
Outcomes of Deep Sclerectomy following Failed XEN Gel Stent Implantation in Open-Angle Glaucoma: A Prospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Primary Procedure: XEN Gel Stent
2.4. Secondary Procedure: Deep Sclerectomy
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Safety
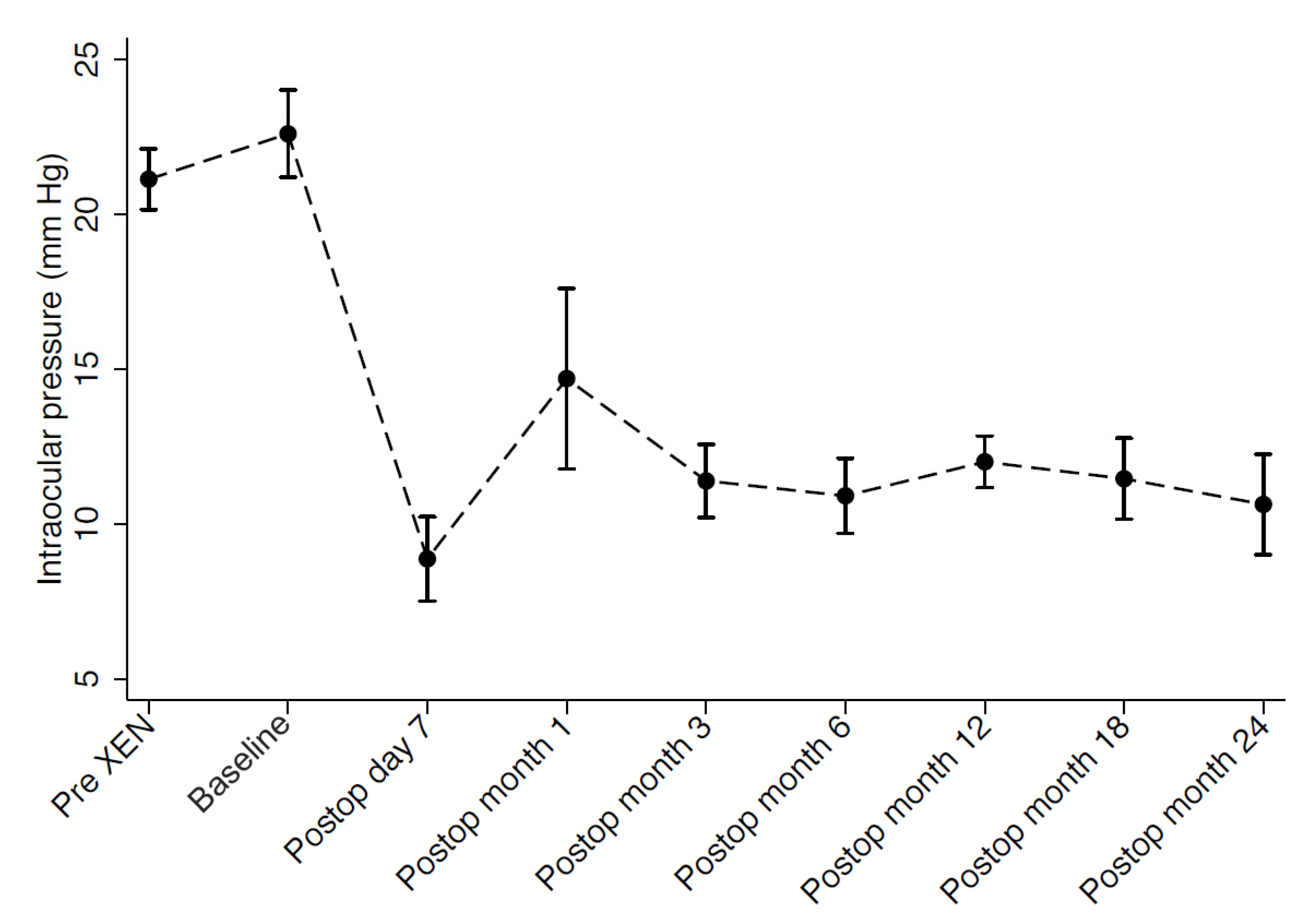
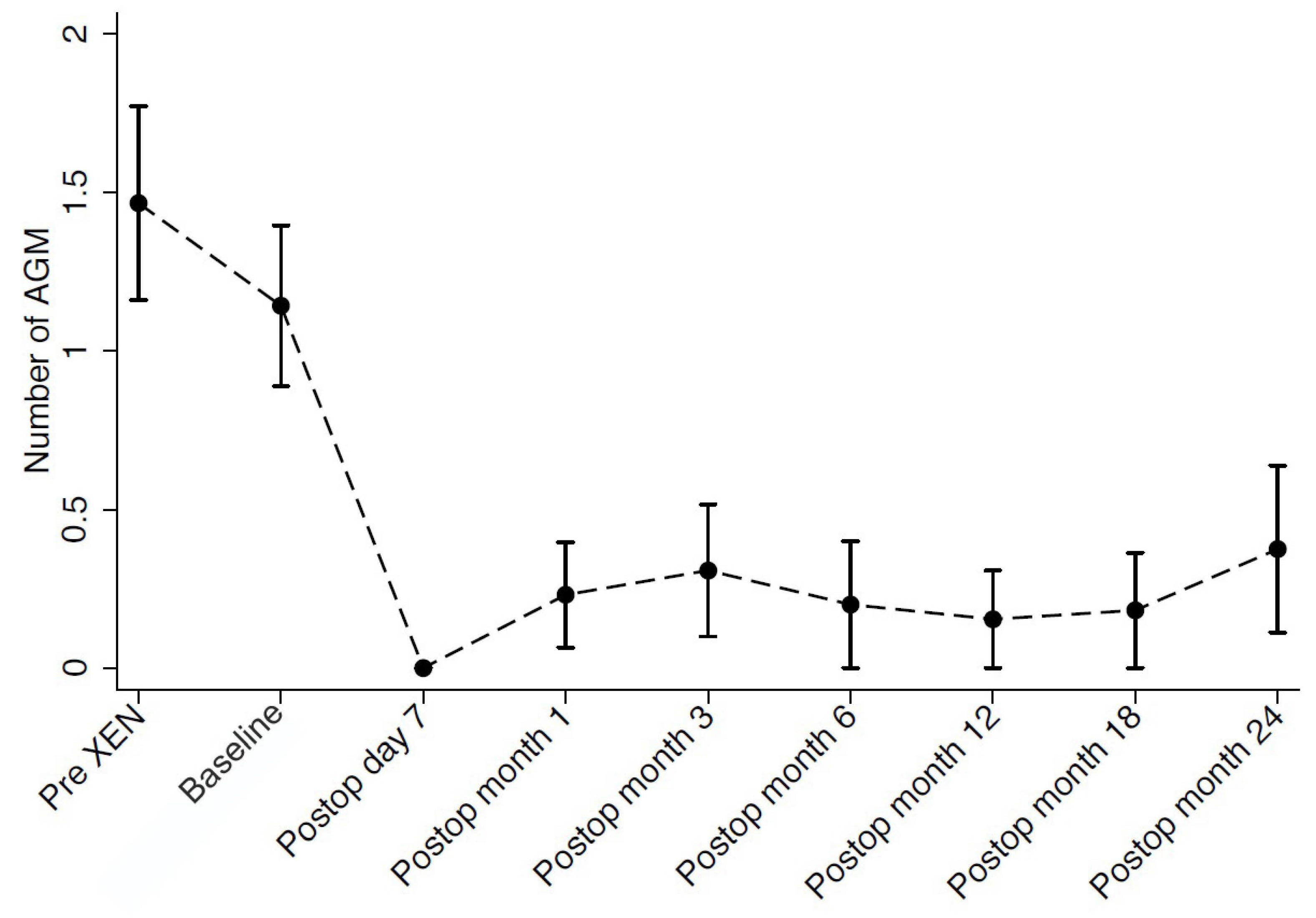
3.3. Intraocular Pressure, Medication Use and Visual Acuity
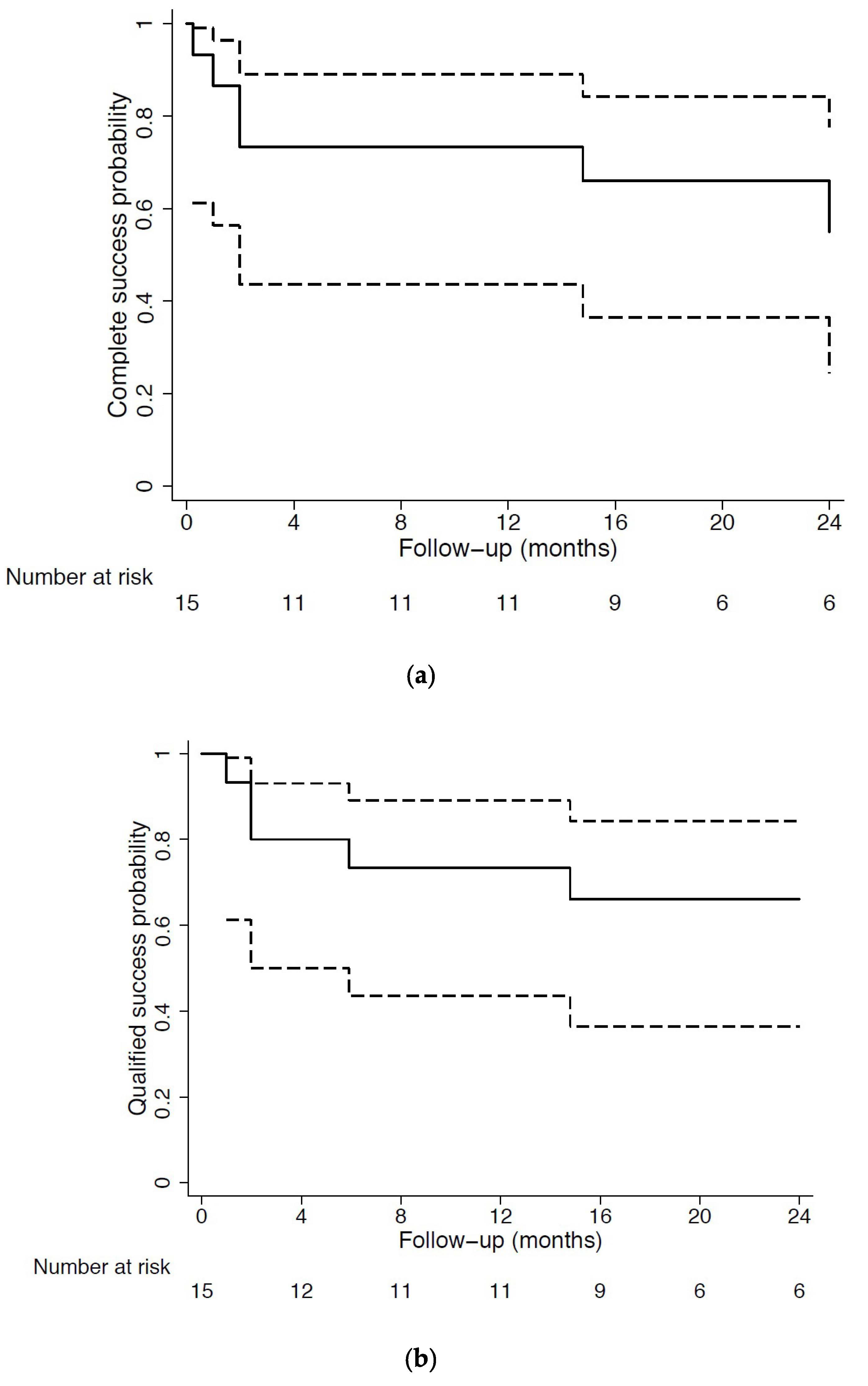
3.4. Primary Outcome: Surgical Success
3.5. Postoperative Interventions
3.6. Postoperative Complications
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DS | deep sclerectomy |
| MMC | mitomycin-C |
| IOP | intraocular pressure |
| MIGS | minimally invasive glaucoma surgery |
| POAG | primary open angle glaucoma |
| PEXG | pseudoexfoliative glaucoma |
| SD-OCT | spectral-domain optical coherence tomography |
| AC | anterior chamber |
| TDM | trabeculo-Descemet’s membrane |
| LGPT | laser goniopuncture |
| SD | standard deviation |
| IRQ | interquartile range |
| MD | mean deviation |
| sLV | square of loss of variance |
| RNFL | retinal nerve fiber layer |
| BCVA | best corrected visual acuity |
| AGM | antiglaucoma medications |
| dB | decibel |
| AE | adverse event |
| GDD | glaucoma drainage device |
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Lavia, C.; Dallorto, L.; Maule, M.; Ceccarelli, M.; Fea, A.M. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0183142. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, A.; Salinas, L.; Guidotti, J.; Mermoud, A.; Mansouri, K. XEN Gel Implant: A new surgical approach in glaucoma. Expert Rev. Med. Devices 2018, 15, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Schlenker, M.B.; Gulamhusein, H.; Conrad-Hengerer, I.; Somers, A.; Lenzhofer, M.; Stalmans, I.; Reitsamer, H.; Hengerer, F.H.; Ahmed, I.I.K. Efficacy, Safety, and Risk Factors for Failure of Standalone Ab Interno Gelatin Microstent Implantation versus Standalone Trabeculectomy. Ophthalmology 2017, 124, 1579–1588. [Google Scholar] [CrossRef] [PubMed]
- Grover, D.S.; Flynn, W.J.; Bashford, K.P.; Lewis, R.A.; Duh, Y.J.; Nangia, R.S.; Niksch, B. Performance and Safety of a New Ab Interno Gelatin Stent in Refractory Glaucoma at 12 Months. Am. J. Ophthalmol. 2017, 183, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, K.; Guidotti, J.; Rao, H.L.; Ouabas, A.; D’Alessandro, E.; Roy, S.; Mermoud, A. Prospective Evaluation of Standalone XEN Gel Implant and Combined Phacoemulsification-XEN Gel Implant Surgery: 1-Year Results. J. Glaucoma 2018, 27, 140–147. [Google Scholar] [CrossRef]
- Mansouri, K.; Bravetti, G.E.; Gillmann, K.; Rao, H.L.; Ch’ng, T.W.; Mermoud, A. Two-Year Outcomes of XEN Gel Stent Surgery in Patients with Open-Angle Glaucoma. Ophthalmol. Glacoma 2019, 2, 309–318. [Google Scholar] [CrossRef]
- Gillmann, K.; Bravetti, G.E.; Rao, H.L.; Mermoud, A.; Mansouri, K. Impact of Phacoemulsification Combined with XEN Gel Stent Implantation on Corneal Endothelial Cell Density: 2-Year Results. J. Glaucoma 2020, 29, 155–160. [Google Scholar] [CrossRef]
- Mansouri, K.; Gillmann, K.; Rao, H.L.; Guidotti, J.; Mermoud, A. Prospective Evaluation of XEN Gel Implant in Eyes With Pseudoexfoliative Glaucoma. J. Glaucoma 2018, 27, 869–873. [Google Scholar] [CrossRef]
- Gillmann, K.; Bravetti, G.E.; Mermoud, A.; Rao, H.L.; Mansouri, K. XEN Gel Stent in Pseudoexfoliative Glaucoma: 2-Year Results of a Prospective Evaluation. J. Glaucoma 2019, 28, 676–684. [Google Scholar] [CrossRef]
- Gizzi, C.; Mohamed-Noriega, J.; Elkarmouty, A.; Scott, A. Trabeculectomy Following Failed Ab Interno Gelatin Microstent: Case Series. J. Glaucoma 2018, 27, e168–e173. [Google Scholar] [CrossRef] [PubMed]
- Laroche, D.; Ng, C.; Lynch, G. Baerveldt Attached to XEN: A New Technique to Manage Failed XEN Glaucoma Surgery. J. Glaucoma 2018, 27, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Sheybani, A.; Reitsamer, H.; Ahmed, I.I. Fluid Dynamics of a Novel Micro-Fistula Implant for the Surgical Treatment of Glaucoma. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4789–4795. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A. Ab interno approach to the subconjunctival space using a collagen glaucoma stent. J. Cataract. Refract. Surg. 2014, 40, 1301–1306. [Google Scholar] [CrossRef]
- Gillmann, K.; Mansouri, K.; Bravetti, G.E.; Mermoud, A. Chronic Intraocular Inflammation as a Risk Factor for XEN Gel Stent Occlusion: A Case of Microscopic Examination of a Fibrin-obstructed XEN Stent. J. Glaucoma 2018, 27, 739–741. [Google Scholar] [CrossRef]
- Ambresin, A.; Shaarawy, T.; Mermoud, A. Deep sclerectomy with collagen implant in one eye compared with trabeculectomy in the other eye of the same patient. J. Glaucoma 2002, 11, 214–220. [Google Scholar] [CrossRef]
- Shaarawy, T.; Mansouri, K.; Schnyder, C.; Ravinet, E.; Achache, F.; Mermoud, A. Long-term results of deep sclerectomy with collagen implant. J. Cataract. Refract. Surg. 2004, 30, 1225–1231. [Google Scholar] [CrossRef]
- El Sayyad, F.; Helal, M.; El-Kholify, H.; Khalil, M.; El-Maghraby, A. Nonpenetrating deep sclerectomy versus trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology 2000, 107, 1671–1674. [Google Scholar] [CrossRef]
- Schwenn, O.; Springer, C.; Troost, A.; Yun, S.H.; Pfeiffer, N. Deep sclerectomy using a hyaluronate implant versus trabeculectomy. A comparison of two glaucoma operations using mitomycin C. Ophthalmologe 2004, 101, 696–704. [Google Scholar] [CrossRef]
- Mermoud, A.; Schnyder, C.C.; Sickenberg, M.; Chiou, A.G.; Hediguer, S.E.; Faggioni, R. Comparison of deep sclerectomy with collagen implant and trabeculectomy in open-angle glaucoma. J. Cataract Refract. Surg. 1999, 25, 323–331. [Google Scholar] [CrossRef]
- Delarive, T.; Rossier, A.; Rossier, S.; Ravinet, E.; Shaarawy, T.; Mermoud, A. Aqueous dynamic and histological findings after deep sclerectomy with collagen implant in an animal model. Br. J. Ophthalmol. 2003, 87, 1340–1344. [Google Scholar] [CrossRef] [PubMed]
- Aptel, F.; Dumas, S.; Denis, P. Ultrasound biomicroscopy and optical coherence tomography imaging of filtering blebs after deep sclerectomy with new collagen implant. Eur. J. Ophthalmol. 2009, 19, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.H.; Johnson, M. How does nonpenetrating glaucoma surgery work? Aqueous outflow resistance and glaucoma surgery. J. Glaucoma 2001, 10, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Kazakova, D.; Roters, S.; Schnyder, C.C.; Achache, F.; Jonescu-Cuypers, C.; Mermoud, A.; Krieglstein, G. Ultrasound biomicroscopy images: Long-term results after deep sclerectomy with collagen implant. Graefes Arch. Clin. Exp. Ophthalmol. 2002, 240, 918–923. [Google Scholar] [CrossRef]
- Roy, S.; Mermoud, A. Deep Sclerectomy. Dev. Ophthalmol. 2017, 59, 36–42. [Google Scholar] [CrossRef]
- Villamarin, A.; Roy, S.; Bigler, S.; Stergiopulos, N. A new adjustable glaucoma drainage device. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1848–1852. [Google Scholar] [CrossRef]
- Anand, N.; Kumar, A.; Gupta, A. Primary phakic deep sclerectomy augmented with mitomycin C: Long-term outcomes. J. Glaucoma 2011, 20, 21–27. [Google Scholar] [CrossRef]
- Sangtam, T.; Roy, S.; Mermoud, A. Outcome and Complications of Combined Modified Deep Sclerectomy and Trabeculectomy for Surgical Management of Glaucoma: A Pilot Study. Clin. Ophthalmol. 2020, 14, 795–803. [Google Scholar] [CrossRef]
- Harju, M.; Suominen, S.; Allinen, P.; Vesti, E. Long-term results of deep sclerectomy in normal-tension glaucoma. Acta Ophthalmol. 2018, 96, 154–160. [Google Scholar] [CrossRef]
- Laroche, D.; Nkrumah, G.; Ng, C. Real-World Retrospective Consecutive Study of Ab Interno XEN 45 Gel Stent Implant with Mitomycin C in Black and Afro-Latino Patients with Glaucoma: 40% Required Secondary Glaucoma Surgery at 1 Year. Middle East Afr. J. Ophthalmol. 2019, 26, 229–234. [Google Scholar] [CrossRef]
- Gillmann, K.; Bravetti, G.E.; Mansouri, K. Delayed Obstruction of XEN Gel Stent by Cell Debris in Primary Open-angle Glaucoma: A New Insight into the Pathophysiology of Filtration Device Failure. J. Curr. Glaucoma Pract. 2019, 13, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Widder, R.A.; Kuhnrich, P.; Hild, M.; Rennings, C.; Szumniak, A.; Rossler, G.F. Intraocular Degradation of XEN45 Gel Stent 3 Years After its Implantation. J. Glaucoma 2019, 28, e171–e173. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, K.; Bravetti, G.E.; Mermoud, A.; Mansouri, K. Anterior Chamber XEN Gel Stent Movements: The Impact on Corneal Endothelial Cell Density. J. Glaucoma 2019, 28, e93–e95. [Google Scholar] [CrossRef]
- Rulli, E.; Biagioli, E.; Riva, I.; Gambirasio, G.; De Simone, I.; Floriani, I.; Quaranta, L. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: A systematic review and meta-analysis. JAMA Ophthalmol. 2013, 131, 1573–1582. [Google Scholar] [CrossRef]
- Eldaly, M.A.; Bunce, C.; Elsheikha, O.Z.; Wormald, R. Non-penetrating filtration surgery versus trabeculectomy for open-angle glaucoma. Cochrane Database Syst. Rev. 2014, 15, 2. [Google Scholar] [CrossRef]
- Roy, S.; Mermoud, A. Deep sclerectomy. Dev. Ophthalmol. 2012, 50, 29–36. [Google Scholar] [CrossRef]
- Mostafaei, A.; Taheri, N.; Ghojazadeh, M.; Latifi, A.; Moghaddam, N. Comparison of the effect of mitomycin C and bevacizumab-methylcellulose mixture on combined phacoemulsification and non-penetrating deep sclerectomy surgery on the intraocular pressure (a clinical trial study). Int. Ophthalmol. 2019, 39, 2341–2351. [Google Scholar] [CrossRef]
- Paletta Guedes, R.A.; Gravina, D.M.; Paletta Guedes, V.M.; Chaoubah, A. Use of a Collagen Matrix Implant as an Adjuvant in Combined Surgery Involving Phacoemulsification and Nonpenetrating Deep Sclerectomy. J. Glaucoma 2019, 28, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Bhartiya, S.; Dhingra, D.; Shaarawy, T. Revisiting Results of Conventional Surgery: Trabeculectomy, Glaucoma Drainage Devices, and Deep Sclerectomy in the Era of MIGS. J. Curr. Glaucoma Pract. 2019, 13, 45–49. [Google Scholar] [CrossRef]
- Chiou, A.G.; Mermoud, A.; Jewelewicz, D.A. Post-operative inflammation following deep sclerectomy with collagen implant versus standard trabeculectomy. Graefes Arch. Clin. Exp. Ophthalmol. 1998, 236, 593–596. [Google Scholar] [CrossRef]
- Dupas, B.; Fardeau, C.; Cassoux, N.; Bodaghi, B.; LeHoang, P. Deep sclerectomy and trabeculectomy in uveitic glaucoma. Eye 2010, 24, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Siriwardena, D.; Kotecha, A.; Minassian, D.; Dart, J.K.; Khaw, P.T. Anterior chamber flare after trabeculectomy and after phacoemulsification. Br. J. Ophthalmol. 2000, 84, 1056–1057. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, E.; Guidotti, J.M.; Mansouri, K.; Mermoud, A. XEN-augmented Baerveldt: A New Surgical Technique for Refractory Glaucoma. J. Glaucoma 2017, 26, e90–e92. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, F.J.; Sousa, D.C.; Machado, N.M.; Caiado, F.; Barao, R.; Sens, P.; Abegao Pinto, L. XEN-augmented Baerveldt surgical success rate and comparison with the Ahmed Valve. Acta Ophthalmol. 2020, 98, e870–e875. [Google Scholar] [CrossRef]
- Bravetti, G.E.; Mansouri, K.; Gillmann, K.; Rao, H.L.; Mermoud, A. XEN-augmented Baerveldt drainage device implantation in refractory glaucoma: 1-year outcomes. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1787–1794. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Data | Mean ± SD (%) |
|---|---|
| Age (years) | 72.1 ± 8.2 |
| Range | 53–89 |
| Female gender | 10 (66.7%) |
| Study eye | |
| Right | 8 (53.3%) |
| Left | 7 (46.6%) |
| Ethnicity | |
| Caucasian | 12 (80%) |
| Black | 2 (13.3%) |
| Asian | 1 (6.7%) |
| Bilateral cases | 1 |
| Diagnosis | |
| POAG | 5 (33.3%) |
| PEXG | 4 (26.6%) |
| Pigmentary glaucoma | 3 (20%) |
| Other | 3 (20%) |
| Central corneal thickness (μm) | 540.1 ± 53.7 |
| pre-XEN Visual field (dBs) | |
| MD | 5.3 ± 2.9 |
| sLV | 3.9 ± 1.9 |
| pre-XEN OCT RNFL thickness (μm) | 85.6 ± 16.5 |
| pre-XEN BCVA (decimal) | 0.8 ± 0.3 |
| Baseline BCVA (decimal) | 0.9 ± 0.2 |
| pre-XEN IOP (mmHg) | 21.1 ± 3.7 |
| Baseline IOP (mmHg) | 22.6 ± 5.3 |
| pre-XEN Medications | 1.5 ± 1.1 |
| Baseline Medications | 1.1 ± 0.9 |
| Definition | Percentage |
|---|---|
| Complete success (unmedicated) | |
| Intraocular pressure ≤ 12 mmHg | 40 |
| With a reduction of more than 20% from baseline | 40 |
| Intraocular pressure ≤ 15 mmHg | 60 |
| With a reduction of more than 20% from baseline | 60 |
| Intraocular pressure ≤ 18 mmHg | 66.7 |
| With a reduction of more than 20% from baseline | 66.7 |
| Qualified success (medicated) | |
| Intraocular pressure ≤ 12 mmHg | 46.7 |
| With a reduction of more than 20% from baseline | 46.7 |
| Intraocular pressure ≤ 15 mmHg | 66.7 |
| With a reduction of more than 20% from baseline | 66.7 |
| Intraocular pressure ≤ 18 mmHg | 80 |
| With a reduction of more than 20% from baseline | 80 |
| Complete failure | 20 |
| Postoperative Interventions | Percentage |
|---|---|
| Total of needling revisions | 46.7 |
| # 1 needling revision | 85.7 |
| # 2 needling revisions | 14.3 |
| Laser Goniopuncture | 60 |
| Postoperative Complications | Percentage |
|---|---|
| Refractory intraocular hypertension requiring further surgery | 20 |
| Persistent bleb leakage requiring conjunctival sutures | 13.3 |
| Persistent hypotony, defined as IOP persistently <5 mmHg | 6.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravetti, G.E.; Gillmann, K.; Rao, H.L.; Mermoud, A.; Mansouri, K. Outcomes of Deep Sclerectomy following Failed XEN Gel Stent Implantation in Open-Angle Glaucoma: A Prospective Study. J. Clin. Med. 2022, 11, 4784. https://doi.org/10.3390/jcm11164784
Bravetti GE, Gillmann K, Rao HL, Mermoud A, Mansouri K. Outcomes of Deep Sclerectomy following Failed XEN Gel Stent Implantation in Open-Angle Glaucoma: A Prospective Study. Journal of Clinical Medicine. 2022; 11(16):4784. https://doi.org/10.3390/jcm11164784
Chicago/Turabian StyleBravetti, Giorgio Enrico, Kevin Gillmann, Harsha L. Rao, André Mermoud, and Kaweh Mansouri. 2022. "Outcomes of Deep Sclerectomy following Failed XEN Gel Stent Implantation in Open-Angle Glaucoma: A Prospective Study" Journal of Clinical Medicine 11, no. 16: 4784. https://doi.org/10.3390/jcm11164784