
Vacuum-Implemented Removal of Lead Vegetations in Cardiac Device-Related Infective Endocarditis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
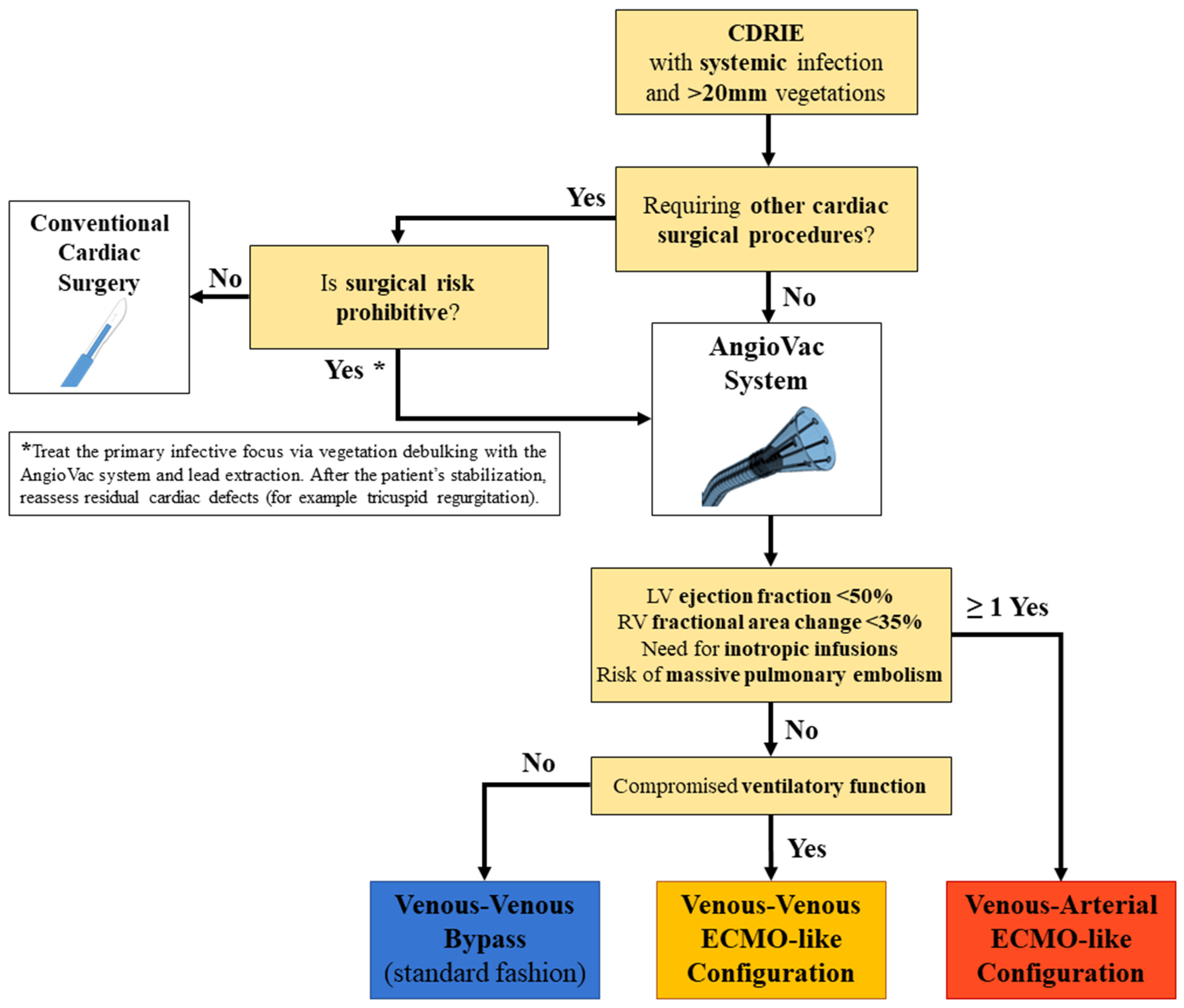
2.2. Procedure Planning
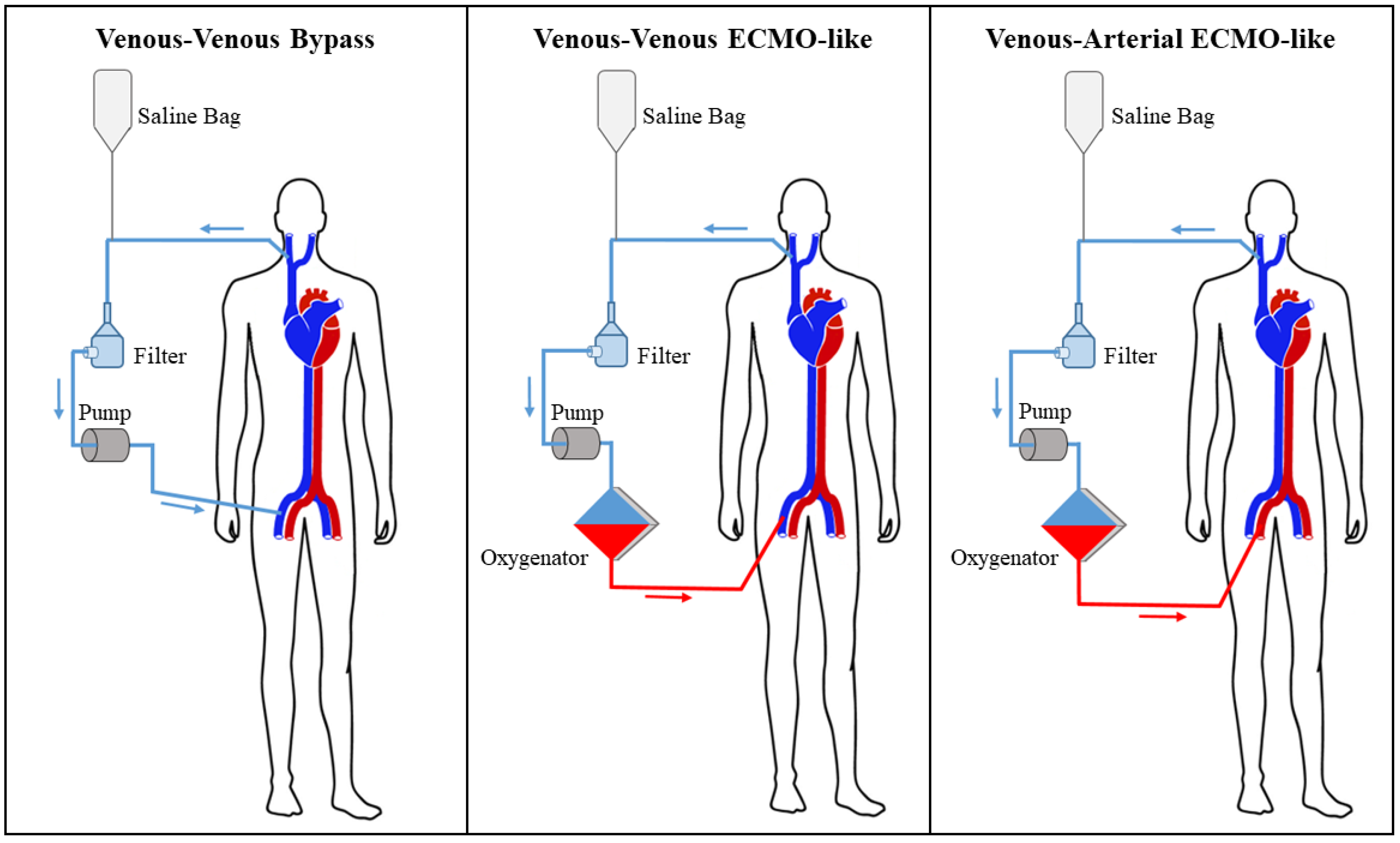
2.3. Operative Technique
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CDRIE | cardiac device-related infective endocarditis |
| CRT-D | cardiac resynchronization therapy-defibrillator |
| ECMO | extracorporeal membrane oxygenation |
| ICD | implantable cardioverter-defibrillator |
| IQR | interquartile range |
| LFV | left femoral vein |
| PM | pacemaker |
| RFV | right femoral vein |
| RIJV | right internal jugular vein |
| SD | standard deviation |
References
- Greenspon, A.J.; Patel, J.D.; Lau, E.; Ochoa, J.A.; Frisch, D.R.; Ho, R.T.; Pavri, B.B.; Kurtz, S.M. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J. Am. Coll. Cardiol. 2011, 58, 1001–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsubara, T.; Sumiyoshi, M.; Kimura, A.; Minami-Takano, A.; Maruyama, K.; Kimura, Y.; Tabuchi, H.; Hayashi, H.; Odagiri, F.; Sekita, G.; et al. Trend in Age at the Initial Pacemaker Implantation in Patients With Bradyarrhythmia―A 50-Year Analysis (1970–2019) in Japan. Circ. J. 2022, 86, CJ-21. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jędrzejczyk-Patej, E.; Mazurek, M.; Kowalski, O.; Sokal, A.; Kozieł, M.; Adamczyk, K.; Przybylska-Siedlecka, K.; Morawski, S.; Liberska, A.; Szulik, M.; et al. Device-related infective endocarditis in cardiac resynchronization therapy recipients—Single center registry with over 2500 person-years follow up. Int. J. Cardiol. 2017, 227, 18–24. [Google Scholar] [CrossRef]
- Blomström-Lundqvist, C.; Traykov, V.; Erba, P.A.; Burri, H.; Nielsen, J.C.; Bongiorni, M.G.; Poole, J.; Boriani, G.; Costa, R.; Deharo, J.C.; et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections—Endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID), and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 41, 2012–2032. [Google Scholar]
- Diemberger, I.; Segreti, L.; Rinaldi, C.A.; Svendsen, J.H.; Kutarski, A.; Younis, A.; Laroche, C.; Leclercq, C.; Małecka, B.; Mitkowski, P.; et al. Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes-An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy. Biology 2022, 11, 615. [Google Scholar] [CrossRef]
- Starck, C.T.; Dreizler, T.; Falk, V. The AngioVac system as a bail-out option in infective valve endocarditis. Ann. Cardiothorac. Surg. 2019, 8, 675–677. [Google Scholar] [CrossRef] [Green Version]
- Tarzia, V.; Tessari, C.; Bagozzi, L.; Migliore, F.; Pittarello, D.; Zanella, F.; Bertaglia, E.; Fabozzo, A.; Gerosa, G. Totally peripheral approach for ICD lead vegetation removal in a GUCH patient. J. Cardiovasc. Electrophysiol. 2021, 32, 1778–1781. [Google Scholar] [CrossRef]
- Kiani, S.; Sabayon, D.; Lloyd, M.S.; Hoskins, M.H.; El-Chami, M.F.; Westerman, S.; Vadlamudi, R.; Keeling, B.; Lattouf, O.M.; Merchant, F.M. Outcomes of percutaneous vacuum-assisted debulking of large vegetations as an adjunct to lead extraction. Pacing Clin. Electrophysiol. 2019, 42, 1032–1037. [Google Scholar] [CrossRef]
- Schaerf, R.H.M.; Najibi, S.; Conrad, J. Percutaneous Vacuum-Assisted Thrombectomy Device Used for Removal of Large Vegetations on Infected Pacemaker and Defibrillator Leads as an Adjunct to Lead Extraction. J. Atr. Fibrillation 2016, 9, 1455. [Google Scholar] [CrossRef] [Green Version]
- Godara, H.; Jia, K.Q.; Augostini, R.S.; Houmsse, M.; Okabe, T.; Hummel, J.D.; Weiss, R.; Kalbfleisch, S.J.; Afzal, M.R.; Badin, A.; et al. Feasibility of concomitant vacuum-assisted removal of lead-related vegetations and cardiac implantable electronic device extraction. J. Cardiovasc. Electrophysiol. 2018, 29, 1460–1466. [Google Scholar] [CrossRef]
- Richardson, T.D.; Lugo, R.M.; Crossley, G.H.; Ellis, C.R. Use of a clot aspiration system during transvenous lead extraction. J. Cardiovasc. Electrophysiol. 2020, 31, 718–722. [Google Scholar] [CrossRef]
- Starck, C.T.; Schaerf, R.H.; Breitenstein, A.; Najibi, S.; Conrad, J.; Berendt, J.; Esmailian, F.; Eulert-Grehn, J.; Dreizler, T.; Falk, V. Transcatheter aspiration of large pacemaker and implantable cardioverter-defibrillator lead vegetations facilitating safe transvenous lead extraction. EP Eur. 2020, 22, 133–138. [Google Scholar] [CrossRef]
- Patel, N.; Azemi, T.; Zaeem, F.; Underhill, D.; Gallagher, R.; Hagberg, R.; Sadiq, I. Vacuum assisted vegetation extraction for the management of large lead vegetations. J. Card. Surg. Incl. Mech. Biol. Support Heart Lungs 2013, 28, 321–324. [Google Scholar] [CrossRef]
- Rusia, A.; Shi, A.J.; Doshi, R.N. Vacuum-assisted vegetation removal with percutaneous lead extraction: A systematic review of the literature. J. Interv. Card. Electrophysiol. 2019, 55, 129–135. [Google Scholar] [CrossRef]
- Moriarty, J.M.; Rueda, V.; Liao, M.; Kim, G.H.J.; Rochon, P.J.; Zayed, M.A.; Lasorda, D.; Golowa, Y.S.; Shavelle, D.M.; Dexter, D.J. Endovascular Removal of Thrombus and Right Heart Masses Using the AngioVac System: Results of 234 Patients from the Prospective, Multicenter Registry of AngioVac Procedures in Detail (RAPID). J. Vasc. Interv. Radiol. 2021, 32, 549–557.e3. [Google Scholar] [CrossRef]
- Migliore, F.; Tarzia, V.; Dall’Aglio, P.B.; Falzone, P.V.; De Lazzari, M.; Bottio, T.; D’Onofrio, A.; Padalino, M.; Vida, V.; Rosso, J.; et al. The valuable interaction among cardiac surgeon and electrophysiologist for transvenous rotational mechanical lead extraction. Pacing Clin. Electrophysiol. 2022, 45, 92–102. [Google Scholar] [CrossRef]
- Arshad, V.; Talha, K.M.; Baddour, L.M. Epidemiology of infective endocarditis: Novel aspects in the twenty-first century. Expert Rev. Cardiovasc. Ther. 2022, 20, 45–54. [Google Scholar] [CrossRef]
- Modi Atig, A.; Alhamad, Y.I.; Alanizi, F.S.; Ardah, H.I.; Alanazi, H. Retrospective study of post-operative infections in implantable cardiac devices in a cardiac tertiary care center. Ann. Saudi Med. 2022, 42, 58–63. [Google Scholar] [CrossRef]
- Lee, J.Z.; Majmundar, M.; Kumar, A.; Thakkar, S.; Patel, H.P.; Sorajja, D.; Valverde, A.M.; Kalra, A.; Cha, Y.M.; Mulpuru, S.K.; et al. Impact of timing of transvenous lead removal on outcomes in infected cardiac implantable electronic devices. Heart Rhythm 2022, 19, 768–775. [Google Scholar] [CrossRef]
- Gerosa, G.; Longinotti, L.; Bagozzi, L.; D’Onofrio, A.; Zanella, F.; Pittarello, D.; Tarzia, V. Transapical Aspiration of a Mitral Mass With the AngioVac System on a Beating Heart. Ann. Thorac. Surg. 2020, 110, e445–e447. [Google Scholar] [CrossRef]
- Gerosa, G.; Bagozzi, L.; Tessari, C.; Pittarello, D.; Zanella, F.; Mancini, M.; Prayer-Galetti, T.; Cillo, U.; Zattoni, F.; Tarzia, V. Proof of Concept: Microinvasive AngioVac Approach in Renal Cell Carcinoma With Atrial Thrombosis. Ann. Thorac. Surg. 2021, 112, e193–e196. [Google Scholar] [CrossRef]
- Tarzia, V.; Gerosa, G. The Rules of Medical Innovation: Experience, Creativity, and Courage: Reply. Ann. Thorac. Surg. 2021, 112, 2113–2114. [Google Scholar] [CrossRef]
- Ruttmann, E.; Hangler, H.B.; Kilo, J.; Höfer, D.; Müller, L.C.; Hintringer, F.; MÜLler, S.; Laufer, G.; Antretter, H. Transvenous pacemaker lead removal is safe and effective even in large vegetations: An analysis of 53 cases of pacemaker lead endocarditis. Pacing Clin. Electrophysiol. 2006, 29, 231–236. [Google Scholar] [CrossRef]
- Grammes, J.A.; Schulze, C.M.; Al-Bataineh, M.; Yesenosky, G.A.; Saari, C.S.; Vrabel, M.J.; Horrow, J.; Chowdhury, M.; Fontaine, J.M.; Kutalek, S.P. Percutaneous pacemaker and implantable cardioverter-defibrillator lead extraction in 100 patients with intracardiac vegetations defined by transesophageal echocardiogram. J. Am. Coll. Cardiol. 2010, 55, 886–894. [Google Scholar] [CrossRef] [Green Version]
- Meier-Ewert, H.K.; Gray, M.-E.; John, R.M. Endocardial pacemaker or defibrillator leads with infected vegetations: A single-center experience and consequences of transvenous extraction. Am. Heart J. 2003, 146, 339–344. [Google Scholar] [CrossRef]
- Klug, D.; Lacroix, D.; Savoye, C.; Goullard, L.; Grandmougin, D.; Hennequin, J.L.; Kacet, S.; Lekieffre, J. Systemic infection related to endocarditis on pacemaker leads: Clinical presentation and management. Circulation 1997, 95, 2098–2107. [Google Scholar] [CrossRef]
- Arora, Y.; Perez, A.A.; Carrillo, R.G. Influence of vegetation shape on outcomes in transvenous lead extractions: Does shape matter? Hear Rhythm 2020, 17, 646–653. [Google Scholar] [CrossRef]
- Caiati, C.; Pollice, P.; Lepera, M.E.; Favale, S. Pacemaker Lead Endocarditis Investigated with Intracardiac Echocardiography: Factors Modulating the Size of Vegetations and Larger Vegetation Embolic Risk during Lead Extraction. Antibiot 2019, 8, 228. [Google Scholar] [CrossRef] [Green Version]
- Pérez-García, C.N.; Olmos, C.; Islas, F.; Marcos-Alberca, P.; Pozo, E.; Ferrera, C.; García-Arribas, D.; Perez de Isla, L.; Vilacosta, I. Morphological characterization of vegetation by real-time three-dimensional transesophageal echocardiography in infective endocarditis: Prognostic impact. Echocardiography 2019, 36, 742–751. [Google Scholar] [CrossRef]
- Hameed, I.; Lau, C.; Khan, F.M.; Wingo, M.; Rahouma, M.; Leonard, J.R.; Di Franco, A.; Worku, B.M.; Salemi, A.; Girardi, L.N.; et al. AngioVac for extraction of venous thromboses and endocardial vegetations: A meta-analysis. J. Card. Surg. 2019, 34, 170–180. [Google Scholar] [CrossRef] [PubMed]
- George, B.; Voelkel, A.; Kotter, J.; Leventhal, A.; Gurley, J. A novel approach to percutaneous removal of large tricuspid valve vegetations using suction filtration and veno-venous bypass: A single center experience. Catheter. Cardiovasc. Interv. 2017, 90, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Döring, M.; Richter, S.; Hindricks, G. The Diagnosis and Treatment of Pacemaker-Associated Infection. Dtsch. Ärzteblatt Int. 2018, 115, 445–452. [Google Scholar] [CrossRef]
- Krishnan, B.; Lassig, J.; Narashiman, C.; Simonson, J.; Shultz, J. Use of vacuum-assisted aspiration for removal of vegetations during transvenous lead extraction. HeartRhythm Case Rep. 2021, 7, 170–173. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 13) | ||
|---|---|---|
| Mean (SD) | Median (IQR) | |
| Age (years) | 63.6 (12.2) | 67.1 (55.8–73.6) |
| Weight (kg) | 73.9 (10.2) | 76 (66.5–81) |
| Height (m) | 1.73 (0.06) | 1.72 (1.70–1.76) |
| Body surface area (m²) | 1.87 (0.13) | 1.88 (1.77–1.97) |
| Body mass index (kg/m²) | 24.6 (3.4) | 25.1 (21.1–26.3) |
| Serum creatinine (mg/dL) | 1.12 (0.88) | 0.87 (0.83–1) |
| Hemoglobin (g/L) | 11.1 (1.9) | 10.2 (9.7–12.7) |
| Left ventricular ejection fraction | 0.43 (0.13) | 0.36 (0.35–0.54) |
| Right ventricular fractional area change | 0.42 (0.11) | 0.41 (0.33–0.52) |
| Time from device implantation (years) | 5.7 (5.7) | 5 (0.9–9.4) |
| Number of infected leads | 2 (1) | 2 (1–3) |
| Mass dimension (mm) | 37.2 (18.6) | 39 (26–40.5) |
| MELD score | 11 (5) | 9 (8–12) |
| Karnofsky scale | 71 (20) | 70 (60–90) |
| Zubrod scale | 2 (1) | 2 (1–3) |
| N | % | |
| Male | 13 | 100 |
| Comorbidities | ||
| Dyslipidemia | 8 | 61.5 |
| Arterial hypertension | 6 | 46.2 |
| Previous cardiac arrest | 5 | 38.5 |
| Smoke | 4 | 30.8 |
| Diabetes mellitus | 4 | 30.8 |
| Congestive heart failure | 2 | 15.4 |
| Renal replacement therapy | 1 | 7.7 |
| Previous cerebrovascular accident | 1 | 7.7 |
| Coronary artery disease | 1 | 7.7 |
| Previous cardiac surgery | 2 | 15.4 |
| Previous percutaneous coronary intervention | 4 | 30.8 |
| Preoperative anticoagulation | 6 | 46.2 |
| Preoperative antiplatelet therapy | 5 | 38.5 |
| Positive blood culture | 8 | 61.5 |
| Preoperative inotropic support | 1 | 7.7 |
| Preoperative tricuspid valve regurgitation | ||
| Absent | 3 | 23.1 |
| Mild | 5 | 38.5 |
| Moderate | 3 | 23.1 |
| Severe | 2 | 15.4 |
| Type of implanted device | ||
| Implantable cardioverter-defibrillator | 7 | 53.8 |
| CRT-D | 4 | 30.8 |
| Pacemaker | 2 | 15.2 |
| Indication to implantation | ||
| Secondary prevention of cardiac arrest | 6 | 46.2 |
| Primary prevention of cardiac arrest | 5 | 38.5 |
| Symptomatic atrio-ventricular block | 2 | 15.2 |
| Number of masses | ||
| One mass | 9 | 69.2 |
| Two masses | 3 | 23.1 |
| Three masses | 1 | 7.7 |
| Isolated Germs from Preoperative Blood Cultures | Patients with Positive Blood Cultures (n = 8) | |
|---|---|---|
| N | % | |
| Staphylococcus epidermidis | 2 | 25 |
| Enterobacter cloacae | 2 | 25 |
| Enterobacter faecalis | 1 | 12.5 |
| Acinetobacter baumanii | 1 | 12.5 |
| Staphylococcus aureus | 1 | 12.5 |
| Staphylococcus lugdunensis | 1 | 12.5 |
| Isolated Germs from Intraoperative Samples | Patients with Positive Intraoperative Samples (n = 3) | |
| N | % | |
| Staphylococcus epidermidis | 1 | 33.3 |
| Staphylococcus warneri | 1 | 33.3 |
| Rhizobium radiobacter | 1 | 33.3 |
| Overall (n = 13) | ||
|---|---|---|
| Mean (SD) | Median (IQR) | |
| Total operative time (min) | 237 (91) | 230 (173–328) |
| Fluoroscopy time (min) | 7.8 (5.8) | 7.1 (2.7–13.7) |
| AngioVac time: cannulation, aspiration, decannulation (min) | 95 (25) | 90 (65–120) |
| N | % | |
| Cannula generation | ||
| First generation | 3 | 23.1 |
| Second generation | 5 | 38.5 |
| Third generation | 5 | 38.5 |
| Venous–venous bypass configuration | 6 | 46.2 |
| Aspiration cannula site | ||
| RFV | 3 | 50 |
| RIJV | 2 | 33.3 |
| RFV + RIJV | 1 | 16.7 |
| Reinfusion cannula site | ||
| LFV | 4 | 66.7 |
| RFV | 2 | 33.3 |
| Venous–venous ECMO-like configuration | 5 | 38.5 |
| Aspiration cannula site | ||
| RFV | 2 | 40 |
| RIJV | 1 | 20 |
| LFV | 1 | 20 |
| Right atrium | 1 | 20 |
| Reinfusion cannula site | ||
| LFV | 4 | 80 |
| RFV | 1 | 20 |
| Venous–arterial ECMO-like configuration | 2 | 15.4 |
| Aspiration cannula site | ||
| RFV | 2 | 100 |
| Reinfusion cannula site | ||
| RFA | 2 | 100 |
| Type of lead removal | ||
| Mechanical removal | 8 | 61.5 |
| Manual removal | 5 | 38.5 |
| Histopathological analysis | ||
| Thrombus | 13 | 100 |
| Successful aspiration | 12 | 92.3 |
| Procedure Survivors (n = 13) | ||
|---|---|---|
| Mean (SD) | Median (IQR) | |
| Creatinine peak (mg/dL) | 1.23 (0.56) | 1.02 (0.83–1.62) |
| Hemoglobin nadir (g/L) | 10.8 (1.3) | 11.1 (9.5–11.6) |
| Left ventricular ejection fraction | 0.44 (0.11) | 0.40 (0.36–0.55) |
| Right ventricular fractional area change | 0.38 (0.07) | 0.40 (0.34–0.44) |
| Intensive care unit stay (days) | 5 (8) | 3 (1–4) |
| Total hospital stay (days) | 26 (21) | 21 (16–30) |
| Karnofsky scale at discharge | 75 (31) | 90 (70–95) |
| Zubrod scale at discharge | 2 (1) | 1 (1–3) |
| N | % | |
| Acute kidney injury | 4 | 30.8 |
| Renal replacement therapy | 4 | 30.8 |
| New-onset atrial fibrillation | 2 | 15.4 |
| Access site injury | 1 | 7.7 |
| Tricuspid valve replacement | 1 | 7.7 |
| Postoperative ECMO support | 1 | 7.7 |
| Tricuspid valve regurgitation at discharge | ||
| Absent | 4 | 30.8 |
| Mild | 5 | 38.5 |
| Moderate | 3 | 23.1 |
| Severe | 1 | 7.7 |
| 30-day mortality | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarzia, V.; Ponzoni, M.; Evangelista, G.; Tessari, C.; Bertaglia, E.; De Lazzari, M.; Zanella, F.; Pittarello, D.; Migliore, F.; Gerosa, G. Vacuum-Implemented Removal of Lead Vegetations in Cardiac Device-Related Infective Endocarditis. J. Clin. Med. 2022, 11, 4600. https://doi.org/10.3390/jcm11154600
Tarzia V, Ponzoni M, Evangelista G, Tessari C, Bertaglia E, De Lazzari M, Zanella F, Pittarello D, Migliore F, Gerosa G. Vacuum-Implemented Removal of Lead Vegetations in Cardiac Device-Related Infective Endocarditis. Journal of Clinical Medicine. 2022; 11(15):4600. https://doi.org/10.3390/jcm11154600
Chicago/Turabian StyleTarzia, Vincenzo, Matteo Ponzoni, Giuseppe Evangelista, Chiara Tessari, Emanuele Bertaglia, Manuel De Lazzari, Fabio Zanella, Demetrio Pittarello, Federico Migliore, and Gino Gerosa. 2022. "Vacuum-Implemented Removal of Lead Vegetations in Cardiac Device-Related Infective Endocarditis" Journal of Clinical Medicine 11, no. 15: 4600. https://doi.org/10.3390/jcm11154600