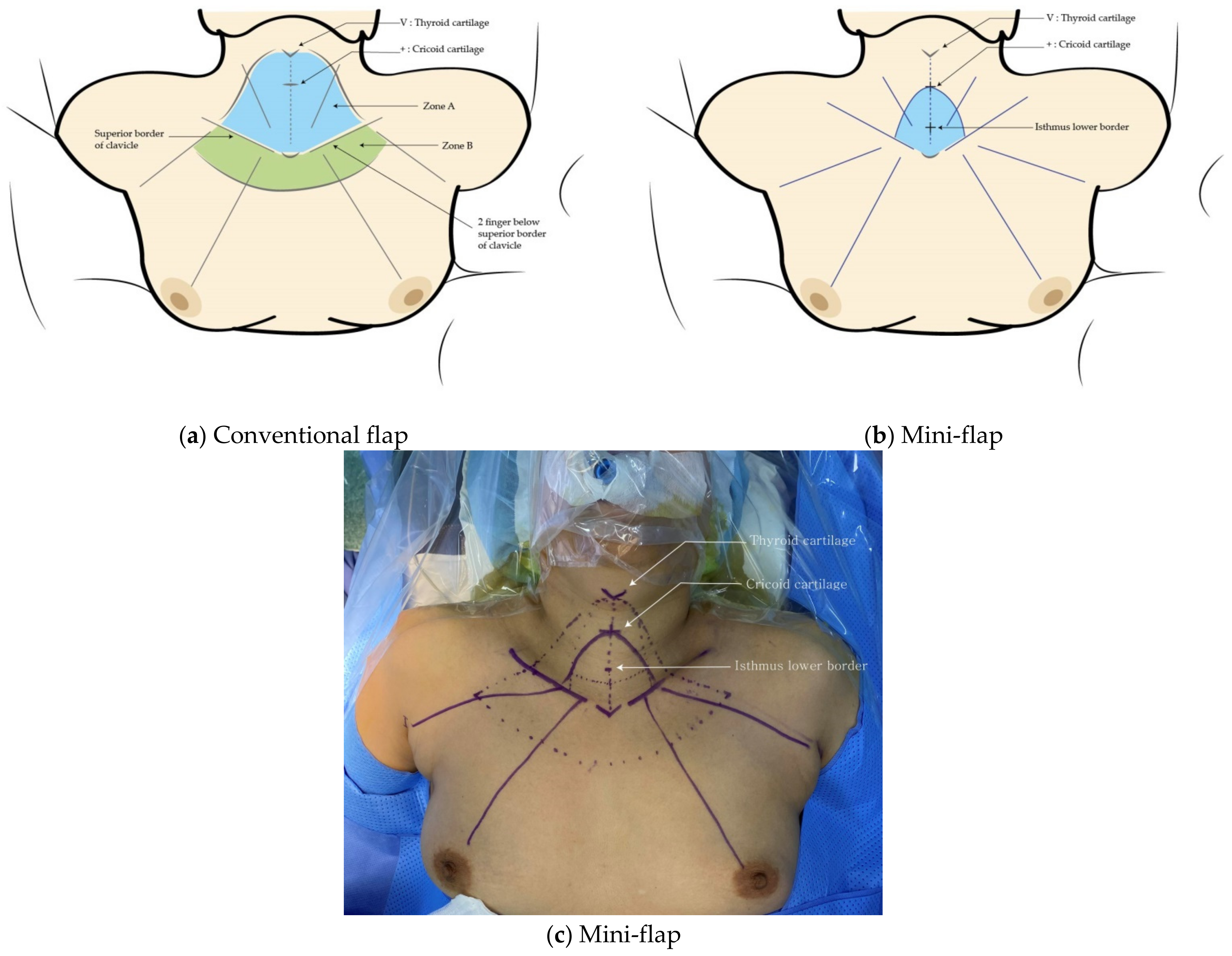
2.2. Surgical Procedure
2.3. Operative and Postoperative Outcome Measurements
2.4. Statistical Analysis
3. Results
3.1. Demographics and Pathological Outcomes
3.2. Clinical Outcomes
3.3. Surgical Outcomes
3.4. Oncological Outcomes
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hunter, J.G. Minimally invasive surgery: The next frontier. World J. Surg. 1999, 23, 422. [Google Scholar] [CrossRef] [PubMed]
- Dralle, H.; Machens, A.; Thanh, P.N. Minimally invasive compared with conventional thyroidectomy for nodular goitre. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 589–599. [Google Scholar] [CrossRef]
- Linos, D. Minimally invasive thyroidectomy: A comprehensive appraisal of existing techniques. Surgery 2011, 150, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.S.; Choe, J.-H.; Kang, K.-H.; Kim, S.W.; Chung, K.-W.; Park, K.S.; Han, W.; Noh, D.-Y.; Oh, S.K.; Youn, Y.-K. Endoscopic thyroidectomy for thyroid malignancies: Comparison with conventional open thyroidectomy. World J. Surg. 2007, 31, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, H.; Han, X.; Di, J.; Zheng, Q. Meta-analysis of comparison between minimally invasive video-assisted thyroidectomy and conventional thyroidectomy. Eur. Rev. Med. Pharm. Sci. 2015, 19, 1381–1387. [Google Scholar]
- Bokor, T.; Kiffner, E.; Kotrikova, B.; Billmann, F. Cosmesis and body image after minimally invasive or open thyroid surgery. World J. Surg. 2012, 36, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, K.E.; Chung, K.-W.; Kim, S.-W.; Choe, J.-H.; Koo, D.H.; Kim, S.-j.; Lee, J.; Chung, Y.S.; Oh, S.K. Endoscopic thyroidectomy via bilateral axillo-breast approach (BABA): Review of 512 cases in a single institute. Surg. Endosc. 2012, 26, 948–955. [Google Scholar] [CrossRef]
- Lee, K.E.; Rao, J.; Youn, Y.-K. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: Our initial experience. Surg. Laparosc. Endosc. Percutaneous Tech. 2009, 19, e71–e75. [Google Scholar] [CrossRef]
- Kim, S.-J.; Lee, K.E.; Myong, J.P.; Kwon, M.R.; Youn, Y.-K. Recovery of sensation in the anterior chest area after bilateral axillo-breast approach endoscopic/robotic thyroidectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2011, 21, 366–371. [Google Scholar] [CrossRef]
- Bae, D.S.; Kim, S.j.; Koo, D.H.; Paek, S.H.; Kwon, H.; Chai, Y.J.; Choi, J.Y.; Lee, K.E.; Youn, Y.K. Prospective, randomized controlled trial on use of ropivacaine after robotic thyroid surgery: Effects on postoperative pain. Head Neck 2016, 38, E588–E593. [Google Scholar] [CrossRef]
- Henry, J.F. Minimally invasive thyroid and parathyroid surgery is not a question of length of the incision. Langenbeck’s Arch. Surg. 2008, 393, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Choi, J.Y.; Youn, Y.-K. Bilateral axillo-breast approach robotic thyroidectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2011, 21, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.W.; Lee, Y.m.; Lee, Y.H.; Hong, S.J.; Yoon, J.H. Dynamic risk stratification system in post-lobectomy low-risk and intermediate-risk papillary thyroid carcinoma patients. Clin. Endocrinol. 2018, 89, 100–109. [Google Scholar] [CrossRef]
- Tae, K. Robotic thyroid surgery. Auris Nasus Larynx 2021, 48, 331–338. [Google Scholar] [CrossRef]
- Bae, D.S.; Koo, D.H.; Choi, J.Y.; Kim, E.; Lee, K.E.; Youn, Y.-K. Current status of robotic thyroid surgery in South Korea: A web-based survey. World J. Surg. 2014, 38, 2632–2639. [Google Scholar] [CrossRef]
- Bae, D.S.; Suh, B.J.; Park, J.K.; Koo, D.H. Technical, oncological, and functional safety of bilateral axillo-breast approach (BABA) robotic total thyroidectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, 253–258. [Google Scholar] [CrossRef]
- Yu, H.W.; Chai, Y.J.; Kim, S.-J.; Choi, J.Y.; Lee, K.E. Robotic-assisted modified radical neck dissection using a bilateral axillo-breast approach (robotic BABA MRND) for papillary thyroid carcinoma with lateral lymph node metastasis. Surg. Endosc. 2018, 32, 2322–2327. [Google Scholar] [CrossRef]
- Shan, L.; Liu, J. Meta-analysis comparison of bilateral axillo-breast approach robotic thyroidectomy and conventional thyroidectomy. Surg. Innov. 2019, 26, 112–123. [Google Scholar] [CrossRef]
- Yu, H.W.; Yi, J.W.; Seong, C.Y.; Kim, J.-K.; Bae, I.E.; Kwon, H.; Chai, Y.J.; Kim, S.-J.; Choi, J.Y.; Lee, K.E. Development of a surgical training model for bilateral axillo-breast approach robotic thyroidectomy. Surg. Endosc. 2018, 32, 1360–1367. [Google Scholar] [CrossRef]
- Liang, T.-J.; Wang, N.-Y.; Tsai, C.-Y.; Liu, S.-I.; Chen, I.-S. Outcome comparison between endoscopic transoral and bilateral axillo-breast approach thyroidectomy performed by a single surgeon. World J. Surg. 2021, 45, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Bae, D.S.; Koo, D.H. A propensity score-matched comparison study of surgical outcomes in patients with differentiated thyroid cancer after robotic versus open total thyroidectomy. World J. Surg. 2019, 43, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Koo, D.H.; Im, H.J.; Park, S.K.; Choi, J.Y.; Paeng, J.C.; Chung, J.-K.; Oh, S.K.; Youn, Y.-K. Surgical completeness of bilateral axillo-breast approach robotic thyroidectomy: Comparison with conventional open thyroidectomy after propensity score matching. Surgery 2011, 150, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Shin, I.B.; Koo, D.H.; Ko, M.J.; Kim, S.H.; Bae, D.S. A prospective, randomized controlled study of the safety and efficacy of gasless bilateral axillo-breast approach (BABA) robotic thyroidectomy. Surg. Endosc. 2020, 34, 4846–4856. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-J.; Lee, K.E.; Myong, J.P.; Koo, D.H.; Lee, J.; Youn, Y.-K. Prospective study of sensation in anterior chest areas before and after a bilateral axillo-breast approach for endoscopic/robotic thyroid surgery. World J. Surg. 2013, 37, 1147–1153. [Google Scholar] [CrossRef]
- Berber, E.; Bernet, V.; Fahey, T.J., III; Kebebew, E.; Shaha, A.; Stack, B.C., Jr.; Stang, M.; Steward, D.L.; Terris, D.J.; Committee, A.T.A.S.A. American Thyroid Association statement on remote-access thyroid surgery. Thyroid 2016, 26, 331–337. [Google Scholar] [CrossRef]
- Russell, J.O.; Noureldine, S.I.; Al Khadem, M.G.; Tufano, R.P. Minimally invasive and remote-access thyroid surgery in the era of the 2015 A merican T hyroid A ssociation guidelines. Laryngoscope Investig. Otolaryngol. 2016, 1, 175–179. [Google Scholar] [CrossRef]
- Paek, S.H.; Kang, K.H.; Kang, H.; Park, S.J. Comparison of postoperative surgical stress following robotic thyroidectomy and open thyroidectomy: A prospective pilot study. Surg. Endosc. 2016, 30, 3861–3866. [Google Scholar] [CrossRef]
- Paek, S.H.; Lee, H.A.; Kwon, H.; Kang, K.H.; Park, S.J. Comparison of robot-assisted modified radical neck dissection using a bilateral axillary breast approach with a conventional open procedure after propensity score matching. Surg. Endosc. 2020, 34, 622–627. [Google Scholar] [CrossRef]
- Shin, H.R.; Lee, K.; Yu, H.W.; Kim, S.-j.; Chai, Y.J.; Choi, J.Y.; Lee, K.E. Comparison of Perioperative Outcomes Using the da Vinci S, Si, X, and Xi Robotic Platforms for BABA Robotic Thyroidectomy. Medicina 2021, 57, 1130. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | ||||
|---|---|---|---|---|
| Overall (n = 44) | Conventional (n = 21) | Mini-Flap (n = 23) | p-Value | |
| Age, years | 40.07 ± 12.01 | 41.19 ± 12.04 | 39.04 ± 12.33 | 0.721 |
| Sex | 1.000 | |||
| Male | 5 (11.4%) | 2 (9.5%) | 3 (13.0%) | |
| Female | 39 (88.6%) | 19 (90.5%) | 20 (87.0%) | |
| BMI (kg/m2) | 24.11 ± 4.22 | 24.07 ± 2.88 | 24.15 ± 5.23 | 0.951 |
| Extent of surgery | 1.000 | |||
| Total thyroidectomy | 7 (15.9%) | 3 (14.3%) | 4 (17.4%) | |
| Unilateral thyroidectomy | 37 (84.1%) | 18 (85.7%) | 19 (82.6%) | |
| CND | 0.709 | |||
| Not performed | 7 (15.9%) | 2 (9.5%) | 5 (21.7%) | |
| Unilateral | 36 (81.8%) | 18 (85.7%) | 18 (78.3%) | |
| Bilateral | 1 (2.3%) | 1 (4.8%) | 0 | |
| Nodes retrieved | 5.60 ± 3.97 | 6.81 ± 4.39 | 4.45 ± 3.20 | 0.050 |
| Metastatic LN | 1.14 ± 2.04 | 1.38 ± 2.58 | 0.91 ± 1.38 | 0.455 |
| Tumor diameter (cm) | 1.05 ± 0.75 | 0.88 ± 0.60 | 1.21 ± 0.85 | 0.149 |
| Pathologic diagnosis | 1.000 | |||
| PTC | 34 (77.3%) | 17 (81.0%) | 17 (73.9%) | |
| HCC | 1 (2.3%) | 0 | 1(4.3%) | |
| Benign | 9 (20.5%) | 4 (19.0%) | 5 (21.7%) | |
| ETE | 1.000 | |||
| Yes | 1 (2.3%) | 0 | 1 (4.3%) | |
| No | 43 (97.7%) | 21 (100.0%) | 22 (95.7%) | |
| Thyroiditis | 0.042 | |||
| Yes | 12 (27.3%) | 9 (42.9%) | 3 (13.0%) | |
| No | 32 (72.7%) | 12 (57.1%) | 20 (87.0%) | |
| Pathological T stage * | 1.000 | |||
| 1a | 26 (74.3%) | 13 (76.5%) | 13 (72.2%) | |
| 1b | 8 (22.9%) | 4 (23.5%) | 4 (22.2%) | |
| 3b | 1 (2.9%) | 0 | 1 (5.6%) | |
| Pathological N stage * | 0.845 | |||
| 0 | 15 (42.9%) | 7 (41.2%) | 8 (44.4%) | |
| 1a | 20 (57.1%) | 10 (58.8%) | 10 (55.6%) | |
| AJCC (8th edition) stage * | 1.000 | |||
| I | 33 (94.3%) | 16 (94.1%) | 17 (94.4%) | |
| II | 2 (5.7%) | 1 (5.9%) | 1 (5.6%) | |
| Group | ||||
|---|---|---|---|---|
| Overall (n = 44) | Conventional (n = 21) | Mini-Flap (n = 23) | p-Value | |
| Operating time (min) | 191.92 ± 35.62 | 206.18 ± 31.09 | 178.90 ± 34.43 | 0.009 |
| Flap-making time (min) | 33.75 ± 8.12 | 38.85 ± 2.73 | 32.21 ± 8.62 | 0.003 |
| Estimated blood loss (mL) | 98.14 ± 48.89 | 92.05 ± 41.67 | 103.70 ± 55.00 | 0.436 |
| Total drainage (mL) | 172.61 ± 66.85 | 196.57 ± 81.40 | 150.74 ± 40.80 | 0.027 |
| Hospital stay (days) | 4.66 ± 1.18 | 4.86 ± 1.24 | 4.48 ± 1.12 | 0.293 |
| Group | |||
|---|---|---|---|
| Conventional (n = 21) | Mini-Flap (n = 23) | p-Value | |
| Numeric rating scale score | |||
| Postoperative 2 h | 5.52 ± 0.87 | 4.57 ± 1.31 | 0.006 |
| Postoperative 24 h | 2.81 ± 0.40 | 3.00 ± 1.09 | 0.440 |
| Postoperative 48 h | 2.76 ± 0.44 | 2.87 ± 0.87 | 0.612 |
| Postoperative 72 h | 2.67 ± 0.48 | 2.39 ± 0.78 | 0.172 |
| Number of analgesics | |||
| Postoperative 2 h | 0.95 ± 0.22 | 0.65 ± 0.49 | 0.012 |
| Postoperative 24 h | 0.29 ± 0.56 | 0.48 ± 0.59 | 0.276 |
| Postoperative 48 h | 0.48 ± 0.98 | 0.30 ± 0.77 | 0.518 |
| Postoperative 72 h | 0.00 ± 0.00 | 0.09 ± 0.29 | 0.162 |
| Group | ||||
|---|---|---|---|---|
| Overall (n = 44) | Conventional (n = 21) | Mini-Flap (n = 23) | p-Value | |
| Postoperative lowest iPTH (pg/mL) | 38.81 ± 18.40 | 39.98 ± 17.89 | 37.75 ± 19.20 | 0.693 |
| Postoperative hypoparathyroidism | 1.000 | |||
| No | 41 (93.2%) | 20 (95.2%) | 21 (91.3%) | |
| Transient | 3 (6.8%) | 1 (4.8%) | 2 (8.7%) | |
| Permanent | 0 | 0 | 0 | |
| Postoperative vocal cord palsy | 0.599 | |||
| No | 41 (93.2%) | 19 (90.5%) | 22 (95.7%) | |
| Transient | 3 (6.8%) | 2 (9.5%) | 1 (4.3%) | |
| Permanent | 0 | 0 | 0 | |
| Other complications | 0 | 0 | 0 | |
| Group | ||||
|---|---|---|---|---|
| Overall (n = 35) | Conventional (n = 17) | Mini-Flap (n = 18) | p-Value | |
| Response to therapy | 1.000 | |||
| Excellent | 31 (88.6%) | 16 (94.1%) | 15 (83.3%) | |
| Indeterminate | 3 (8.6%) | 1 (5.9%) | 2 (11.1%) | |
| Biochemically incomplete | 1 (2.9%) | 0 | 1 (5.6%) | |
| Structurally incomplete | 0 | 0 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, I.B.; Bae, D.S. Comparison of the Postoperative Outcomes of the Mini-Flap Bilateral Axillo-Breast Approach (BABA) and Conventional BABA Robot-Assisted Thyroidectomy. J. Clin. Med. 2022, 11, 4894. https://doi.org/10.3390/jcm11164894
Shin IB, Bae DS. Comparison of the Postoperative Outcomes of the Mini-Flap Bilateral Axillo-Breast Approach (BABA) and Conventional BABA Robot-Assisted Thyroidectomy. Journal of Clinical Medicine. 2022; 11(16):4894. https://doi.org/10.3390/jcm11164894
Chicago/Turabian StyleShin, Ik Beom, and Dong Sik Bae. 2022. "Comparison of the Postoperative Outcomes of the Mini-Flap Bilateral Axillo-Breast Approach (BABA) and Conventional BABA Robot-Assisted Thyroidectomy" Journal of Clinical Medicine 11, no. 16: 4894. https://doi.org/10.3390/jcm11164894