
Signs and Symptoms of Acute Bowel Inflammation and the Risk of Progression to Inflammatory Bowel Disease: A Retrospective Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Design
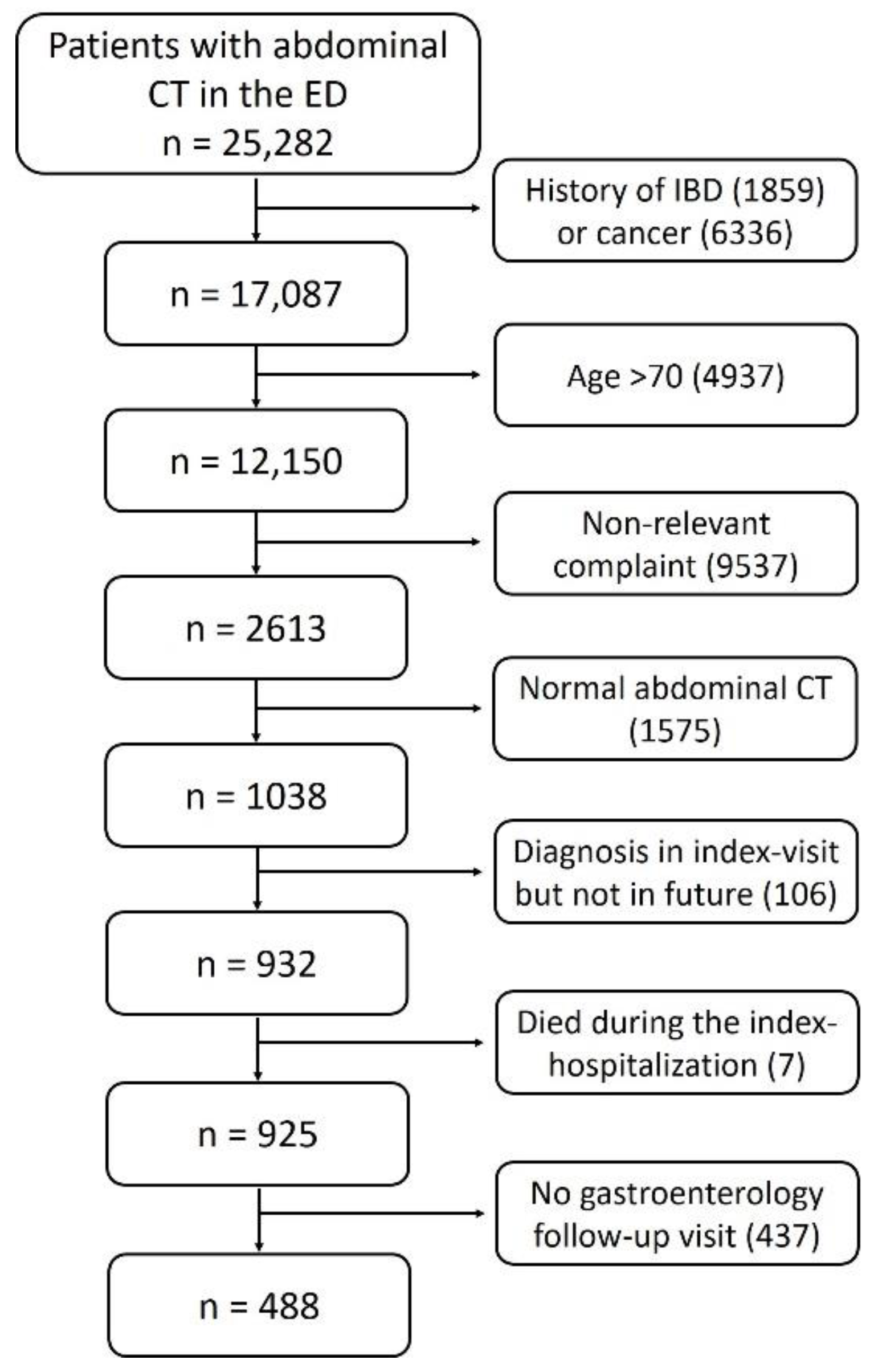
2.2. Exclusion Criteria
- Patients over 70 years old, as new onset IBD at that age group is rare;
- Patients not presenting with abdominal symptoms described above;
- Previous diagnosis of IBD or cancer;
- Abdominal CT scan with no abnormal findings;
- Patients with a presumptive diagnosis of IBD in the index hospitalization but without any further confirmation of an IBD diagnosis during follow up;
- Patients without any follow-up visit in the gastroenterology department in Sheba medical center after the index hospitalization;
- Patients who died during the index hospitalization.
2.3. Data Collection
2.4. Future Development of IBD
2.5. Statistycal Analysis
2.6. Study Ethics and Patient Consent
3. Results
3.1. Study Cohort
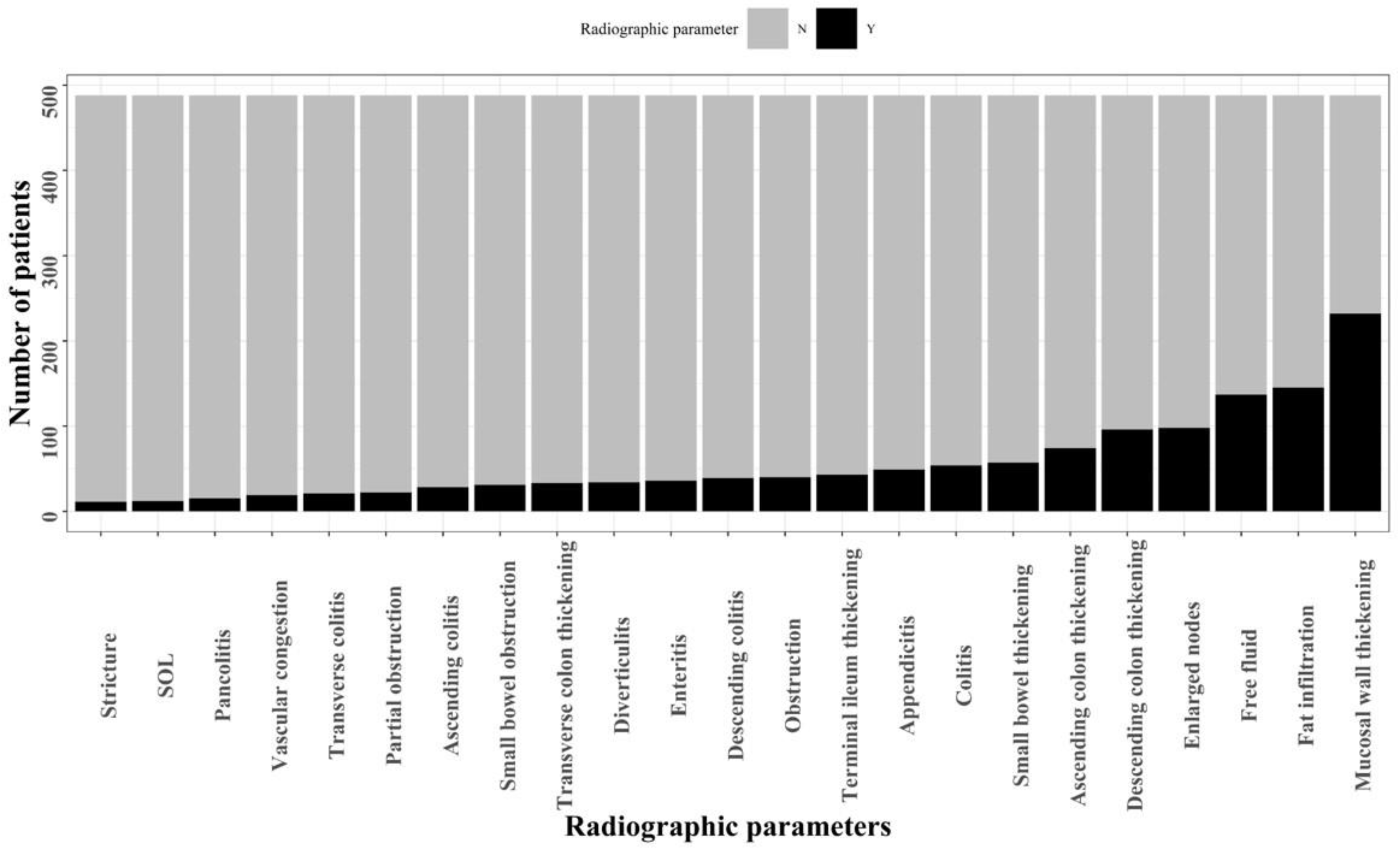
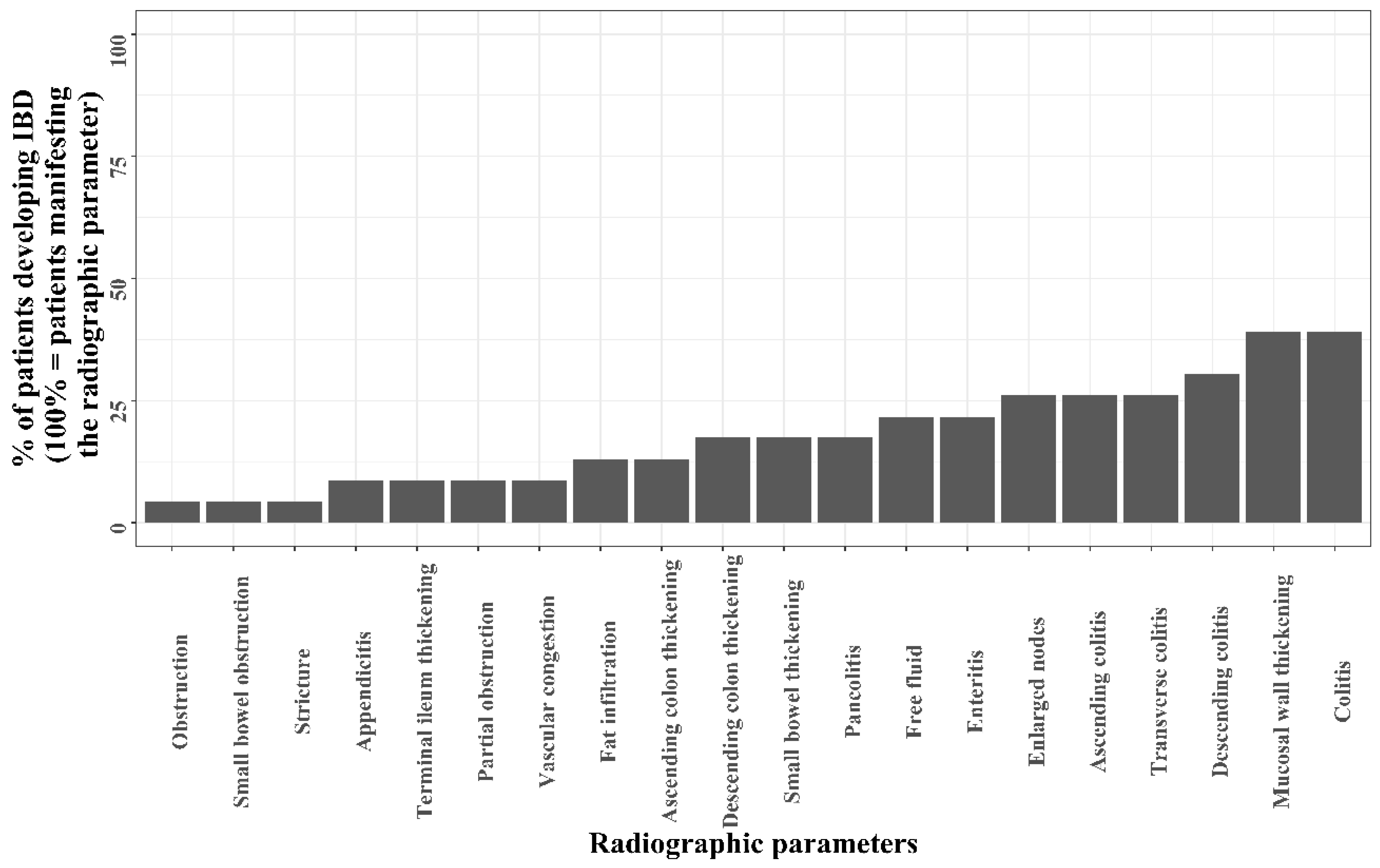
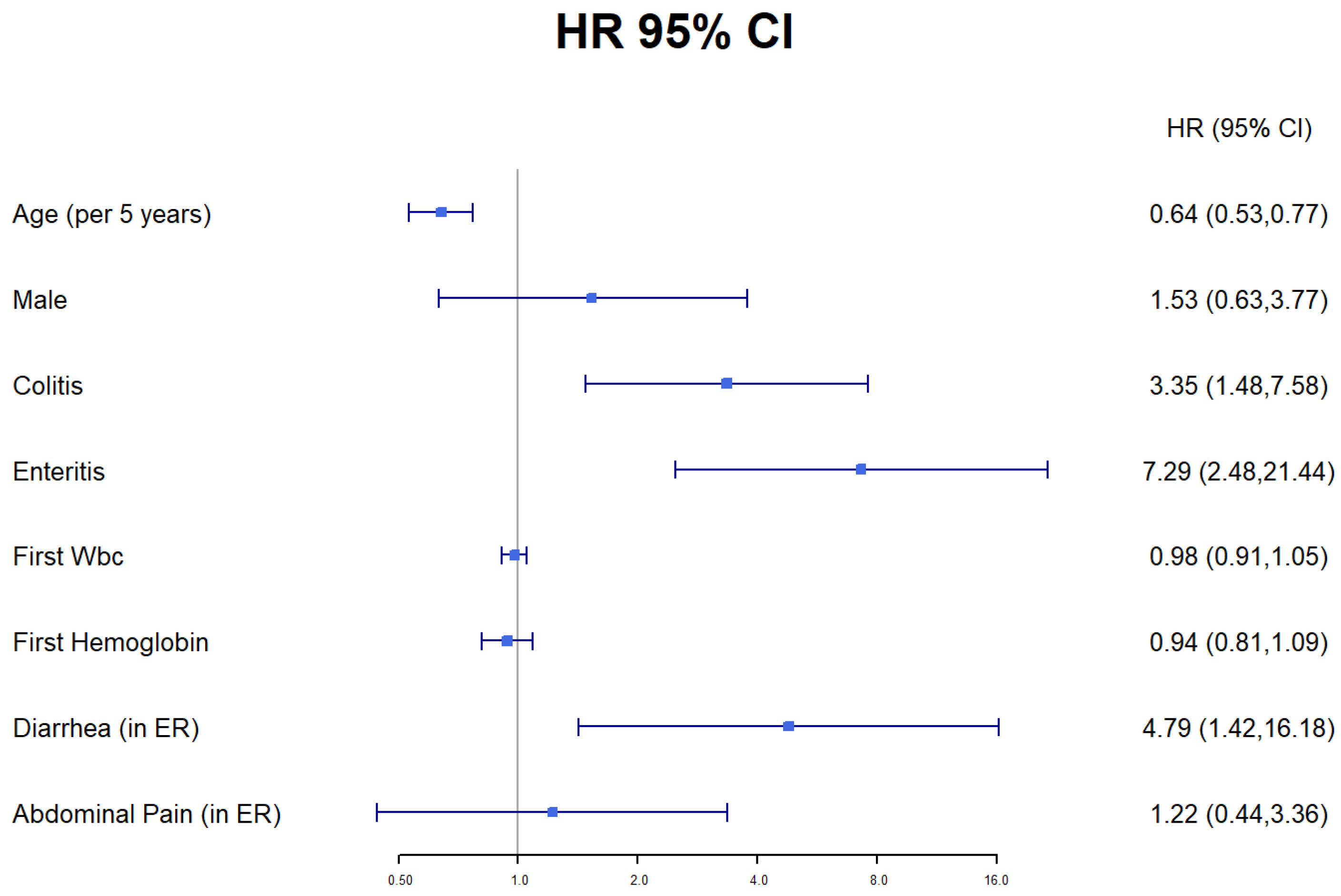
3.2. From Acute Intestinal Inflammation Progression to IBD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Perler, B.K.; Ungaro, R.; Baird, G.; Mallette, M.; Bright, R.; Shah, S.; Shapiro, J.; Sand, B.E. Presenting symptoms in inflammatory bowel disease: Descriptive analysis of a community-based inception cohort. BMC Gastroenterol. 2019, 19, 47. [Google Scholar] [CrossRef] [Green Version]
- Mekhjian, H.S.; Switz, D.M.; Melnyk, C.S.; Rankin, G.B.; Brooks, R.K. Clinical features and natural history of Crohn’s disease. Gastroenterology 1979, 77, 898–906. [Google Scholar] [CrossRef]
- Cantoro, L.; Di Sabatino, A.; Papi, C.; Margagnoni, G.; Ardizzone, S.; Giuffrida, P.; Giannarelli, D.; Massari, A.; Monterubbianesi, R.; Lenti, M.V.; et al. The time course of diagnostic delay in inflammatory bowel disease over the last sixty years: An Italian multicentre study. J. Crohn’s Colitis 2017, 11, 975–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahon, S.; Lahmek, P.; Lesgourgues, B.; Poupardin, C.; Chaussade, S.; Peyrin-Biroulet, L.; Abitbol, V. Diagnostic delay in a French cohort of Crohn’s disease patients. J. Crohn’s Colitis 2014, 8, 964–969. [Google Scholar] [CrossRef] [Green Version]
- Pellino, G.; Sciaudone, G.; Selvaggi, F.; Riegler, G. Delayed diagnosis is influenced by the clinical pattern of Crohn’s disease and affects treatment outcomes and quality of life in the long term: A cross-sectional study of 361 patients in Southern Italy. Eur. J. Gastroenterol. Hepatol. 2015, 27, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Greaves, M.L.; Pochapin, M. Asymptomatic Ileitis: Past, Present, and Future. J. Clin. Gastroenterol. 2006, 40, 281–285. [Google Scholar] [CrossRef]
- Dilauro, S.; Crum-Cianflone, N.F. Ileitis: When it is not Crohn’s disease. Curr. Gastroenterol. Rep. 2010, 12, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Lengeling, R.W.; Mitros, F.A.; Brennan, J.A.; Schulze, K.S. Ulcerative Ileitis Encountered at Ileo-Colonoscopy: Likely Role. Clin. Gastroenterol. Hepatol. 2003, 1, 160–169. [Google Scholar] [CrossRef]
- O’Donnell, S.; Crotty, P.L.; O’Sullivan, M.; Breslin, N.; O’Connor, H.J.; O’Morain, C.A.; Ryan, B.M. Isolated active ileitis: Is it a mild subtype of Crohn’s disease? Inflamm. Bowel Dis. 2013, 19, 1815–1822. [Google Scholar] [CrossRef]
- Tse, C.S.; Deepak, P.; Smyrk, T.C.; Raffals, L.E. Isolated Acute Terminal Ileitis without Preexisting Inflammatory Bowel Disease Rarely Progresses to Crohn’s Disease. Dig. Dis. Sci. 2017, 62, 3557–3562. [Google Scholar] [CrossRef]
- Goldstein, N.S. Isolated ileal erosions in patients with mildly altered bowel habits: A follow-up study of 28 patients. Am. J. Clin. Pathol. 2006, 125, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Fangbin, Z.; Weiwei, H.; Wugan, Z.; Cong, Z.; Yanjun, C.; Feng, X. The analysis of factors associated with progression of isolated terminal ileal lesions. PLoS ONE 2014, 9, e90797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courville, E.L.; Siegel, C.A.; Vay, T.; Wilcox, A.R.; Suriawinata, A.A.; Srivastava, A. Isolated asymptomatic ileitis does not progress to overt crohn disease on long-term follow-up despite features of chronicity in ileal biopsies. Am. J. Surg. Pathol. 2009, 33, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Delabrousse, E.; Ferreira, F.; Badet, N.; Martin, M.; Zins, M. Coping with the problems of diagnosis of acute colitis. Diagn. Interv. Imaging 2013, 94, 793–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zalis, M.; Singh, A.K. Imaging of inflammatory bowel disease: CT and MR. Dig Dis. 2004, 22, 56–62. [Google Scholar] [CrossRef]
- Gore, R.M.; Balthazar, E.J.; Ghahremani, G.G.; Miller, F.H. Disease Features of Ulcerative colitis and Crohn’s disease. Am. J. Roentgenol. 1996, 167, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. Laboratory markers in IBD: Useful, magic, or unnecessary toys? Gut 2006, 55, 426–431. [Google Scholar] [CrossRef] [Green Version]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. C-reactive protein as a marker for inflammatory bowel disease. Inflamm. Bowel Dis. 2004, 10, 661–665. [Google Scholar] [CrossRef] [Green Version]
- SShine, B.; Berghouse, L.; Jones, J.; Landon, J. C-Reactive protein as an aid in the differentiation of functional and inflammatory bowel disorders. Clin. Chim. Acta 1985, 148, 105–109. [Google Scholar] [CrossRef]
- Lewis, J.D. The utility of biomarkers in the diagnosis and therapy of inflammatory bowel disease. Gastroenterology 2011, 140, 1817–1826.e2. [Google Scholar] [CrossRef] [Green Version]
- Siddiki, H.; Dora, L.H.; Shabana, F.; Pasha, M.; Gurudu, S.R.; Leighton, J.A. Terminal Ileitis of Unknown Significance: Long-Term Follow-up and Outcomes in a Single Cohort of Patients: 1809. Am. J. Gastroenterol. 2015, 110, 1809–1810. [Google Scholar] [CrossRef]
- Schumacher, G.; Sandstedt, B.; Kollberg, B. A prospective study of first attacks of inflammatory bowel disease and infectious colitis: Clinical findings and early diagnosis. Scand. J. Gastroenterol. 1994, 29, 265–274. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-IBD (n = 465) | Future IBD (n = 23) | p-Value | |
|---|---|---|---|
| Male gender, n (%) | 243 (52.3) | 12 (52.2) | 1 |
| Age (median, IQR) | 56 (43, 63) | 28 (20.5, 43) | <0.001 |
| BMI (median, IQR) | 26.12 (22.76, 29.97) | 21.23 (19.65, 22.32( | <0.001 |
| Comorbidities, n (%) | |||
| Hypertension, n (%) | 67 (14.4) | 0 (0) | 0.1 |
| Diabetes mellitus, n (%) | 43 (9.2) | 0 (0) | 0.25 |
| Anemia, n (%) | 48 (10.3) | 1 (4.3) | 0.56 |
| Past smoker, n (%) | 29 (6.2) | 0 (0) | 0.43 |
| Laboratory features (IQR) | |||
| WBC | 10.88 (7.96, 14.23) | 9.78 (8.21, 13.44) | 0.595 |
| CRP | 34.38 (7.45, 104.28( | 67.42 (49.16, 145.8) | 0.07 |
| Albumin | 3.6 (3.3, 4 ( | 3.4 (3.1,3.7) | 0.210 |
| Hemoglobin | 13.01 (11.49, 14.28( | 12.49 (11.27, 13.32) | 0.364 |
| ED admission, n (%) | |||
| Fever (median, IQR) | 36.8 (36.6, 37.2( | 36.9 (36.75, 37.3) | 0.214 |
| Diarrhea diagnosis | 19 (4.1) | 4 (17.4) | 0.015 |
| Abdominal pain diagnosis | 104 (22.4) | 9 (30.4) | 0.52 |
| ED discharge | 103 (22.2) | 1 (4.3) | 0.076 |
| Hospitalization, n = 384 (%) | |||
| Re-hospitalizations—30 days | 79 (17) | 7 (30.4) | 0.172 |
| Re-hospitalizations—90 days | 118 (25.4) | 8 (34.8) | 0.45 |
| Surgery during index hospitalization | 83 (22.9) | 2 (9.1) | 0.21 |
| Imaging features, n (%) | |||
| Ascending colitis | 22 (4.7) | 6 (26.1) | <0.001 |
| Transverse colitis | 15 (3.2) | 6 (26.1) | <0.001 |
| Descending colitis | 32 (6.9) | 7 (30.4) | <0.001 |
| Pan-colitis | 11 (2.4) | 4 (17.4) | 0.001 |
| Enteritis | 31 (6.7) | 5 (21.7) | 0.022 |
| Number of Patients | 23 |
|---|---|
| Male, n (%) | 11 (47.8) |
| Crohn’s disease, n (%) Ulcerative colitis, n (%) | 19 (82.6) 4 (17.4) |
| Current or past smoker, n (% | 3 (13) |
| EIM, n (%) | 6 (26) |
CD extent at diagnosis, n (% of CD patients)
| 12 (63.1) 1 (5.3) 6 (31.6) |
CD behavior at diagnosis, n (% of CD patients)
| 12 (63.1) 4 (21.1) 3 (15.8) |
UC extent, n (%)
| 1 (25) 2 (50) 1 (25) |
Therapy on diagnosis, n (%)
| 9 (39.1) 2 (8.7) 5 (21.7) 3 (13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levartovsky, A.; Ovdat, T.; Barash, Y.; Ben-Shatach, Z.; Skinezes, Y.; Jesin, S.; Klempfner, R.; Grossman, E.; Kopylov, U.; Ben-Horin, S.; et al. Signs and Symptoms of Acute Bowel Inflammation and the Risk of Progression to Inflammatory Bowel Disease: A Retrospective Analysis. J. Clin. Med. 2022, 11, 4595. https://doi.org/10.3390/jcm11154595
Levartovsky A, Ovdat T, Barash Y, Ben-Shatach Z, Skinezes Y, Jesin S, Klempfner R, Grossman E, Kopylov U, Ben-Horin S, et al. Signs and Symptoms of Acute Bowel Inflammation and the Risk of Progression to Inflammatory Bowel Disease: A Retrospective Analysis. Journal of Clinical Medicine. 2022; 11(15):4595. https://doi.org/10.3390/jcm11154595
Chicago/Turabian StyleLevartovsky, Asaf, Tal Ovdat, Yiftach Barash, Zohar Ben-Shatach, Yael Skinezes, Stuart Jesin, Robert Klempfner, Ehud Grossman, Uri Kopylov, Shomron Ben-Horin, and et al. 2022. "Signs and Symptoms of Acute Bowel Inflammation and the Risk of Progression to Inflammatory Bowel Disease: A Retrospective Analysis" Journal of Clinical Medicine 11, no. 15: 4595. https://doi.org/10.3390/jcm11154595