
Endoprosthetic Reconstruction in Ewing’s Sarcoma Patients: A Systematic Review of Postoperative Complications and Functional Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Collection
2.4. Quality Assessment
3. Results
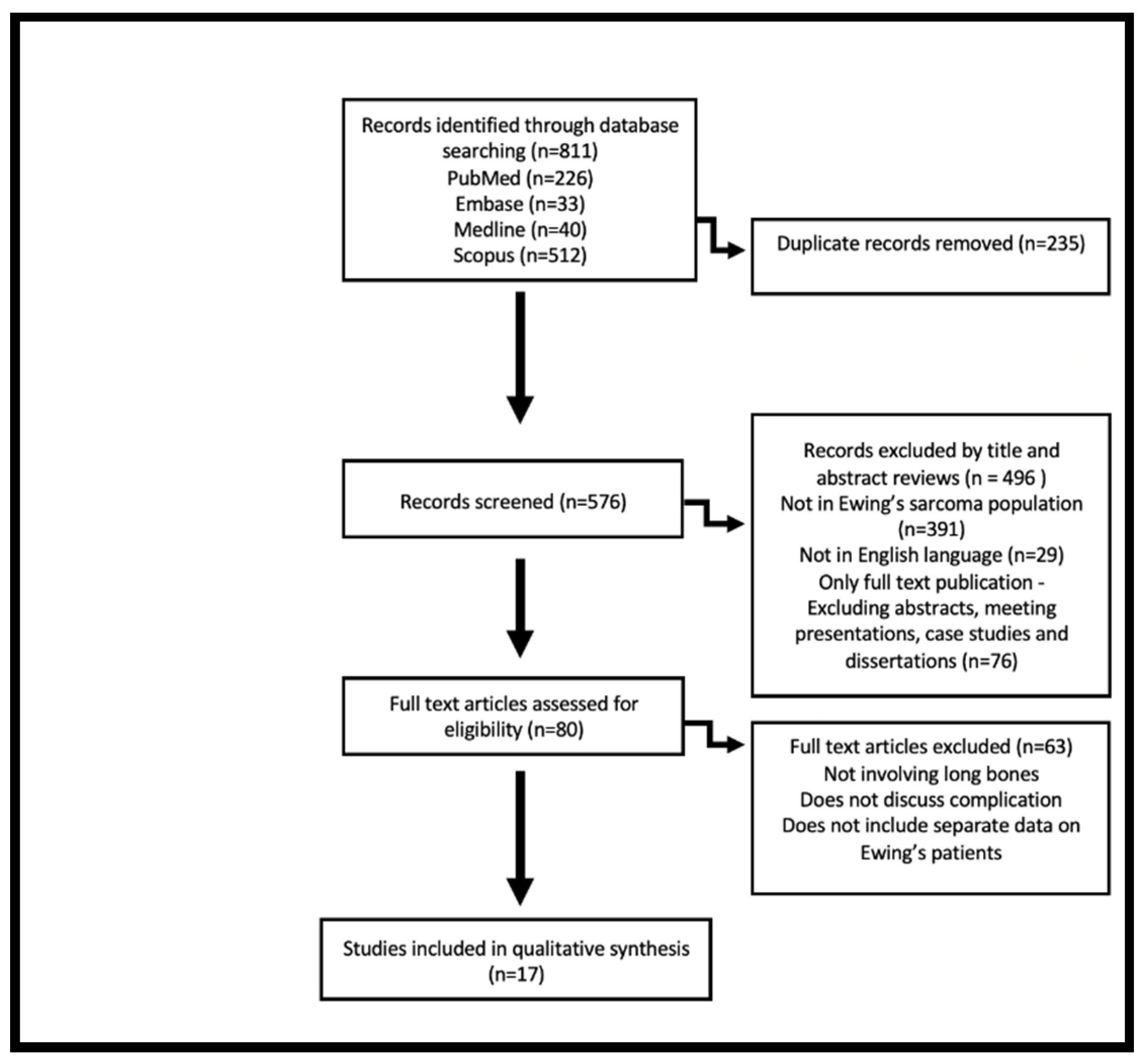
3.1. Search Results
3.2. Design and Content of the Studies
3.3. Postoperative Complications
3.4. Prosthesis Survivorship
3.5. Functional Outcomes
4. Discussion
4.1. Prostheses Comparison
4.2. Outcomes
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bernstein, M.; Kovar, H.; Paulussen, M.; Randall, R.L.; Schuck, A.; Teot, L.A.; Juergens, H. Ewing’s Sarcoma Family of Tumors: Current Management. Oncologist 2006, 11, 503–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sewell, M.D.; Tan, K.A.; Quraishi, N.A.; Preda, C.; Varga, P.P.; Williams, R. Systematic review of En Block Resection in the Management of Ewing’s Sarcoma of the Mobile Spine with respect to Local Control and Disease-Free Survival. Medicine 2015, 94, e109. [Google Scholar] [CrossRef] [PubMed]
- Heare, T.; Hensley, M.A.; Dell’Orfano, S. Bone tumors: Osteosarcoma and Ewing’s sarcoma. Curr. Opin. Pediatr. 2009, 21, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Hanna, S.A.; David, L.A.; Aston, W.J.; Gikas, P.D.; Blunn, G.W.; Cannon, S.R.; Briggs, T.W. Endoprosthetic replacement of the distal humerus following resection of bone tumours. J. Bone Jt. Surg. Br. 2007, 89, 1498–1503. [Google Scholar] [CrossRef] [Green Version]
- Henderson, E.R.; Groundland, J.S.; Pala, E.; Dennis, J.A.; Wooten, R.; Cheong, D.; Windhager, R.; Kotz, R.I.; Mercuri, M.; Funovics, P.T.; et al. Failure mode classification for tumor endoprosthesis: Retrospective review of five institutions and a literature review. J. Bone Jt. Surg. Am. 2011, 93, 418–429. [Google Scholar] [CrossRef]
- Dormand, E.L.; Banwell, P.E.; Goodacre, T.E. Radiotherapy and Wound healing. Int. Wound J. 2005, 2, 112–127. [Google Scholar] [CrossRef]
- Novikov, D.; Cohen, D.; Swanson, D.; Voidani, S.; Khan, F. A Meta-Analysis of Outcomes in Total Hip Arthroplasty Recipients Followic Pelvic Irradiation. J. Arthroplast. 2019, 34, 1546–1552. [Google Scholar] [CrossRef]
- Leachman, B.K.; Galloway, T.J. The Role for Radiation Therapy in the Management of Sarcoma. Surg. Clin. N. Am. 2016, 96, 1127–1139. [Google Scholar] [CrossRef]
- Kapoor, S.K.; Thiyam, R. Management of infection following reconstruction in bone tumors. J. Clin. Orthop. Trauma. 2015, 6, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, J.A. Ewing Sarcoma: Historical perspectives, current state-of-the-art, and opportunities for targeted therapy in the future. Curr. Opin. Oncol. 2008, 20, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Gerrand, C.; Athanasou, N.; Brennan, B.; Grimer, R.; Judson, I.; Morland, B.; Peake, D.; Seddon, B.; Whelan, J.; On behalf of the British Sarcoma Group. UK guidelines for the management of bone sarcomas. Clin Sarcoma Res. 2016, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation [published correction appears in BMJ. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connel, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Feb 2009. Available online: http://wwwohrica/programs/clinical_epidemiology/oxfordhtm (accessed on 12 February 2022).
- Benevenia, J.; Patterson, F.; Beebe, K.; Tucker, K.; Moore, J.; Ippolito, J.; Rivero, S. Results of 20 consecutive patients treated with Repiphysis expandable prosthesis for primary malignant bone. SpringerPlus 2015, 4, 793. [Google Scholar] [CrossRef] [Green Version]
- Vijayan, S.; Bartlett, W.; Lee, R.; Ostler, P.; Blunn, G.W.; Cannon, S.R.; Briggs, T.W. Use of irradiated autologous bone in joint sparing endoprosthetic femoral replacement tumor surgery. Indian J. Orthop. 2011, 45, 161–167. [Google Scholar] [CrossRef]
- Torner, F.; Segur, J.M.; Ullot, R.; Soldado, F.; Domenech, P.; DeSena, L.; Knorr, J. Non-invasive expandable prosthesis in musculoskeletal oncology paediatric patients for the distal and proximal femur. First results. Int. Orthop. 2016, 40, 1683–1688. [Google Scholar] [CrossRef]
- Hanna, S.A.; Sewell, M.D.; Aston, W.J.; Pollock, R.C.; Skinner, J.A.; Cannon, S.R.; Briggs, T.W. Femoral diaphyseal endoprosthetic reconstruction after segmental resection of primary bone tumours. J. Bone Jt. Surg. Br. 2010, 92, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.; Evans, S.; Khan, Z.; Abudu, A.; Jeys, L.; Grimer, R. Reconstruction of the distal tibia following resection of aggressive bone tumours using a custom-made megaprosthesis. J. Orthop. 2017, 14, 406–409. [Google Scholar] [CrossRef]
- Schiller, C.; Windhager, R.; Fellinger, E.J.; Salzer-Kuntschik, M.; Kaider, A.; Kotz, R. Extendable tumour endoprostheses for the leg in children. J. Bone Jt. Surg. Br. 1995, 77, 608–614. [Google Scholar] [CrossRef] [Green Version]
- Dotan, A.; Dadia, S.; Bickels, J.; Nirkin, A.; Flusser, G.; Issakov, J.; Neumann, Y.; Cohen, I.; Ben-Arush, M.; Kollender, Y.; et al. Expandable endoprosthesis for limb-sparing surgery in children: Long-term results. J. Child. Orthop. 2010, 4, 391–400. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, Y.; Osaka, S.; Tokuhashi, Y. Experience with extendable prostheses for malignant bone tumors in children. J. Formos. Med. Assoc. 2011, 110, 711–715. [Google Scholar] [CrossRef] [Green Version]
- Shekkeris, A.S.; Hanna, S.A.; Sewell, M.D.; Spiegelberg, B.G.; Aston, W.J.; Blunn, G.W.; Cannon, S.R.; Briggs, T.W. Endoprosthetic reconstruction of the distal tibia and ankle joint after resection of primary bone tumours. J. Bone Jt. Surg. Br. 2009, 91, 1378–1382. [Google Scholar] [CrossRef]
- Raciborska, A.; Bilska, K.; Malesza, I.; Rodriguez-Galindo, C.; Pachuta, B. Distal Tibial Recontruction in the Management of Primary Bone Tumors in Children and Adoloscents. Foot Ankle Int. 2021, 42, 1447–1453. [Google Scholar] [CrossRef]
- Yoshida, Y.; Iwata, S.; Ueda, T.; Kawai, A.; Isu, K.; Ryu, J. Current state of extendable prostheses for the lower limb in Japan. Surg. Oncol. 2008, 17, 65–71. [Google Scholar] [CrossRef]
- Erol, B.; Sofulu, O.; Sirin, E.; Saglam, F.; Buyuktopcu, O. Reconstruction after periacetabular tumor resection with Lumic® endoprosthesis: What are the midterm results? J. Surg. Oncol. 2021, 123, 532–543. [Google Scholar] [CrossRef]
- Puri, A.; Gulia, A.; Chan, W.H. Functional and oncologic outcomes after excision of the total femur in primary bone tumors: Results with a low cost total femur prosthesis. Indian J. Orthop. 2012, 46, 470–474. [Google Scholar] [CrossRef]
- Ayoub, K.S.; Firenze, F.; Grime, R.J.; Tillman, R.M.; Carter, S.R. Extensible endoprostheses of the humerus after resection of bone tumours. J. Bone Jt. Surg. Br. 1999, 81, 495–500. [Google Scholar] [CrossRef]
- Wafer, H.; Reddy, K.; Grimmer, R.; Abdu, A.; Jesy, L.; Carter, S.; Tillman, R. Does total humeral endoprosthetic replacement provide reliable reconstruction with preservation of a useful extremity? Clin. Orthop. Relat. Res. 2015, 473, 917–925. [Google Scholar] [CrossRef] [Green Version]
- Ji, T.; Yang, Y.; Li, D.S.; Tang, X.D.; Guo, W. Limb Salvage Using Non-hinged Endoprosthesis and Staged Correction of Leg-length Discrepancy for Children with Distal Femoral Malignant Tumors. Orthop. Surg. 2019, 11, 819–825. [Google Scholar] [CrossRef]
- Lewis, M.M. The use of an expandable and adjustable prosthesis in the treatment of childhood malignant bone tumors of the extremity. Cancer 1986, 57, 499–502. [Google Scholar] [CrossRef]
- Mankin, H.J.; Hornicek, F.J.; Harris, M. Total femur replacement procedures in tumor treatment. Clin. Orthop. Relat. Res. 2005, 438, 60–64. [Google Scholar] [CrossRef]
- Sewell, M.D.; Spiegelberg, B.G.; Hanna, S.A.; Aston, W.J.; Bartlett, W.; Blunn, G.W.; David, L.A.; Cannon, S.R.; Briggs, T.W. Total femoral endoprosthetic replacement following excision of bone tumours. J. Bone Jt. Surg. Br. 2009, 91, 1513–1529. [Google Scholar] [CrossRef]
- Hosalkar, H.S.; Dormans, J.P. Limb sparing surgery for pediatric musculoskeletal tumors. Pediatr. Blood Cancer 2004, 42, 295–310. [Google Scholar] [CrossRef]
- Eckardt, J.J.; Kabo, J.M.; Kelley, C.M.; Ward WGSr Asavamongkolkul, A.; Wirganowicz, P.Z.; Yang, R.S.; Eilber, F.R. Expandable endoprosthesis reconstruction in skeletally immature patients with tumors. Clin. Orthop. Relat. Res. 2000, 373, 51–61. [Google Scholar] [CrossRef]
- Schuck, A.; Ahrens, S.; Paulussen, M.; Kuhlen, M.; Könemann, S.; Rübe, C.; Winkelmann, W.; Kotz, R.; Dunst, J.; Willich, N.; et al. Local therapy in localized Ewing tumors; results of 1058 patients treated in the CESS 81, CESS 86, and EICESS 92 trials. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 168–177. [Google Scholar] [CrossRef]
- Ozaki, T. Diagnosis and treatment of Ewing sarcoma of the bone: A review article. J. Orthop. Sci. 2015, 20, 250–263. [Google Scholar] [CrossRef] [Green Version]
- Longhi, A.; Ferrari, S.; Tamburini, A.; Luksch, R.; Fagioli, F.; Bacci, G.; Ferrari, C. Late effects of chemotherapy and radiotherapy in osteosarcoma and Ewing sarcoma patients: The Italian Sarcoma Group Experience (1983–2006). Cancer 2012, 118, 5050–5059. [Google Scholar] [CrossRef] [Green Version]
- Dunst, J.; Ahrens, S.; Paulussen, M.; Rübe, C.; Winkelmann, W.; Zoubek, A.; Harms, D.; Jürgens, H. Second malignancies after treatment for Ewing’s sarcoma: A report of the CESS-studies. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 379–384. [Google Scholar] [CrossRef]
- Abu-Amer, Y.; Darwech, I.; Clohisy, J.C. Aseptic loosening of total joint replacements: Mechanisms underlying osteolysis and potential therapies. Arthritis Res. Ther. 2007, 9 (Suppl. S1), S6. [Google Scholar] [CrossRef] [Green Version]
- Graci, C.; Maccauro, G.; Muratori, F.; Spinelli, M.S.; Rosa, M.A.; Fabbriciani, C. Infection following bone tumor resection and reconstruction with tumoral prostheses: A literature review. Int. J. Immunopathol. Pharm. 2010, 23, 1005–1013. [Google Scholar] [CrossRef] [Green Version]
- Jeys, L.M.; Grimer, R.J.; Carter, S.R.; Tilman, R.M. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J. Bone Jt. Surg. Am. 2005, 87, 842–849. [Google Scholar] [CrossRef]
- Picardo, N.E.; Blunn, G.W.; Shekkeris, A.S.; Meswania, J.; Aston, W.J.; Pollock, R.C.; Skinner, J.A.; Cannon, S.R.; Briggs, T.W. The medium-term results of the Stanmore non-invasive extendible endoprosthesis in the treatment of paediatric bone tumors. J. Bone Jt. Surg. Br. 2012, 94, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Hardes, J.; Henrichs, M.P.; Hauschild, G.; Nottrott, M.; Guder, W.; Streitbuerger, A. A Silver-Coated Megaprosthesis of the Proximal Tibia in Patients with Sarcoma. J. Arthroplast. 2017, 32, 2208–2213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, K.; Racano, A.; Deheshi, B.; Farrokhyar, F.; Wunder, J.; Ferguson, P.; Holt, G.; Schwartz, H.; Petrisor, B.; Bhandari, M.; et al. Prophylactic antibiotic regimens in tumor surgery (PARITY) surgery. BMC Musculoskelet. Disord. 2012, 13, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, S.J.; van Rein, E.A.; Paulino Pereira, N.R.; Raskin, K.A.; Ferrone, M.L.; Hornicek, F.J.; Lozano-Calderon, S.A.; Schwab, J.H. The Discrepancy between Patient and Clinician Reported Function in Extremetiy Bone Metastases. Sarcoma 2016, 2016, 1014248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimer, R.J.; Taminiau, A.M.; Cannon, S.R. Surgical Subcommitte of the Europena Osteosarcoma Intergroup. Surgical outcomes in osteosarcoma. J. Bone Jt. Surg. Br. 2002, 85, 395–400. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Selection | Comparability | Outcome | Quality Based on AHRQ * |
|---|---|---|---|---|
| Benevenia 2015 [14] | ★★ | ★ | ★★★ | Fair |
| Vijayan 2011 [15] | ★★★ | ★★ | ★★★ | Good |
| Torner 2016 [16] | ★★★ | ★★ | ★★★ | Good |
| Hanna 2010 [17] | ★★★ | ★ | ★★★ | Good |
| Yang 2017 [18] | ★★★ | ★ | ★★★ | Good |
| Schiller 1995 [19] | ★★★ | ★★ | ★★★ | Good |
| Dotan 2010 [20] | ★★★ | ★ | ★★★ | Good |
| Yoshida 2011 [21] | ★★★ | ★ | ★★★ | Good |
| Shekkeris 2009 [22] | ★★★ | ★ | ★★★ | Good |
| Raciborska 2021 [23] | ★★★ | ★★ | ★★★ | Good |
| Yoshida 2008 [24] | ★★★ | ★★ | ★★★ | Good |
| Erol 2021 [25] | ★★★ | ★ | ★★★ | Good |
| Puri 2012 [26] | ★★★ | ★ | ★★ | Fair |
| Ayoub 1999 [27] | ★★★ | ★★ | ★★ | Good |
| Wafa 2015 [28] | ★★★ | ★ | ★★★ | Good |
| Ji 2019 [29] | ★★★ | ★★ | ★★★ | Good |
| Lewis 1986 [30] | ★★★ | ★ | ★★★ | Good |
| Author, Year | N | Age Range | Prosthesis | Complications | Mean FS |
|---|---|---|---|---|---|
| Benevenia, 2015 [14] | 2 | 11–16 | Repiphysis | Contracture×2, | 95%(MSTS) |
| Deep Infection | |||||
| Vijayan, 2011 [15] | 1 | 4 | Stanmore | Joint instability, flexion deformities | - |
| Torner, 2016 [16] | 1 | 12 | MUTARS | - | 86% (MSTS) |
| Hanna, 2010 [17] | 3 | 10–25 | Stanmore | Deep infection | 79.7% (MSTS) |
| Yang, 2017 [18] | 1 | 26 | Stanmore | - | 67% (MSTS) |
| Schiller, 1995 [19] | 1 | 9 | HMRS | Deep infection, joint instability | - |
| Dotan, 2010 [20] | 12 | 6–14 | Kotz | Superficial infection ×4, Deep infection ×5, Contracture ×3, Mechanical failure ×2, Wound dehiscence, Dislocation ×2, Aseptic Loosening ×3, Periprosthetic fracture, Amputation due to local recurrence | Good (AMSTS) |
| Yoshida, 2011 [21] | 1 | 12 | Kotz | Amputation due to local recurrence | 88% (ISOLS) |
| Shekkeris, 2009 [22] | 2 | 15–42 | Stanmore | - | 76.5% (MSTS) |
| Raciborska, 2021 [23] | 4 | 6–18 | MUTARS | - | 73% (MSTS) |
| Yoshida, 2008 [24] | 3 | 7–12 | Stanmore + Kotz | - | 73.6% (Enneking) |
| Erol, 2021 [25] | 6 | 17–46 | LUMiC | Amputation due to local recurrence, Dislocation | 67.7% (MSTS) |
| Puri, 2012 [26] | 1 | 17 | RESTOR | - | 80% (MSTS) |
| Ayoub, 1999 [27] | 8 | 6–11 | Stanmore | Wound dehiscence, | 80% (Enneking) |
| Radial nerve palsy, Amputation for pain | |||||
| Wafa, 2015 [28] | 7 | 7–32 | Stanmore | Superficial wound infection, Periprosthetic infection | 82.9% (MSTS) |
| Ji, 2019 [29] | 2 | 9–10 | Non-hinged CCK | - | 77% (MSTS) |
| Lewis, 1986 [30] | 2 | 10–13 | Lewis | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu El Afieh, J.; Gray, M.; Seah, M.; Khan, W. Endoprosthetic Reconstruction in Ewing’s Sarcoma Patients: A Systematic Review of Postoperative Complications and Functional Outcomes. J. Clin. Med. 2022, 11, 4612. https://doi.org/10.3390/jcm11154612
Abu El Afieh J, Gray M, Seah M, Khan W. Endoprosthetic Reconstruction in Ewing’s Sarcoma Patients: A Systematic Review of Postoperative Complications and Functional Outcomes. Journal of Clinical Medicine. 2022; 11(15):4612. https://doi.org/10.3390/jcm11154612
Chicago/Turabian StyleAbu El Afieh, Jude, Marena Gray, Matthew Seah, and Wasim Khan. 2022. "Endoprosthetic Reconstruction in Ewing’s Sarcoma Patients: A Systematic Review of Postoperative Complications and Functional Outcomes" Journal of Clinical Medicine 11, no. 15: 4612. https://doi.org/10.3390/jcm11154612