
Role of Lipid-Lowering Therapy in Peripheral Artery Disease


Abstract
:1. Introduction
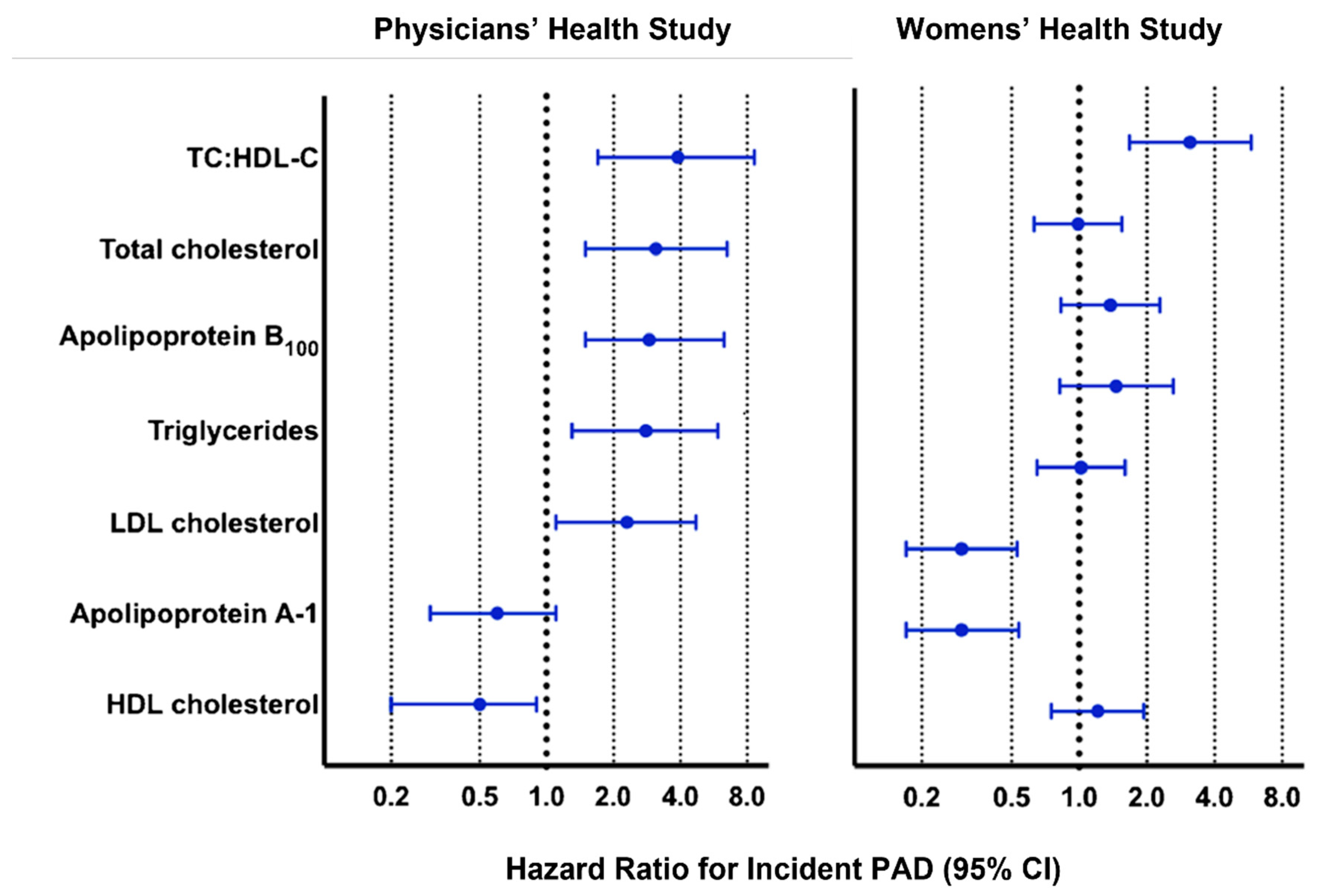
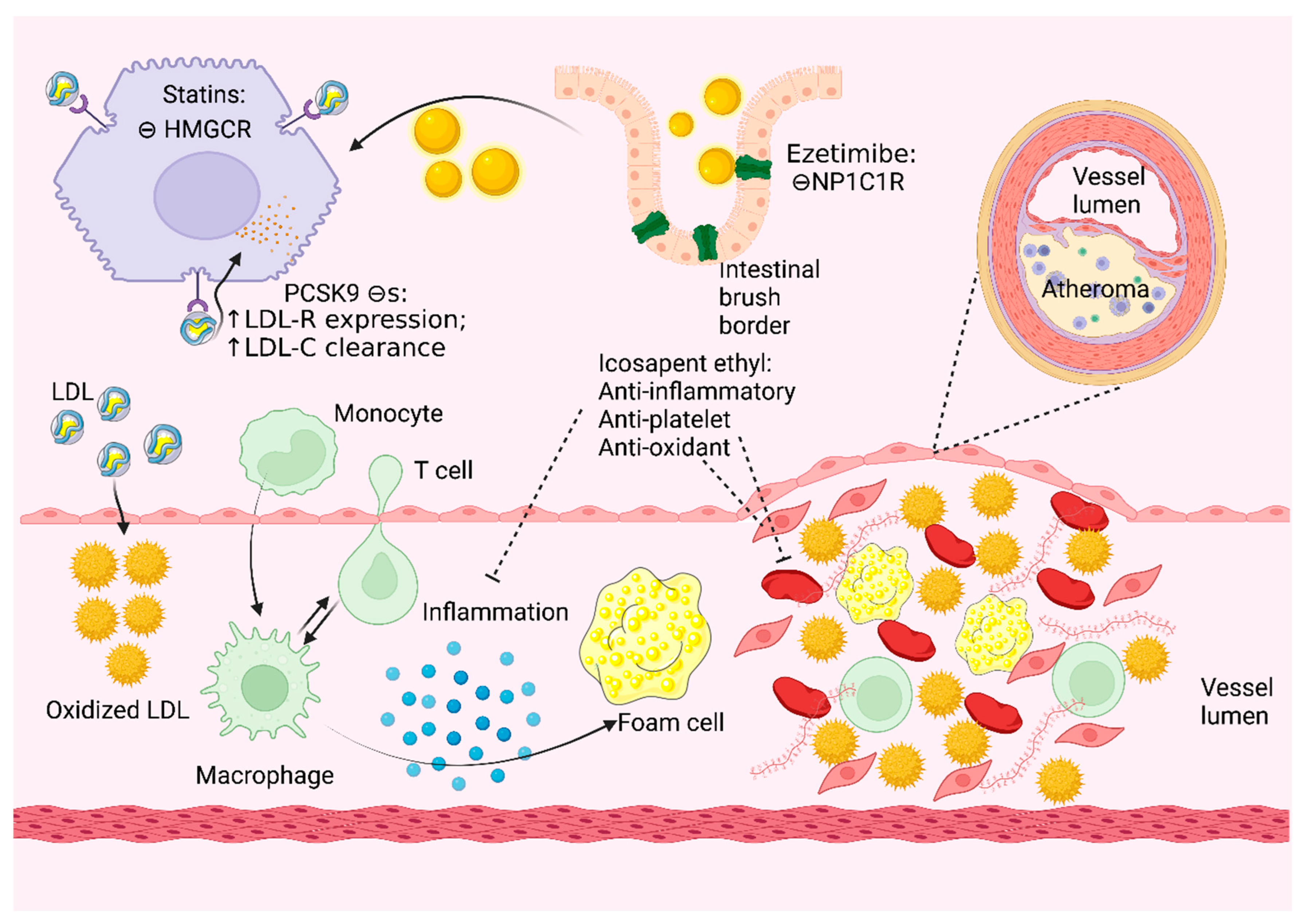
2. Role of Lipids in Atherosclerosis
3. Epidemiology and Clinical Burden of PAD
4. Role of Statins in PAD
4.1. Mechanism of Action of Statins
4.2. Clinical Outcomes Associated with Statin Use in Patients with PAD
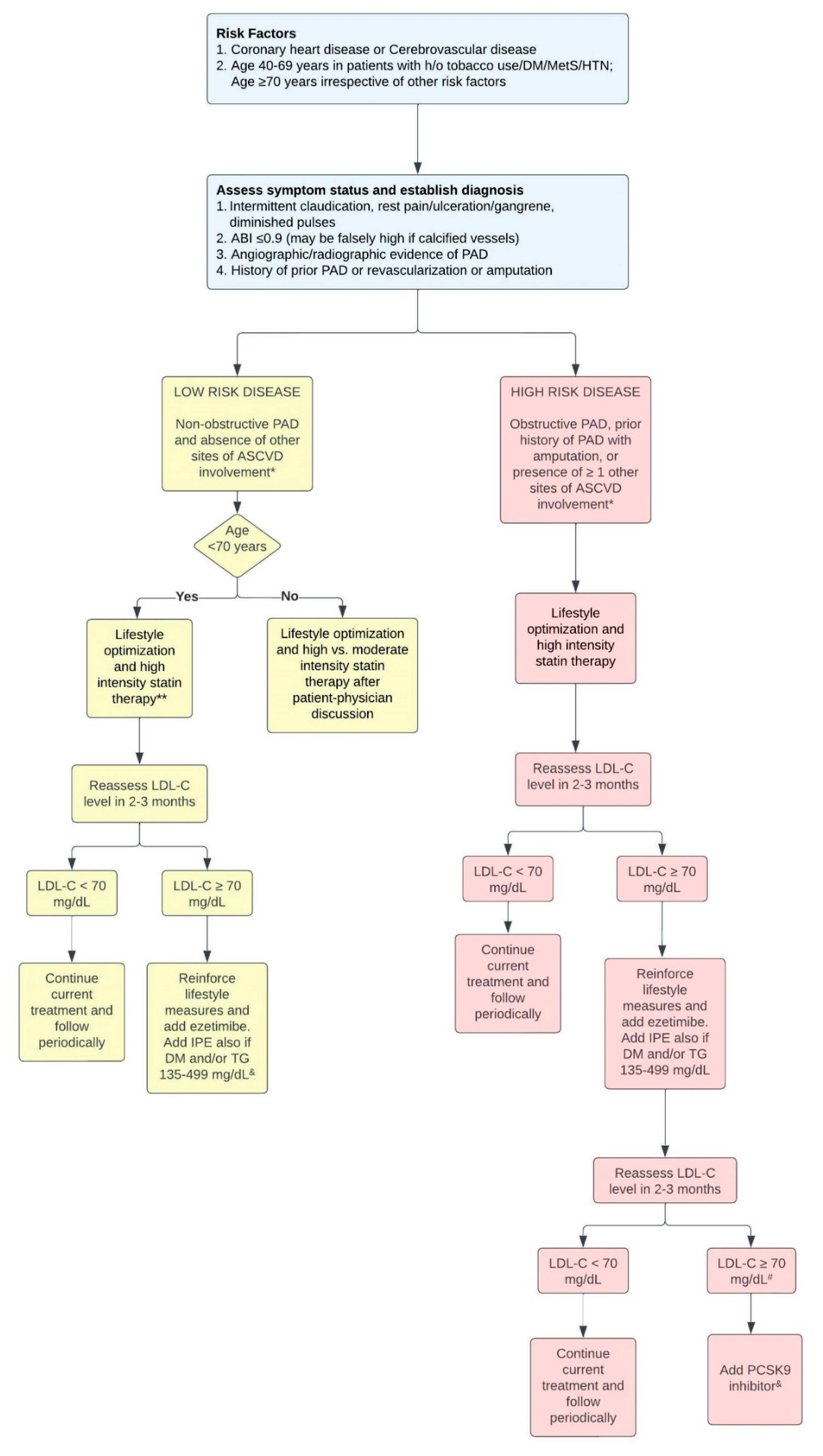
4.3. Current Guidelines
4.4. Underuse of Statins in PAD
5. Role of PCSK9 Inhibitors in Patients with PAD
5.1. Mechanism of Action of PCSK9 Inhibitors
5.2. Clinical Outcomes of PCSK9 Inhibitors in Patients with PAD
6. Role of Icosapent Ethyl (IPE) in PAD
7. Role of Fibrates, Ezetimibe and Niacin in PAD
8. Novel Drugs: Inclisiran
9. Role of Apheresis in PAD
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Palasubramaniam, J.; Wang, X.; Peter, K. Myocardial Infarction-From Atherosclerosis to Thrombosis. Arter. Thromb. Vasc. Biol. 2019, 39, e176–e185. [Google Scholar] [CrossRef] [PubMed]
- Berliner, J.A.; Navab, M.; Fogelman, A.M.; Frank, J.S.; Demer, L.L.; Edwards, P.A.; Watson, A.D.; Lusis, A.J. Atherosclerosis: Basic Mechanisms. Oxidation, Inflammation, and Genetics. Circulation 1995, 91, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.M.; Moxon, J.V.; Golledge, J. A Review of the Pathophysiology and Potential Biomarkers for Peripheral Artery Disease. Int. J. Mol. Sci. 2015, 16, 11294–11322. [Google Scholar] [CrossRef]
- Knowles, J.W.; Assimes, T.L.; Li, J.; Quertermous, T.; Cooke, J.P. Genetic Susceptibility to Peripheral Arterial Disease: A Dark Corner in Vascular Biology. Arter. Thromb. Vasc. Biol. 2007, 27, 2068–2078. [Google Scholar] [CrossRef] [PubMed]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.J.F.; Brodmann, M.; Baumgartner, I.; Binder, C.J.; Casula, M.; Heiss, C.; Kahan, T.; Parini, P.; Poredos, P.; Catapano, A.L.; et al. Lipid-Lowering and Anti-Thrombotic Therapy in Patients with Peripheral Arterial Disease: European Atherosclerosis Society/European Society of Vascular Medicine Joint Statement. Atherosclerosis 2021, 338, 55–63. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Murray, G.D.; Butcher, I.; Folsom, A.R.; Hirsch, A.T.; Couper, D.J.; Debacker, G.; Kornitzer, M.; Newman, A.B.; Sutton-Tyrrell, K.C.; et al. Development and Validation of an Ankle Brachial Index Risk Model for the Prediction of Cardiovascular Events. Eur. J. Prev. Cardiol. 2014, 21, 310–320. [Google Scholar] [CrossRef]
- Criqui, M.H.; Aboyans, V. Epidemiology of Peripheral Artery Disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef]
- Morita, S. Metabolism and Modification of Apolipoprotein B-Containing Lipoproteins Involved in Dyslipidemia and Atherosclerosis. Biol. Pharm. Bull. 2016, 39, 1–24. [Google Scholar] [CrossRef]
- Sanda, G.E.; Belur, A.D.; Teague, H.L.; Mehta, N.N. Emerging Associations Between Neutrophils, Atherosclerosis, and Psoriasis. Curr. Atheroscler. Rep. 2017, 19, 53. [Google Scholar] [CrossRef]
- Aday, A.W.; Lawler, P.R.; Cook, N.R.; Ridker, P.M.; Mora, S.; Pradhan, A.D. Lipoprotein Particle Profiles, Standard Lipids, and Peripheral Artery Disease Incidence. Circulation 2018, 138, 2330–2341. [Google Scholar] [CrossRef]
- Bergiers, S.; Vaes, B.; Degryse, J. To Screen or Not to Screen for Peripheral Arterial Disease in Subjects Aged 80 and over in Primary Health Care: A Cross-Sectional Analysis from the BELFRAIL Study. BMC Fam. Pract. 2011, 12, 39. [Google Scholar] [CrossRef]
- Rosero, E.B.; Kane, K.; Clagett, G.P.; Timaran, C.H. A Systematic Review of the Limitations and Approaches to Improve Detection and Management of Peripheral Arterial Disease in Hispanics. J. Vasc. Surg. 2010, 51, 27S–35S. [Google Scholar] [CrossRef]
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef]
- Forbang, N.I.; Criqui, M.H.; Allison, M.A.; Ix, J.H.; Steffen, B.T.; Cushman, M.; Tsai, M.Y. Sex and Ethnic Differences in the Associations between Lipoprotein(a) and Peripheral Arterial Disease in the Multi-Ethnic Study of Atherosclerosis. J. Vasc. Surg. 2016, 63, 453–458. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of Global Estimates of Prevalence and Risk Factors for Peripheral Artery Disease in 2000 and 2010: A Systematic Review and Analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Duval, S.; Massaro, J.M.; Jaff, M.R.; Boden, W.E.; Alberts, M.J.; Califf, R.M.; Eagle, K.A.; D’Agostino, R.B.; Pedley, A.; Fonarow, G.C.; et al. An Evidence-Based Score to Detect Prevalent Peripheral Artery Disease (PAD). Vasc. Med. 2012, 17, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Ihnat, D.M.; Mills, J.L. Current Assessment of Endovascular Therapy for Infrainguinal Arterial Occlusive Disease in Patients with Diabetes. J. Vasc. Surg. 2010, 52, 92S–95S. [Google Scholar] [CrossRef]
- Lawall, H.; Bramlage, P.; Amann, B. Stem Cell and Progenitor Cell Therapy in Peripheral Artery Disease. A Critical Appraisal. Thromb. Haemost. 2010, 103, 696–709. [Google Scholar] [CrossRef]
- Davies, M.G. Critical Limb Ischemia: Cell and Molecular Therapies for Limb Salvage. Methodist DeBakey Cardiovasc. J. 2012, 8, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, R.S.; Back, M.R.; Armstrong, P.A.; Cuthbertson, D.; Shames, M.L.; Johnson, B.L.; Bandyk, D.F. The Relative Importance of Graft Surveillance and Warfarin Therapy in Infrainguinal Prosthetic Bypass Failure. J. Vasc. Surg. 2007, 46, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Adam, D.J.; Beard, J.D.; Cleveland, T.; Bell, J.; Bradbury, A.W.; Forbes, J.F.; Fowkes, F.G.R.; Gillepsie, I.; Ruckley, C.V.; Raab, G.; et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL): Multicentre, Randomised Controlled Trial. Lancet 2005, 366, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Corrado, E.; Mignano, A.; Coppola, G. Use of Statins in Patients with Peripheral Artery Disease. Trends Cardiovasc. Med. 2020, 30, 257–262. [Google Scholar] [CrossRef]
- Coppola, G.; Novo, S. Statins and Peripheral Arterial Disease: Effects on Claudication, Disease Progression, and Prevention of Cardiovascular Events. Arch. Med. Res. 2007, 38, 479–488. [Google Scholar] [CrossRef]
- Antoniou, G.A.; Fisher, R.K.; Georgiadis, G.S.; Antoniou, S.A.; Torella, F. Statin Therapy in Lower Limb Peripheral Arterial Disease: Systematic Review and Meta-Analysis. Vascul. Pharmacol. 2014, 63, 79–87. [Google Scholar] [CrossRef]
- Pedersen, T.R.; Kjekshus, J.; Pyörälä, K.; Olsson, A.G.; Cook, T.J.; Musliner, T.A.; Tobert, J.A.; Haghfelt, T. Effect of Simvastatin on Ischemic Signs and Symptoms in the Scandinavian Simvastatin Survival Study (4S). Am. J. Cardiol. 1998, 81, 333–335. [Google Scholar] [CrossRef]
- Heart Protection Study Collaborative Group. Randomized Trial of the Effects of Cholesterol-Lowering with Simvastatin on Peripheral Vascular and Other Major Vascular Outcomes in 20,536 People with Peripheral Arterial Disease and Other High-Risk Conditions. J. Vasc. Surg. 2007, 45, 645–654. [Google Scholar] [CrossRef]
- Kumbhani, D.J.; Steg, P.G.; Cannon, C.P.; Eagle, K.A.; Smith, S.C.; Goto, S.; Ohman, E.M.; Elbez, Y.; Sritara, P.; Baumgartner, I.; et al. Statin Therapy and Long-Term Adverse Limb Outcomes in Patients with Peripheral Artery Disease: Insights from the REACH Registry. Eur. Heart J. 2014, 35, 2864–2872. [Google Scholar] [CrossRef]
- Stavroulakis, K.; Borowski, M.; Torsello, G.; Bisdas, T.; CRITISCH collaborators. Association between Statin Therapy and Amputation-Free Survival in Patients with Critical Limb Ischemia in the CRITISCH Registry. J. Vasc. Surg. 2017, 66, 1534–1542. [Google Scholar] [CrossRef]
- Long, C.A.; Mulder, H.; Fowkes, F.G.R.; Baumgartner, I.; Berger, J.S.; Katona, B.G.; Mahaffey, K.W.; Norgren, L.; Blomster, J.I.; Rockhold, F.W.; et al. Incidence and Factors Associated with Major Amputation in Patients with Peripheral Artery Disease: Insights from the EUCLID Trial. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006399. [Google Scholar] [CrossRef]
- Arya, S.; Khakharia, A.; Binney, Z.O.; DeMartino, R.R.; Brewster, L.P.; Goodney, P.P.; Wilson, P.W.F. Association of Statin Dose with Amputation and Survival in Patients with Peripheral Artery Disease. Circulation 2018, 137, 1435–1446. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Chen, Y.-T.; Su, Y.-W.; Chang, C.-C.; Huang, P.-H.; Lin, S.-J. Statin Therapy Reduces Future Risk of Lower-Limb Amputation in Patients with Diabetes and Peripheral Artery Disease. J. Clin. Endocrinol. Metab. 2017, 102, 2373–2381. [Google Scholar] [CrossRef]
- Aung, P.P.; Maxwell, H.G.; Jepson, R.G.; Price, J.F.; Leng, G.C. Lipid-Lowering for Peripheral Arterial Disease of the Lower Limb. Cochrane Database Syst. Rev. 2007, 4, CD000123. [Google Scholar] [CrossRef]
- Walldius, G.; Erikson, U.; Olsson, A.G.; Bergstrand, L.; Hådell, K.; Johansson, J.; Kaijser, L.; Lassvik, C.; Mölgaard, J.; Nilsson, S. The Effect of Probucol on Femoral Atherosclerosis: The Probucol Quantitative Regression Swedish Trial (PQRST). Am. J. Cardiol. 1994, 74, 875–883. [Google Scholar] [CrossRef]
- Pastori, D.; Farcomeni, A.; Milanese, A.; del Sole, F.; Menichelli, D.; Hiatt, W.R.; Violi, F. Statins and Major Adverse Limb Events in Patients with Peripheral Artery Disease: A Systematic Review and Meta-Analysis. Thromb. Haemost. 2020, 120, 866–875. [Google Scholar] [CrossRef]
- Kokkinidis, D.G.; Arfaras-Melainis, A.; Giannopoulos, S.; Katsaros, I.; Jawaid, O.; Jonnalagadda, A.K.; Parikh, S.A.; Secemsky, E.A.; Giri, J.; Kumbhani, D.J.; et al. Statin Therapy for Reduction of Cardiovascular and Limb-Related Events in Critical Limb Ischemia: A Systematic Review and Meta-Analysis. Vasc. Med. 2020, 25, 106–117. [Google Scholar] [CrossRef]
- Mondillo, S.; Ballo, P.; Barbati, R.; Guerrini, F.; Ammaturo, T.; Agricola, E.; Pastore, M.; Borrello, F.; Belcastro, M.; Picchi, A.; et al. Effects of Simvastatin on Walking Performance and Symptoms of Intermittent Claudication in Hypercholesterolemic Patients with Peripheral Vascular Disease. Am. J. Med. 2003, 114, 359–364. [Google Scholar] [CrossRef]
- Jones, W.S.; Schmit, K.M.; Vemulapalli, S.; Subherwal, S.; Patel, M.R.; Hasselblad, V.; Heidenfelder, B.L.; Chobot, M.M.; Posey, R.; Wing, L.; et al. Treatment Strategies for Patients with Peripheral Artery Disease [Internet]; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013; Report No.: 13-EHC090-EF. [Google Scholar]
- Crismaru, I.; Diaconu, C.C. Lipid-lowering therapy in patients with peripheral artery disease. E-J. ESC Counc. Cardiol. Pract. 2015, 13, 31. [Google Scholar]
- Momsen, A.H.; Jensen, M.B.; Norager, C.B.; Madsen, M.R.; Vestersgaard-Andersen, T.; Lindholt, J.S. Drug therapy for improving walking distance in intermittent claudication: A systematic review and meta-analysis of robust randomised controlled studies. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 463–474. [Google Scholar] [CrossRef]
- Aronow, W.S. Lipid-lowering therapy in high-risk persons. Compr. Ther. 2006, 32, 68–73. [Google Scholar] [CrossRef]
- Harris, S.K.; Roos, M.G.; Landry, G.J. Statin use in patients with peripheral arterial disease. J. Vasc. Surg. 2016, 64, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Spring, B.; Tian, L.; Treat-Jacobson, D.; Ferrucci, L.; Lloyd-Jones, D.; Zhao, L.; Polonsky, T.; Kibbe, M.R.; Bazzano, L.; et al. Effect of Low-Intensity vs. High-Intensity Home-Based Walking Exercise on Walk Distance in Patients with Peripheral Artery Disease: The LITE Randomized Clinical Trial. JAMA 2021, 325, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Jansen-Chaparro, S.; López-Carmona, M.D.; Cobos-Palacios, L.; Sanz-Cánovas, J.; Bernal-López, M.R.; Gómez-Huelgas, R. Statins and Peripheral Arterial Disease: A Narrative Review. Front. Cardiovasc. Med. 2021, 8, 777016. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, G.; Spadarella, G.; Cafaro, G.; Petitto, M.; Lupoli, R.; Di Minno, A.; De Gaetano, G.; Tremoli, E. Systematic reviews and meta-analyses for more profitable strategies in peripheral artery disease. Ann. Med. 2014, 46, 475–489. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.J.F.; Brodmann, M.; Baumgartner, I.; Binder, C.J.; Casula, M.; Heiss, C.; Kahan, T.; Parini, P.; Poredos, P.; Catapano, A.L.; et al. Lipid-lowering and anti-thrombotic therapy in patients with peripheral arterial disease. Vasa 2021, 50, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Harwood, A.E.; Pymer, S.; Ingle, L.; Doherty, P.; Chetter, I.C.; Parmenter, B.; Askew, C.D.; Tew, G.A. Exercise training for intermittent claudication: A narrative review and summary of guidelines for practitioners. BMJ Open Sport Exerc. Med. 2020, 6, e000897. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The Effects of Lowering LDL Cholesterol with Statin Therapy in People at Low Risk of Vascular Disease: Meta-Analysis of Individual Data from 27 Randomised Trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/AphA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Singh, N.; Ding, L.; Devera, J.; Magee, G.A.; Garg, P.K. Prescribing of Statins After Lower Extremity Revascularization Procedures in the US. JAMA Netw. Open 2021, 4, e2136014. [Google Scholar] [CrossRef]
- Conte, M.S.; Bandyk, D.F.; Clowes, A.W.; Moneta, G.L.; Namini, H.; Seely, L. Risk Factors, Medical Therapies and Perioperative Events in Limb Salvage Surgery: Observations from the PREVENT III Multicenter Trial. J. Vasc. Surg. 2005, 42, 456–464. [Google Scholar] [CrossRef]
- Hess, C.N.; Cannon, C.P.; Beckman, J.A.; Goodney, P.P.; Patel, M.R.; Hiatt, W.R.; Mues, K.E.; Orroth, K.K.; Shannon, E.; Bonaca, M.P. Effectiveness of Blood Lipid Management in Patients with Peripheral Artery Disease. J. Am. Coll. Cardiol. 2021, 77, 3016–3027. [Google Scholar] [CrossRef]
- Colantonio, L.D.; Hubbard, D.; Monda, K.L.; Mues, K.E.; Huang, L.; Dai, Y.; Jackson, E.A.; Brown, T.M.; Rosenson, R.S.; Woodward, M.; et al. Atherosclerotic Risk and Statin Use Among Patients with Peripheral Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 251–264. [Google Scholar] [CrossRef]
- Kiyosue, A.; Honarpour, N.; Kurtz, C.; Xue, A.; Wasserman, S.M.; Hirayama, A. A Phase 3 Study of Evolocumab (AMG 145) in Statin-Treated Japanese Patients at High Cardiovascular Risk. Am. J. Cardiol. 2016, 117, 40–47. [Google Scholar] [CrossRef]
- Mayne, J.; Dewpura, T.; Raymond, A.; Cousins, M.; Chaplin, A.; Lahey, K.A.; Lahaye, S.A.; Mbikay, M.; Ooi, T.C.; Chrétien, M. Plasma PCSK9 Levels Are Significantly Modified by Statins and Fibrates in Humans. Lipids Health Dis. 2008, 7, 22. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.; Honarpour, N.; Wang, H.; Liu, T.; Wasserman, S.M.; Scott, R.; Sever, P.S.; Pedersen, T.R. Rationale and Design of the Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk Trial. Am. Heart J. 2016, 173, 94–101. [Google Scholar] [CrossRef]
- Oyama, K.; Giugliano, R.P.; Tang, M.; Bonaca, M.P.; Saver, J.L.; Murphy, S.A.; Ruzza, A.; Keech, A.C.; Sever, P.S.; Sabatine, M.S.; et al. Effect of Evolocumab on Acute Arterial Events across All Vascular Territories: Results from the FOURIER Trial. Eur. Heart J. 2021, 42, 4821–4829. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Nault, P.; Giugliano, R.P.; Keech, A.C.; Pineda, A.L.; Kanevsky, E.; Kuder, J.; Murphy, S.A.; Jukema, J.W.; Lewis, B.S.; et al. Low-Density Lipoprotein Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk). Circulation 2018, 137, 338–350. [Google Scholar] [CrossRef]
- Skeik, N.; Nowariak, M.E.; Smith, J.E.; Alexander, J.Q.; Manunga, J.M.; Mirza, A.K.; Sullivan, T.M. Lipid-Lowering Therapies in Peripheral Artery Disease: A Review. Vasc. Med. 2021, 26, 71–80. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bittner, V.A.; Diaz, R.; Goodman, S.G.; Kim, Y.-U.; Jukema, J.W.; Pordy, R.; Roe, M.T.; et al. Peripheral Artery Disease and Venous Thromboembolic Events After Acute Coronary Syndrome: Role of Lipoprotein(a) and Modification by Alirocumab: Prespecified Analysis of the ODYSSEY OUTCOMES Randomized Clinical Trial. Circulation 2020, 141, 1608–1617. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Budoff, M.J.; Bhatt, D.L.; Kinninger, A.; Lakshmanan, S.; Muhlestein, J.B.; Le, V.T.; May, H.T.; Shaikh, K.; Shekar, C.; Roy, S.K.; et al. Effect of Icosapent Ethyl on Progression of Coronary Atherosclerosis in Patients with Elevated Triglycerides on Statin Therapy: Final Results of the EVAPORATE Trial. Eur. Heart J. 2020, 41, 3925–3932. [Google Scholar] [CrossRef]
- Virani, S.S.; Morris, P.B.; Agarwala, A.; Ballantyne, C.M.; Birtcher, K.K.; Kris-Etherton, P.M.; Ladden-Stirling, A.B.; Miller, M.; Orringer, C.E.; Stone, N.J. 2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients with Persistent Hypertriglyceridemia: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 78, 960–993. [Google Scholar] [CrossRef]
- Sohn, M.-W.; Meadows, J.L.; Oh, E.H.; Budiman-Mak, E.; Lee, T.A.; Stone, N.J.; Pearce, W.B. Statin Use and Lower Extremity Amputation Risk in Nonelderly Diabetic Patients. J. Vasc. Surg. 2013, 58, 1578–1585.e1. [Google Scholar] [CrossRef]
- West, A.M.; Anderson, J.D.; Meyer, C.H.; Epstein, F.H.; Wang, H.; Hagspiel, K.D.; Berr, S.S.; Harthun, N.L.; DiMaria, J.M.; Hunter, J.R.; et al. The Effect of Ezetimibe on Peripheral Arterial Atherosclerosis Depends upon Statin Use at Baseline. Atherosclerosis 2011, 218, 156–162. [Google Scholar] [CrossRef]
- Ray, K.K.; Wright, R.S.; Kallend, D.; Koenig, W.; Leiter, L.A.; Raal, F.J.; Bisch, J.A.; Richardson, T.; Jaros, M.; Wijngaard, P.L.J.; et al. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N. Engl. J. Med. 2020, 382, 1507–1519. [Google Scholar] [CrossRef]
- Ray, K.K.; Landmesser, U.; Leiter, L.A.; Kallend, D.; Dufour, R.; Karakas, M.; Hall, T.; Troquay, R.P.T.; Turner, T.; Visseren, F.L.J.; et al. Inclisiran in Patients at High Cardiovascular Risk with Elevated LDL Cholesterol. N. Engl. J. Med. 2017, 376, 1430–1440. [Google Scholar] [CrossRef]
- Dieplinger, B.; Lingenhel, A.; Baumgartner, N.; Poelz, W.; Dieplinger, H.; Haltmayer, M.; Kronenberg, F.; Mueller, T. Increased Serum Lipoprotein(a) Concentrations and Low Molecular Weight Phenotypes of Apolipoprotein(a) Are Associated with Symptomatic Peripheral Arterial Disease. Clin. Chem. 2007, 53, 1298–1305. [Google Scholar] [CrossRef]
- Gurdasani, D.; Sjouke, B.; Tsimikas, S.; Hovingh, G.K.; Luben, R.N.; Wainwright, N.W.J.; Pomilla, C.; Wareham, N.J.; Khaw, K.-T.; Boekholdt, S.M.; et al. Lipoprotein(a) and Risk of Coronary, Cerebrovascular, and Peripheral Artery Disease: The EPIC-Norfolk Prospective Population Study. Arter. Thromb. Vasc. Biol. 2012, 32, 3058–3065. [Google Scholar] [CrossRef]
- Thompson, G.R.; Catapano, A.; Saheb, S.; Atassi-Dumont, M.; Barbir, M.; Eriksson, M.; Paulweber, B.; Sijbrands, E.; Stalenhoef, A.F.; Parhofer, K.G. Severe Hypercholesterolaemia: Therapeutic Goals and Eligibility Criteria for LDL Apheresis in Europe. Curr. Opin. Lipidol. 2010, 21, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Winters, J.L. Lipid Apheresis, Indications, and Principles. J. Clin. Apher. 2011, 26, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Schatz, U.; Tselmin, S.; Müller, G.; Julius, U.; Hohenstein, B.; Fischer, S.; Bornstein, S.R. Most Significant Reduction of Cardiovascular Events in Patients Undergoing Lipoproteinapheresis Due to Raised Lp(a) Levels—A Multicenter Observational Study. Atheroscler Suppl. 2017, 30, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Roeseler, E.; Julius, U.; Heigl, F.; Spitthoever, R.; Heutling, D.; Breitenberger, P.; Leebmann, J.; Lehmacher, W.; Kamstrup, P.R.; Nordestgaard, B.G.; et al. Lipoprotein Apheresis for Lipoprotein(a)-Associated Cardiovascular Disease: Prospective 5 Years of Follow-Up and Apolipoprotein(a) Characterization. Arter. Thromb. Vasc. Biol. 2016, 36, 2019–2027. [Google Scholar] [CrossRef] [PubMed]
- Leebmann, J.; Roeseler, E.; Julius, U.; Heigl, F.; Spitthoever, R.; Heutling, D.; Breitenberger, P.; Maerz, W.; Lehmacher, W.; Heibges, A.; et al. Lipoprotein Apheresis in Patients with Maximally Tolerated Lipid-Lowering Therapy, Lipoprotein(a)-Hyperlipoproteinemia, and Progressive Cardiovascular Disease: Prospective Observational Multicenter Study. Circulation 2013, 128, 2567–2576. [Google Scholar] [CrossRef]
- Jaeger, B.R.; Richter, Y.; Nagel, D.; Heigl, F.; Vogt, A.; Roeseler, E.; Parhofer, K.; Ramlow, W.; Koch, M.; Utermann, G.; et al. Longitudinal Cohort Study on the Effectiveness of Lipid Apheresis Treatment to Reduce High Lipoprotein(a) Levels and Prevent Major Adverse Coronary Events. Nat. Clin. Pract. Cardiol. 2009, 6, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.; Julius, U. Lipoprotein(a) Apheresis in Patients with Peripheral Arterial Disease: Rationale and Clinical Results. Clin. Res. Cardiol. Suppl. 2019, 14, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Novartis Pharmaceuticals Assessing the Impact of Lipoprotein (a) Lowering with Pelacarsen (TQJ230) on Major Cardiovascular Events in Patients with CVD (Lp(a)HORIZON): NCT04023552. Available online: https://clinicaltrials.gov/ct2/show/NCT04023552 (accessed on 13 May 2022).
- Fruchart, J.-C.; Nierman, M.C.; Stroes, E.S.G.; Kastelein, J.J.P.; Duriez, P. New Risk Factors for Atherosclerosis and Patient Risk Assessment. Circulation 2004, 109, III-15–III-19. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and Atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Shishehbor, M.H.; Bhatt, D.L. Inflammation and Atherosclerosis. Curr. Atheroscler. Rep. 2004, 6, 131–139. [Google Scholar] [CrossRef]
- Libby, P. The Changing Landscape of Atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Study Design | Sample Size | Patient Population | Intervention | Median Follow Up Time | Outcome | Interpretation |
|---|---|---|---|---|---|---|---|
| Pedersen (4S Study), 1994 [27] | Randomized controlled trial (RCT) | 4444 | MI or angina pectoris, serum cholesterol between 213–309 mg/dL | Simvastatin 20–40 mg daily vs. placebo | 5.4 years | Intermittent claudication | Statin therapy may help in plaque stabilization and may also have a general anti-atherosclerotic effect. |
| Heart Protection Study Collaborative Group, 2002 [28] | RCT | 6748 | History of PAD, CAD, stroke, diabetes, treated hypertension | Simvastatin 40 vs. placebo | 5 years | First major vascular event | Statin treatment showed improvement in MACE, overall revascularizations in all patients with PAD irrespective of their pre-treatment lipid levels. |
| Kumbhani (REACH registry), 2014 [29] | Retrospective review | 5861 | Symptomatic PAD | Statin vs. no statin | 4 years | Primary adverse limb events, primary endpoints of CV death, non-fatal MI, or non-fatal stroke | Patients taking statins had significantly lower risk of MACE and MALE at 4 years. |
| Stavroulakis (CRITISCH registry), 2017 [30] | Retrospective analysis of prospectively collected data | 816 | Presence of new onset CLTI | Statin vs. no statin | 2 years | MACE and cerebral events, amputation free survival | Statin treatment showed improvement in amputation-free survival and overall cardio/cerebrovascular events in patients with new onset CLTI |
| Arya, 2018 [32] | Retrospective observational cohort study | 155,647 | Incident PAD | High-intensity statin therapy vs. low-to-moderate–intensity statin vs. other or no therapies for PAD | 5.9 years | High-intensity statin vs. antiplatelet therapy: Amputation rates, low-to-moderate–intensity statins vs. antiplatelet therapy only: Amputation rates | Statin therapy showed reduced risk of amputation and overall morality as compared to antiplatelet therapy and high-,intensity statin therapy noted more pronounced improvement in comparison to low–moderate-intensity statins. |
| Hsu, 2017 [33] | Retrospective observational cohort study | 69,332 | ≥20 years old with diabetes and PAD | Statin vs. non-statin lipid treatments vs. non-user group | 5.7 years | Statin vs. non statin user, incident LE amputation risk, in-hospital CV death, and all-cause mortality | Statin therapy noted decreased risk of incident and total amputations in patients with diabetes and PAD. It also showed improvement in CV and mortality outcomes. |
| Aung, 2007 [34] | Cochrane meta-analysis | 10,049 | PAD | Lipid lowering treatment vs. none | NA | Total CV events, total coronary events | Lipid lowering therapy improves CV outcomes in patients with PAD. |
| Pastori, 2020 [36] | Meta-analysis | 138,060 | PAD | Statins vs. no statins | NA | MALE, amputations, all-cause mortality, CV deaths, and ischemic stroke | Statin therapy in PAD patients reduces adverse limb outcomes and cardio and cerebrovascular events, as well as overall mortality. |
| Kokkinidis, 2020 [37] | Meta-analysis | 26,985 | Existing CLTI | Statins vs. no statins | NA | Major adverse CV and cerebral events, amputations | Statin use can decrease overall CV and cerebral outcomes in addition to overall mortality. It also might decrease amputation rates, but the data was noted to have significant heterogeneity. |
| Mondillo, 2003 [38] | RCT | 86 | PAD (Fontaine stage II), intermittent claudication and cholesterol levels >220 mg/dL | Simvastatin 40 mg daily vs. placebo | 0, 3 and 6 months | Pain-free walking distance at 6 months, total walking distance | Simvastatin therapy in patients with pre-existing PAD, IC and hypercholesterolemia showed improvement in 6-month pain-free walking distance and total walking distance. |
| Mihaylova (Cholesterol Treatment Trialists group), 2012 [49] | Meta-analysis | 134,537 | NA | Statin vs. no statin | NA | Major vascular event in patients at low 5-year risk of major vascular event | Even in patients with low 5-year major vascular event risk, low-dose statins showed absolute reduction in major vascular events. |
| Oyama (FOURIER), 2018 [58] Bonaca (FOURIER Insights), 2021 [59] | RCT | 27,564 | Prior MI, non-hemorrhagic stroke, or symptomatic PAD, with LDL ≥70 mg/dL or non-HDL-C ≥100 mg/dL while on high- or moderate-intensity statin +/− ezetimibe | Evolucumab vs. placebo | 2.2 years | First acute arterial event, total event rate, ACS, peripheral vascular events, cerebrovascular events | Addition of evolocumab over statin therapy with or without ezetimibe improves vascular outcomes in all territories. |
| Schwartz (ODYSSEY OUTCOMES), 2018, 2020 [61,62] | RCT | 18,924 | History of ACS in last 12 months, LDL-C ≥70 mg/dL, HDL-C at least 100 mg/dL, apoB at least 80 mg/dL on high-intensity or maximally tolerated dose of statin | Alirocumab vs. placebo | 2.8 years | Composite death from CAD, non-fatal MI, fatal or non-fatal ischemic stroke, or unstable angina requiring hospitalization | Alirocumab also shows improvement in overall CV outcomes when prescribed in addition to maximally tolerated or high-dose statin therapy. It also showed improvement in PAD and venous thromboembolism outcomes in these patients. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belur, A.D.; Shah, A.J.; Virani, S.S.; Vorla, M.; Kalra, D.K. Role of Lipid-Lowering Therapy in Peripheral Artery Disease. J. Clin. Med. 2022, 11, 4872. https://doi.org/10.3390/jcm11164872
Belur AD, Shah AJ, Virani SS, Vorla M, Kalra DK. Role of Lipid-Lowering Therapy in Peripheral Artery Disease. Journal of Clinical Medicine. 2022; 11(16):4872. https://doi.org/10.3390/jcm11164872
Chicago/Turabian StyleBelur, Agastya D., Aangi J. Shah, Salim S. Virani, Mounica Vorla, and Dinesh K. Kalra. 2022. "Role of Lipid-Lowering Therapy in Peripheral Artery Disease" Journal of Clinical Medicine 11, no. 16: 4872. https://doi.org/10.3390/jcm11164872