
The JAK/STAT Pathway and Its Selective Inhibition in the Treatment of Atopic Dermatitis: A Systematic Review
 ,
,
Abstract
:
1. Introduction
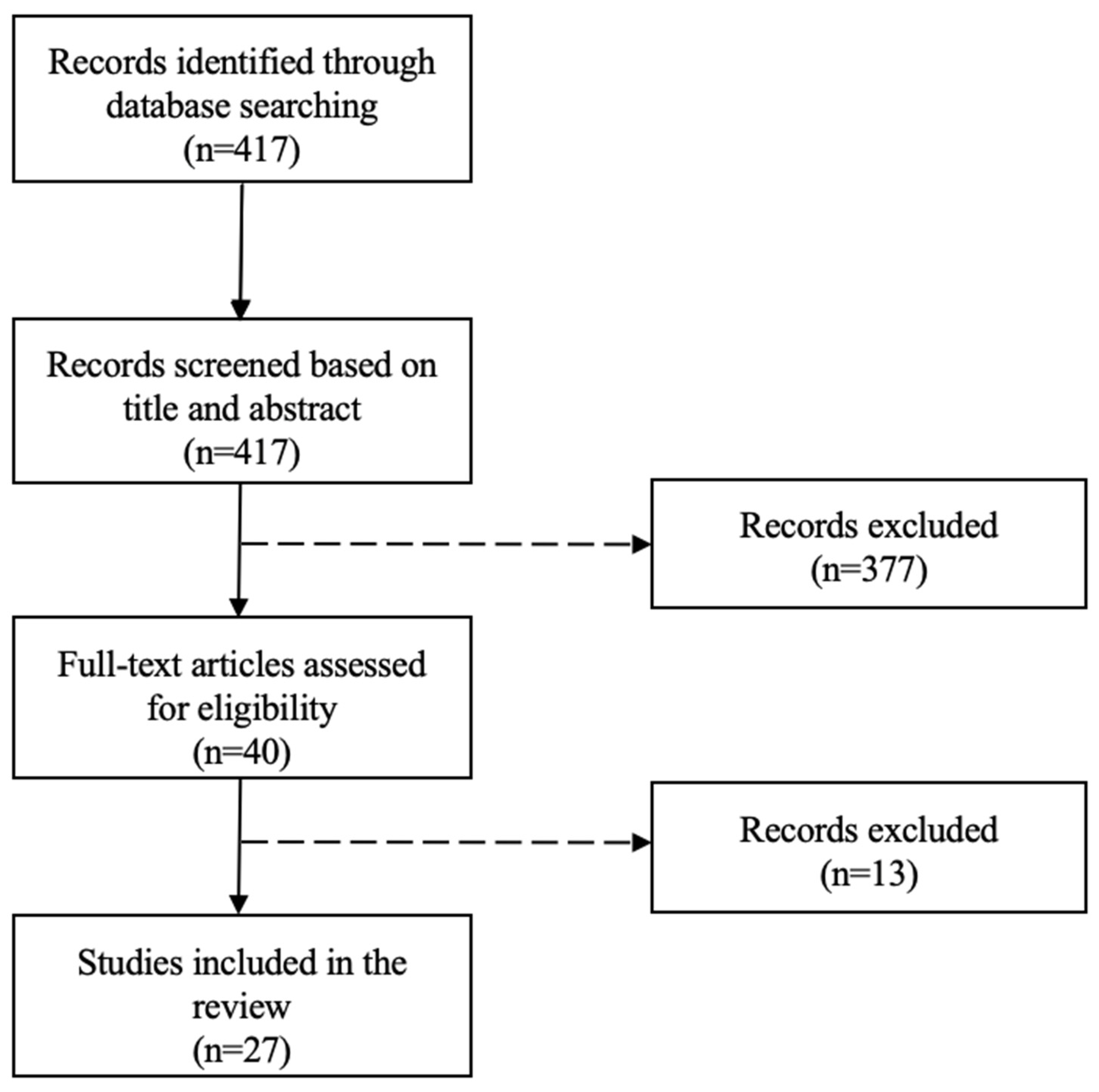
2. Materials and Methods
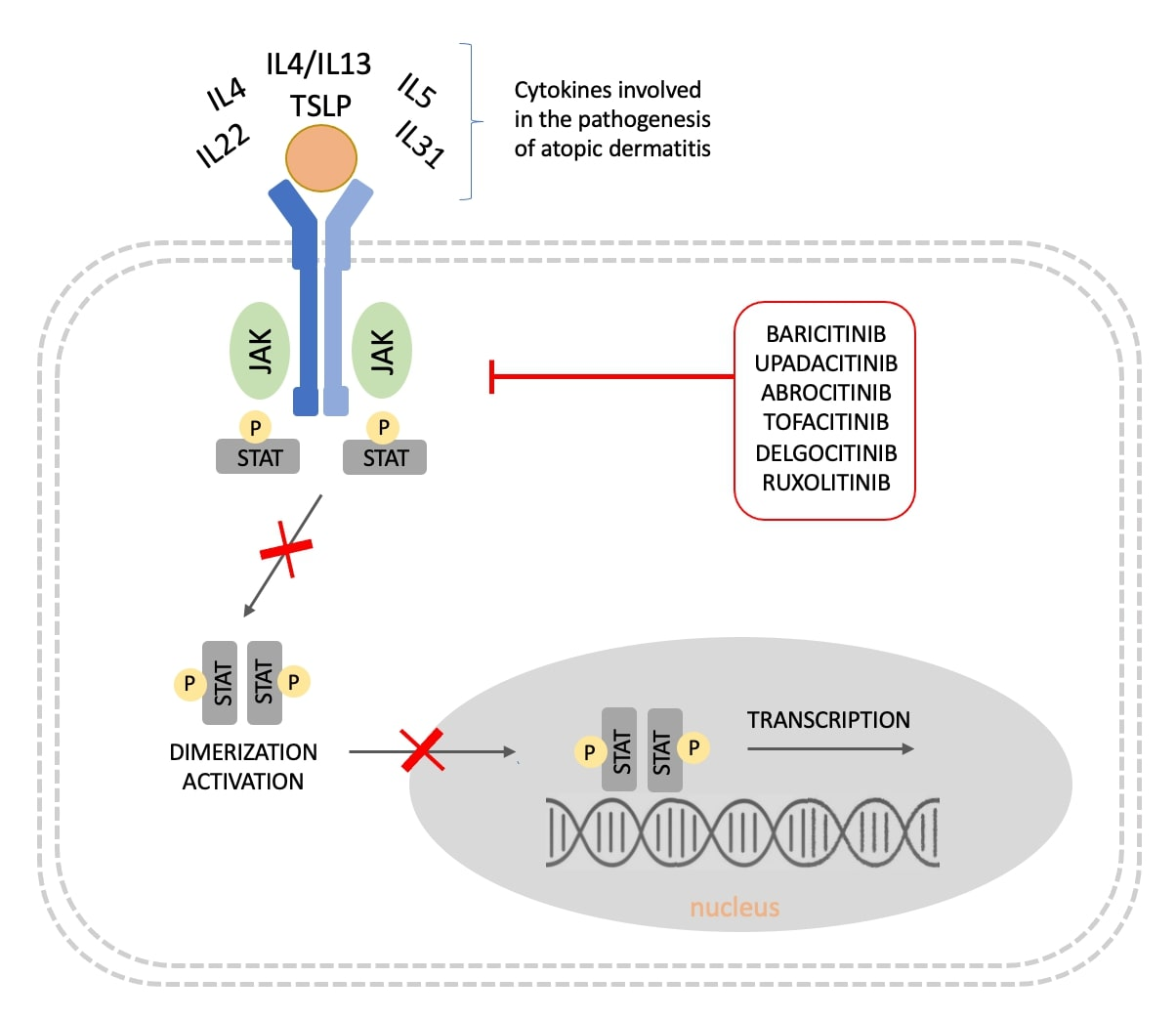
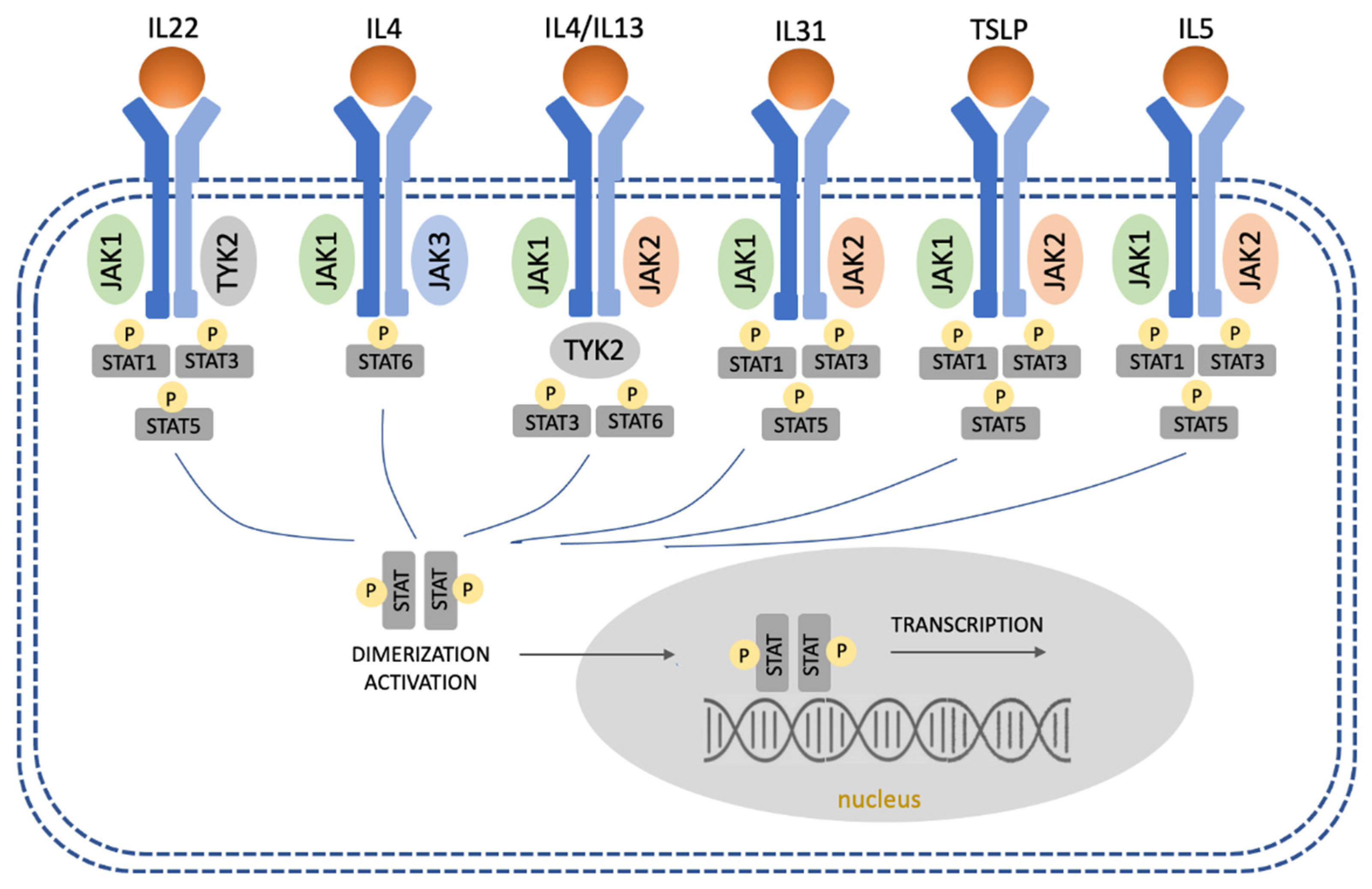
3. The JAK/STAT Pathway in AD
3.1. Overregulation of Th2 and Th22 Immune Responses
3.2. Regulation of Th1 and Th17 Immune Responses
3.3. Suppression of Regulatory T Cells
3.4. Stimulation of Eosinophils and Mast Cells
4. JAK Inhibitors for the Treatment of AD
5. Topical JAK Inhibitors
6. Systemic JAK Inhibitors
6.1. Baricitinib
6.2. Upadacitinib
6.3. Abrocitinib
6.4. Other Oral JAKs
7. Comparative Data Regarding the Efficacy and Safety of JAK Inhibitors in AD
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AD | atopic dermatitis |
| BSA | body surface area |
| CPK | creatine phosphokinase |
| EASI | eczema area and severity index |
| IFN-γ | interferon-γ |
| Ig | Immunoglobulin |
| IGA | Investigator’s Global Assessment |
| IL | Interleukin |
| JAK | Janus kinase |
| RCT | randomized controlled trial |
| STAT | signal transducer and activation of transcription |
| TCS | topical corticosteroids |
| Th | T helper |
| TNF-a | tumor necrosis factor alpha |
| Treg | T regulatory |
| TSLP | thymic stromal lymphopoietin |
| TYK2 | tyrosine kinase 2 |
References
- Li, H.; Zhang, Z.; Zhang, H.; Guo, Y.; Yao, Z. Update on the Pathogenesis and Therapy of Atopic Dermatitis. Clin. Rev. Allergy Immunol. 2021, 61, 324–338. [Google Scholar] [CrossRef] [PubMed]
- Mandlik, D.S.; Mandlik, S.K. Atopic dermatitis: New insight into the etiology, pathogenesis, diagnosis and novel treatment strategies. Immunopharmacol. Immunotoxicol. 2021, 43, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Howell, M.D.; Kuo, F.I.; Smith, P.A. Targeting the Janus Kinase Family in Autoimmune Skin Diseases. Front. Immunol. 2019, 10, 2342. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, C.S.; Amici, M.; Bortolotto, Z.A.; Doherty, A.; Csaba, Z.; Fafouri, A.; Dournaud, P.; Gressens, P.; Collingridge, G.L.; Peineau, S. The role of JAK-STAT signaling within the CNS. JAKSTAT 2013, 2, e22925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlings, J.S.; Rosler, K.M.; Harrison, D.A. The JAK/STAT signaling pathway. J. Cell Sci. 2004, 117, 1281–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubin, C.; Del Duca, E.; Guttman-Yassky, E. The IL-4, IL-13 and IL-31 pathways in atopic dermatitis. Expert Rev. Clin. Immunol. 2021, 17, 835–852. [Google Scholar] [CrossRef]
- Singh, R.; Heron, C.E.; Ghamrawi, R.I.; Strowd, L.C.; Feldman, S.R. Emerging Role of Janus Kinase Inhibitors for the Treatment of Atopic Dermatitis. ImmunoTargets Ther. 2020, 9, 255–272. [Google Scholar] [CrossRef]
- Gündüz, Ö. JAK/STAT pathway modulation: Does it work in dermatology? Dermatol. Ther. 2019, 32, e12903. [Google Scholar] [CrossRef]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Oda, M.; Kabashima, K.; Nagata, T. Phase 2 clinical study of delgocitinib ointment in pediatric patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 144, 1575–1583. [Google Scholar] [CrossRef]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Nagata, T. Efficacy and safety of topical JTE-052, a Janus kinase inhibitor, in Japanese adult patients with moderate-to-severe atopic dermatitis: A phase II, multicentre, randomized, vehicle-controlled clinical study. Br. J. Dermatol. 2018, 178, 424–432. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Kaino, H.; Nagata, T. Delgocitinib ointment, a topical Janus kinase inhibitor, in adult patients with moderate to severe atopic dermatitis: A phase 3, randomized, double-blind, vehicle-controlled study and an open-label, long-term extension study. J. Am. Acad. Dermatol. 2020, 82, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Kabashima, K.; Oda, M.; Nagata, T. Delgocitinib ointment in pediatric patients with atopic dermatitis: A phase 3, randomized, double-blind, vehicle-controlled study and a subsequent open-label, long-term study. J. Am. Acad. Dermatol. 2021, 85, 854–862. [Google Scholar] [CrossRef]
- Bissonnette, R.; Papp, K.A.; Poulin, Y.; Gooderham, M.; Raman, M.; Mallbris, L.; Wang, C.; Purohit, V.; Mamolo, C.; Papacharalambous, J.; et al. Topical tofacitinib for atopic dermatitis: A phase IIa randomized trial. Br. J. Dermatol. 2016, 175, 902–911. [Google Scholar] [CrossRef]
- Papp, K.; Szepietowski, J.C.; Kircik, L.; Toth, D.; Eichenfield, L.F.; Leung, D.Y.M.; Forman, S.B.; Venturanza, M.E.; Sun, K.; Kuligowski, M.E.; et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: Results from 2 phase 3, randomized, double-blind studies. J. Am. Acad. Dermatol. 2021, 85, 863–872. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Silverberg, J.I.; Nemoto, O.; Forman, S.B.; Wilke, A.; Prescilla, R.; de la Pena, A.; Nunes, F.P.; Janes, J.; Gamalo, M.; et al. Baricitinib in adult patients with moderate-to-severe atopic dermatitis: A phase 2 parallel, double-blinded, randomized placebo-controlled multiple-dose study. J. Am. Acad. Dermatol. 2019, 80, 913–921.e9. [Google Scholar] [CrossRef]
- Simpson, E.L.; Lacour, J.P.; Spelman, L.; Galimberti, R.; Eichenfield, L.F.; Bissonnette, R.; King, B.A.; Thyssen, J.P.; Silverberg, J.I.; Bieber, T.; et al. Baricitinib in patients with moderate-to-severe atopic dermatitis and inadequate response to topical corticosteroids: Results from two randomized monotherapy phase III trials. Br. J. Dermatol. 2020, 183, 242–255. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Simpson, E.L.; Wollenberg, A.; Bissonnette, R.; Kabashima, K.; DeLozier, A.M.; Sun, L.; Cardillo, T.; Nunes, F.P.; Reich, K. Long-term Efficacy of Baricitinib in Adults With Moderate to Severe Atopic Dermatitis Who Were Treatment Responders or Partial Responders: An Extension Study of 2 Randomized Clinical Trials. JAMA Dermatol. 2021, 157, 691–699. [Google Scholar] [CrossRef]
- Bieber, T.; Reich, K.; Paul, C.; Tsunemi, Y.; Augustin, M.; Lacour, J.; Ghislain, P.D.; Dutronc, Y.; Liao, R.; Yang, F.E.; et al. Efficacy and Safety of Baricitinib in Combination With Topical Corticosteroids in Patients With Moderate-to-Severe Atopic Dermatitis With Inadequate Response, Intolerance, or Contraindication to Cyclosporine: Results From a Randomized, Placebo-Controlled, Phase III Clinical Trial (BREEZE-AD4). Br. J. Dermatol. 2022. [Google Scholar] [CrossRef]
- Simpson, E.L.; Forman, S.; Silverberg, J.I.; Zirwas, M.; Maverakis, E.; Han, G.; Guttman-Yassky, E.; Marnell, M.; Bissonette, R.; Waibel, J.; et al. Baricitinib in patients with moderate-to-severe atopic dermatitis: Results from a randomized monotherapy phase 3 trial in the United States and Canada (BREEZE-AD5). J. Am. Acad. Dermatol. 2021, 85, 62–70. [Google Scholar] [CrossRef]
- Reich, K.; Kabashima, K.; Peris, K.; Silverberg, J.I.; Eichenfield, L.F.; Bieber, T.; Kaszuba, A.; Kolodsick, J.; Yang, F.E.; Gamalo, M.; et al. Efficacy and safety of baricitinib combined with topical corticosteroids for treatment of moderate to severe atopic dermatitis: A randomized clinical trial. JAMA Dermatol. 2020, 156, 1333–1343. [Google Scholar] [CrossRef]
- Guttman-yassky, E.; Thaçi, D.; Pangan, A.L.; Papp, K.A.; Reich, K.; Beck, L.A.; Mohamed, M.E.F.; Othman, A.A.; Anderson, J.K.; Gu, Y.; et al. Upadacitinib in Adults With Moderate-to-Severe Atopic Dermatitis: 16-Week Results From a Randomized, Placebo-Controlled Trial. J. Allergy Clin. Immunol. 2020, 145, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Guttman-Yassky, E.; Teixeira, H.D.; Simpson, E.L.; Papp, K.A.; Pangan, A.L.; Blauvelt, A.; Thaci, D.; Chu, C.Y.; Hong, H.C.H.; Katoh, N.; et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): Results from two replicate double-blind, randomised controlled phase 3 trials. Lancet 2021, 397, 2151–2168. [Google Scholar] [CrossRef]
- Simpson, E.L.; Papp, K.A.; Blauvelt, A.; Chu, C.-Y.; Hong, H.C.-H.; Katoh, N.; Calimlim, B.M.; Thyssen, J.P.; Chiou, A.S.; Bissonnette, R.; et al. Efficacy and Safety of Upadacitinib in Patients With Moderate to Severe Atopic Dermatitis: Analysis of Follow-up Data From the Measure Up 1 and Measure Up 2 Randomized Clinical Trials. JAMA Dermatol. 2022, 158, 404–413. [Google Scholar] [CrossRef]
- Reich, K.; Teixeira, H.D.; de Bruin-Weller, M.; Bieber, T.; Soong, W.; Kabashima, K.; Werfel, T.; Zeng, J.; Huang, X.; Hu, X.; et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): Results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2021, 397, 2169–2181. [Google Scholar] [CrossRef]
- Silverberg, J.I.; de Bieber, W.; Soong, W.; Kabashima, K.; Costanzo, A.; Rosmarin, D.; Lynde, C.; Liu, J.; Gamelli, A.; Zeng, J.; et al. Upadacitinib plus topical corticosteroids in atopic dermatitis: Week-52 AD Up study results. J. Allergy Clin. Immunol. 2021, 149, 977–987.e14. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; Teixeira, H.D.; Simpson, E.L.; Costanzo, A.; De Bruin-Weller, M.; Barbarot, S.; Proajapati, V.H.; Lio, P.; Hu, X.; Wu, T.; et al. Efficacy and Safety of Upadacitinib vs Dupilumab in Adults With Moderate-to-Severe Atopic Dermatitis A Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Katoh, N.; Ohya, Y.; Murota, H.; Ikeda, M.; Hu, X.; Ikeda, K.; Liu, J.; Sasaki, T.; Chu, A.D.; Teixeira, A.D.; et al. A phase 3 randomized, multicenter, double-blind study to evaluate the safety of upadacitinib in combination with topical corticosteroids in adolescent and adult patients with moderate-to-severe atopic dermatitis in Japan (Rising Up): An interim 24-week analysis. JAAD Int. 2022, 6, 27–36. [Google Scholar]
- Gooderham, M.J.; Forman, S.B.; Bissonnette, R.; Beebe, J.S.; Zhang, W.; Banfield, C.; Zhu, L.; Papacharalambous, J.; Vincent, M.S.; Peeva, E.; et al. Efficacy and Safety of Oral Janus Kinase 1 Inhibitor Abrocitinib for Patients with Atopic Dermatitis: A Phase 2 Randomized Clinical Trial. JAMA Dermatol. 2019, 155, 1371–1379. [Google Scholar] [CrossRef] [Green Version]
- Simpson, E.L.; Sinclair, R.; Forman, S.; Wollenberg, A.; Aschoff, R.; Cork, M.; Bieber, T.; Thyssen, J.P.; Yosipovich, G.; Flohr, C.; et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): A multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet 2020, 396, 255–266. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Simpson, E.L.; Thyssen, J.P.; Gooderham, M.; Chan, G.; Feeney, C.; Biswas, P.; Valdez, H.; DiBonaventura, M.; Nduaka, C.; et al. Efficacy and Safety of Abrocitinib in Patients with Moderate-to-Severe Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol. 2020, 156, 863–873. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Flohr, C.; Sidbury, R.; Siegfried, E.; Szalai, Z.; Galus, R.; Yao, Z.; Takahashi, H.; Barbarot, S.; Feeney, C.; et al. Efficacy and Safety of Abrocitinib in Combination with Topical Therapy in Adolescents with Moderate-to-Severe Atopic Dermatitis: The JADE TEEN Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 1165–1173. [Google Scholar] [CrossRef]
- Blauvelt, A.; Silverberg, J.I.; Lynde, C.W.; Bieber, T.; Eisman, S.; Zdybski, J.; Gubelin, W.; Simpson, E.L.; Valenzuela, F.; Criado, P.R.; et al. Abrocitinib induction, randomized withdrawal, and retreatment in patients with moderate-to-severe atopic dermatitis: Results from the JAK1 Atopic Dermatitis Efficacy and Safety (JADE) REGIMEN phase 3 trial. J. Am. Acad. Dermatol. 2022, 86, 104–112. [Google Scholar] [CrossRef]
- Bieber, T.; Simpson, E.L.; Silverberg, J.I.; Thaçi, D.; Paul, C.; Pink, A.E.; Kataoka, Y.; Chu, C.Y.; DiBonaventura, M.; Roji, R.; et al. Abrocitinib versus Placebo or Dupilumab for Atopic Dermatitis. N. Engl. J. Med. 2021, 384, 1101–1112. [Google Scholar] [CrossRef]
- Shi, V.Y.; Bhutani, T.; Fonacier, L.; Deleuran, M.; Shumack, S.; Valdez, H.; Zhang, F.; Chan, G.L.; Cameron, M.C.; Yin, N.C. Phase 3 efficacy and safety of abrocitinib in adults with moderate-to-severe atopic dermatitis after switching from dupilumab (JADE EXTEND). J. Am. Acad. Dermatol. 2022, 87, 351–358. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, L.; Ding, Y.; Tao, X.; Ji, C.; Dong, X.; Lu, J.; Wu, L.; Wang, R.; Lu, Q.; et al. Efficacy and Safety of SHR0302, a Highly Selective Janus Kinase 1 Inhibitor in Patients with Moderate to Severe Atopic Dermatitis: A Phase II Randomized Clinical Trial. Am. J. Clin. Dermatol. 2021, 22, 877–889. [Google Scholar] [CrossRef]
- Mowen, K.A.; Glimcher, L.H. Signaling pathways in Th2 development. Immunol. Rev. 2004, 202, 203–222. [Google Scholar] [CrossRef]
- Karpathiou, G.; Papoudou-Bai, A.; Ferrand, E.; Dumollard, J.M.; Peoc’h, M. STAT6: A review of a signaling pathway implicated in various diseases with a special emphasis in its usefulness in pathology. Pathol. Res. Pract. 2021, 223, 153477. [Google Scholar] [CrossRef]
- Tamura, K.; Arakawa, H.; Suzuki, M.; Kobayashi, Y.; Mochizuki, H.; Kato, M.; Tokuyama, K.; Morikawa, A. Novel dinucleotide repeat polymorphism in the first exon of the STAT-6 gene is associated with allergic diseases. Clin. Exp. Allergy 2001, 31, 1509–1514. [Google Scholar] [CrossRef]
- Gandhi, N.A.; Bennett, B.L.; Graham, N.M.H.; Pirozzi, G.; Stahl, N.; Yancopoulos, G.D. Targeting key proximal drivers of type 2 inflammation in disease. Nat. Rev. Drug Discov. 2016, 15, 35–50. [Google Scholar] [CrossRef]
- Salas, A.; Hernandez-Rocha, C.; Duijvestein, M.; Faubion, W.; McGovern, D.; Vermeire, S.; Vetrano, S.; Casteele, N.V. JAK–STAT pathway targeting for the treatment of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 323–337. [Google Scholar] [CrossRef]
- Molfino, N.A.; Gossage, D.; Kolbeck, R.; Parker, J.M.; Geba, G.P. Molecular and clinical rationale for therapeutic targeting of interleukin-5 and its receptor. Clin. Exp. Allergy 2012, 42, 712–737. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Zhang, H.; Chan, L.S. The involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitis. JAKSTAT 2013, 2, e24137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochman, Y.; Kashyap, M.; Robinson, G.W.; Sakamoto, K.; Gomez-Rodriguez, J.; Wagner, K.U.; Leonard, W.J. Thymic stromal lymphopoietin-mediated STAT5 phosphorylation via kinases JAK1 and JAK2 reveals a key difference from IL-7-induced signaling. Proc. Natl. Acad. Sci. USA 2010, 107, 19455–19460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howell, M.D.; Kim, B.E.; Gao, P.; Grant, A.V.; Boguniewicz, M.; Debenedetto, A.; Schneider, L.; Beck, L.A.; Barnes, K.C.; Leung, D.Y.M. Cytokine Modulation of AD Filaggrin Skin Expression. J. Allergy Clin. Immunol. 2007, 120, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.E.; Leung, D.Y.M.; Boguniewicza, M.; Howell, M.D. Loricrin and involucrin expression is down-regulated by Th2 cytokines through STAT-6. Clin. Immunol. 2008, 126, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Albanesi, C.; Fairchild, H.R.; Madonna, S.; Scarponi, C.; De Pita, O.; Leung, D.Y.M.; Howell, M.D. IL-4 and IL-13 Negatively Regulate TNF-α- and IFN-γ-induced β-Defensin Expression through STAT-6, Suppressor of Cytokine Signaling (SOCS)-1, and SOCS-3. J. Immunol. 2007, 179, 984–992. [Google Scholar] [CrossRef] [Green Version]
- Brauweiler, A.M.; Goleva, E.; Leung, D.Y.M. Th2 cytokines increase staphylococcus aureus alpha toxin-induced keratinocyte death through the signal transducer and activator of transcription 6 (STAT6). J. Investig. Dermatol. 2014, 134, 2114–2121. [Google Scholar] [CrossRef] [Green Version]
- Ong, P.Y.; Ohtake, T.; Brandt, C.; Strickland, I.; Boguniewicz, M.; Ganz, T.; Gallo, R.L.; Leung, D.Y.M. Endogenous Antimicrobial Peptides and Skin Infections in Atopic Dermatitis. N. Engl. J. Med. 2002, 347, 1151–1160. [Google Scholar] [CrossRef] [Green Version]
- Furue, M. Regulation of Skin Barrier Function via Competition between AHR Axis versus IL-13/IL-4-JAK-STAT6/STAT3 Axis: Pathogenic and Therapeutic Implications in Atopic Dermatitis. J. Clin. Med. 2020, 9, 3741. [Google Scholar] [CrossRef]
- Eyerich, K.; Dimartino, V.; Cavani, A. IL-17 and IL-22 in immunity: Driving protection and pathology. Eur. J. Immunol. 2017, 47, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Boniface, K.; Bernard, F.X.; Garcia, M.; Gurney, A.L.; Lecron, J.C.; Morel, F. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J. Immunol. 2005, 174, 3695–3702. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, C.; Yanagihara, S.; Otsuka, A. Innovation in the treatment of atopic dermatitis: Emerging topical and oral Janus kinase inhibitors. Allergol. Int. 2022, 71, 40–46. [Google Scholar] [CrossRef]
- Seif, F.; Khoshmirafa, M.; Aazami, H.; Mohsenzadegan, M.; Sedighi, G.; Bahar, M. The role of JAK-STAT signaling pathway and its regulators in the fate of T helper cells. Cell Commun. Signal. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Pernis, A.B.; Rothman, P.B. JAK-STAT signaling in asthma. J. Clin. Investig. 2002, 109, 1279–1283. [Google Scholar] [CrossRef]
- Koga, C.; Kabashima, K.; Shiraishi, N.; Kobayashi, M.; Tokura, Y. Possible pathogenic role of Th17 cells for atopic dermatitis. J. Investig. Dermatol. 2008, 128, 2625–2630. [Google Scholar] [CrossRef] [Green Version]
- Fyhrquist, N.; Lehtimaki, S.; Lahl, K.; Savinko, T.; Lappetelainen, A.M.; Sparwasser, T.; Wolff, H.; Lauerma, A.; Alenius, H. Foxp3+ cells control Th2 responses in a murine model of atopic dermatitis. J. Investig. Dermatol. 2012, 132, 1672–1680. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, J.D.; Burlion, A.; Zaragoza, B.; Sendeyo, K.; Polansky, J.K.; Huehn, J.; Piaggio, E.; Salomon, B.L.; Marodon, G. Inhibition of the JAK/STAT signaling pathway in regulatory T cells reveals a very dynamic regulation of Foxp3 expression. PLoS ONE 2016, 11, e0153682. [Google Scholar] [CrossRef]
- Chapoval, S.; Dasgupta, P.; Dorsey, N.J.; Keegan, A.D. Regulation of the T helper cell type 2 (Th2)/T regulatory cell (Treg) balance by IL-4 and STAT6. J. Leukoc. Biol. 2010, 87, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Cheung, P.F.Y.; Wong, C.K.; Ho, A.W.Y.; Hu, S.; Chen, D.P.; Lam, C.W.K. Activation of human eosinophils and epidermal keratinocytes by Th2 cytokine IL-31: Implication for the immunopathogenesis of atopic dermatitis. Int. Immunol. 2010, 22, 453–467. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, K.; Tanabe, E.; Ishihara, C.; Kagami, M.; Sugiyama, T.; Sueishi, M.; Koya, N.; Tomioka, H. Role of JAK2 signal transductional pathway in activation and survival of human peripheral eosinophils by interferon-gamma (IFN-γ). Clin. Exp. Immunol. 1999, 118, 340–343. [Google Scholar] [CrossRef]
- Sismanopoulos, N.; Delivanis, D.A.; Alysandratos, K.D.; Angelidou, A.; Vasiadi, M.; Therianou, A.; Theocharides, T.C. IL-9 induces VEGF secretion from human mast cells and IL-9/IL-9 receptor genes are overexpressed in atopic dermatitis. PLoS ONE 2012, 7, e33271. [Google Scholar] [CrossRef]
- García-Melendo, C.; Cubiró, X.; Puig, L. Janus Kinase Inhibitors in Dermatology: Part 2: Applications in Psoriasis, Atopic Dermatitis, and Other Dermatoses. Actas Dermosifiliogr. 2021, 112, 586–600. [Google Scholar] [CrossRef]
- Morales, J.K.; Falanga, Y.T.; Depcrynski, A.; Fernando, J.; Ryan, J.J. Mast cell homeostasis and the JAK–STAT pathway. Genes Immun. 2010, 11, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Traidl, S.; Freimooser, S.; Werfel, T. Janus kinase inhibitors for the therapy of atopic dermatitis. Allergol. Sel. 2021, 5, 293–304. [Google Scholar] [CrossRef]
- Japan Tobacco Inc. JT Receives Manufacturing And Marketing Approval of Corectim® Ointment 0.5% for the Treatment of Atopic Dermatitis in Japan. Available online: https://www.jt.com/media/news/2020/pdf/20200123_E01.pdf (accessed on 22 June 2022).
- Piscitelli, S.C.; Pavel, A.B.; McHale, K.; Jett, J.E.; Collins, J.; Gillmor, D.; Tabolt, F.; Li, R.; Song, T.; Zhang, L.; et al. A Phase 1b, Randomized, Single-Center Trial of Topical Cerdulatinib (DMVT-502) in Patients with Mild-to-Moderate Atopic Dermatitis. J. Investig. Dermatol. 2021, 141, 1847–1851. [Google Scholar] [CrossRef]
- Landis, M. A Phase 2b study to evaluate the efficacy and safety of the topical TYK2/JAK1 inhibitor brepocitinib for mild-to-moderate atopic dermatitis. Abstract (D1T03.4D). In Proceedings of the European Academy of Dermatology and Venereology Virtual Congress, 2020. Available online: https://conferences.medicom-publishers.com/wp-content/uploads/2021/07/E_MCR-EADV-2020.pdf (accessed on 10 June 2022).
- Smith, S.; Bhatia, N.; Shanler, S.D.; DeMoor, R.; Schnyder, J. Safety of ATI-502, a novel topical JAK1/3 inhibitor, in adults with moderate to severe atopic dermatitis: Results from a phase 2a open-label trial. J. Am. Acad. Dermatol. 2020, 83, AB170. [Google Scholar] [CrossRef]
- Evaluate the Efficacy and Safety of Topical SHR0302 Ointment in Patients with Mild-to-Moderate Atopic Dermatitis (MARBLE-23). Available online: https://clinicaltrials.gov/ct2/show/NCT04717310 (accessed on 22 June 2022).
- Markham, A. Baricitinib: First Global Approval. Drugs 2017, 77, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Bieber, T.; Thyssen, J.P.; Reich, K.; Simpson, E.L.; Katoh, N.; Torrelo, A.; De Bruin-Wellerer, M.; Thaci, T.; Bissonnette, R.; Gooderham, M.; et al. Pooled safety analysis of baricitinib in adult patients with atopic dermatitis from 8 randomized clinical trials. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.; Guttman-Yassky, E.; Torres, T. Selective JAK1 Inhibitors for the Treatment of Atopic Dermatitis: Focus on Upadacitinib and Abrocitinib. Am. J. Clin. Dermatol. 2020, 21, 783–798. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, L.; Jiang, X. The efficacy of Janus kinase inhibitors in patients with atopic dermatitis: A systematic review and network meta-analysis. Dermatol. Ther. 2021, 34, e15098. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Sun, X.; Zhao, K.; Meng, F.; Li, L.; Mu, Z.; Han, X. Efficacy and Safety of Janus Kinase Inhibitors for the Treatment of Atopic Dermatitis: A Systematic Review and Meta-Analysis. Dermatology 2021, 238, 1–11. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Hong, H.C.H.; Thyssen, J.P.; Calimlim, B.M.; Joshi, A.; Teixeira, H.D.; Collins, E.B.; Crowell, M.M.; Johnson, S.J.; Armstrong, A.W. Comparative Efficacy of Targeted Systemic Therapies for Moderate to Severe Atopic Dermatitis without Topical Corticosteroids: Systematic Review and Network Meta-analysis. Dermatol. Ther. 2022, 12, 1181–1196. [Google Scholar] [CrossRef]
- FDA Requires Warnings about Increased Risk of serious Heart-Related Events, Cancer, Blood Clots, and Death for JAK Inhibitors that treat Certain Chronic Inflammatory Conditions. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requires-warnings-about-increased-risk-serious-heart-related-events-cancer-blood-clots-and-death (accessed on 22 June 2022).
- Clark, J.D.; Flanagan, M.E.; Telliez, J.B. Discovery and development of Janus kinase (JAK) inhibitors for inflammatory diseases. J. Med. Chem. 2014, 57, 5023–5038. [Google Scholar] [CrossRef]
- Parmentier, J.M.; Voss, J.; Graff, C.; Schwartz, A.; Argiriadi, M.; Friedman, M.; Camp, H.S.; Padley, R.J.; George, J.S.; Hyland, D.; et al. In Vitro and In Vivo characterization of the JAK1 selectivity of upadacitinib (ABT-494). BMC Rheumatol. 2018, 2, 23. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Search Terms | Results |
|---|---|
| JAK inhibitor | 9898 |
| JAK/STAT pathway | 8894 |
| Tofacitinib | 2314 |
| Delgocitinib | 46 |
| Ruxolitinib | 2240 |
| Baricitinib | 885 |
| Upadacitinib | 340 |
| Abrocitinib | 88 |
| JAK inhibitor OR JAK/STAT pathway OR tofacitinib OR delgocitinib OR ruxolitinib OR baricitinib OR upadacitinib OR abrocitinib | 18,427 |
| Atopic dermatitis | 32,379 |
| Atopic dermatitis AND (JAK inhibitor OR JAK/STAT pathway OR tofacitinib OR delgocitinib OR ruxolitinib OR baricitinib OR upadacitinib OR abrocitinib) | 417 |
| Study Identifier | Phase | Study Group | Intervention | Primary Endpoint(s) |
|---|---|---|---|---|
| Delgocitinib (topical pan-JAK inhibitor) | ||||
| JapicCTI-173553 [9] | II | 2–15 | Delgocitinib (oint), vehicle |
mEASI change at week 4:
- 0.25% oint: −54.2% - 0.5% oint: −61.8% |
| JapicCTI-152887 [10] | II | 16–65 | Delgocitinib (oint), tacrolimus, vehicle |
mEASI change at week 4:
- 0.25% oint: −41.7% - 0.5% oint: −57.1% - 1% oint: 54.9% - 3% oint: 72.9% - vehicle: −12.2% |
| JapicCTI-173554 [11] | III | ≥16 | Delgocitinib (oint), vehicle |
mEASI change at week 4 (part 1):
- 0.5% oint: −44.3% - vehicle: −1.7%
mEASI improvement maintained through the 24-week open-label extension period (part 2)
|
| JapicCTI-184064 [12] | III | 2–15 | Delgocitinib (oint), vehicle |
mEASI change at week 4 (part 1):
- 0.25% oint: −39.3% - vehicle: −10.9%
mEASI improvement maintained through the 56-week open-label extension period (part 2)
|
| Tofacitinib (topical pan-JAK inhibitor) | ||||
| NCT02001181 [13] | II | 18–60 | Tofacitinib (oint), vehicle |
EASI change at week 4:
- 2% oint: −81.7% - vehicle: −29.9% |
| Ruxolitinib (topical selective JAK1/2 inhibitor) | ||||
| NCT03745638 (TRuE AD1) [14] | III | ≥12 | Ruxolitinib (cream), vehicle |
Patients with IGA 1/0 at week 8:
- 0.75% cream: 50% - 1.5% cream: 53.8% - vehicle: 15.1% |
| NCT03745651 (TRuE AD2) [14] | III | ≥12 | Ruxolitinib (cream), vehicle |
Patients with IGA 1/0 at week 8:
- 0.75% cream: 39% - 1.5% cream: 51.3% - vehicle: 7.6% |
| Baricitinib (systemic selective JAK1/2 inhibitor) | ||||
| NCT02576938 [15] | II | ≥18 years | Baricitinib, placebo, TCS |
Patients with EASI-50 at week 16:
- 2 mg: 57% - 4 mg: 61% - placebo: 37% |
| NCT03334396 (BREEZE-AD1) [16] | III | ≥18 years | Baricitinib, placebo |
Patients with IGA 0/1 at week 16:
- 1 mg: 11.8% - 2 mg: 11.4% - 4 mg: 16.8% - placebo: 4.8% |
| NCT03334422 (BREEZE-AD2) [16] | III | ≥18 years | Baricitinib, placebo |
Patients with IGA 0/1 at week 16:
- 1 mg: 8.8% - 2 mg: 10.6% - 4 mg: 13.8% - placebo: 4.5% |
| NCT03334435 (BREEZE-AD3) [17] | III | ≥18 years | Baricitinib (long-term extension of BREEZE-AD1 and BREEZE-AD2) |
Patients with IGA 0/1 at week 68:
- 2 mg: 59.3% - 4 mg: 47.1% |
| NCT03428100 (BREEZE-AD4) [18] | III | ≥18 years | Baricitinib, placebo, TCS |
Patients with EASI-75 at week 16:
- 2 mg: 28% - 4 mg: 32% - placebo: 17% |
| NCT03435081 (BREEZE-AD5) [19] | III | ≥18 years | Baricitinib, placebo |
Patients with EASI-75 at week 16:
- 1 mg: 13% - 2 mg: 30% - placebo: 8% |
| NCT03559270 (BREEZE-AD6) * | III | ≥18 years | Baricitinib | Active, not recruiting |
| NCT03733301 (BREEZE-AD7) [20] | III | ≥18 years | Baricitinib, placebo, TCS |
Patients with IGA 0/1 at week 16:
- 2 mg: 24% - 4 mg: 31% - placebo: 15% |
| NCT03952559 (BREEZE-AD Peds) * | III | 2–17 years | Baricitinib, placebo, TCS | Recruiting |
| Upadacitinib (systemic selective JAK 1 inhibitor) | ||||
| NCT02925117 [21] | II | 18–75 years | Upadacitinib, placebo |
EASI improvement at week 16:
- 7.5 mg: 39% - 15 mg: 62% - 30 mg: 74% - placebo: 23% |
| NCT03569293 (Measure Up-1) [22,23] | III | 12–75 years | Upadacitinib, placebo |
Patients with EASI-75 at week 16:
- 15 mg: 70% - 30 mg: 80% - placebo: 16% |
| NCT03607422 (Measure Up-2) [22,23] | III | 12–75 years | Upadacitinib, placebo |
Patients with EASI-75 at week 16:
- 15 mg: 60% - 30 mg: 73% - placebo: 13% |
| NCT03568318 (AD Up) [24,25] | III | 12–75 years | Upadacitinib, placebo, TCS |
Patients with EASI-75 at week 16:
- 15 mg: 65% - 30 mg: 77% - placebo: 23%
Patients with IGA 0/1 at week 16:
- 15 mg: 40% - 30 mg: 59% - placebo: 11% |
| NCT03738397 (Heads Up) [26] | III | 12–75 years | Upadacitinib, dupilumab |
Patients with EASI-75 at week 16:
- Upadacitinib 30 mg: 71% - Dupilumab: 61.1% |
| NCT03661138 (Rising Up) [27] | III | 12–75 years | Upadacitinib, placebo, TCS | n/a (safety analysis) |
| NCT04195698 * | III | 18–75 years | Upadacitinib | Active, not recruiting |
| Abrocitinib (systemic JAK 1 inhibitor) | ||||
| NCT02780167 [28] | II | 18–75 years | Abrocitinib, placebo |
Patients with IGA 0/1 at week 12:
- 10 mg: 40% (10.9%) - 30 mg: 59% (8.9%) - 100 mg: 29.6% - 200 mg: 43.8% - placebo: 5.8% |
| NCT04345367 * | III | ≥18 years | Abrocitinib, dupilumab | not yet available |
| NCT03349060 (JADE MONO-1) [29] | III | ≥12 years | Abrocitinib, placebo |
Patients with IGA 0/1 at week 12:
- 100 mg: 44% - 200 mg: 24% - placebo: 8% |
| NCT03575871 (JADE MONO-2) [30] | III | ≥12 years | Abrocitinib, placebo |
Patients with IGA 0/1 at week 12:
- 100 mg: 44% - 200 mg: 24% - placebo: 8% |
| NCT03796676 (JADE TEEN) [31] | III | 12–17 years | Abrocitinib, placebo |
Patients with EASI-75 at week 12:
- 100 mg: 44.5% - 200 mg: 61% - placebo: 10.4%
Patients with IGA 0/1 at week 12:
- 100 mg: 38.1% - 200 mg: 28.4% - placebo: 9.1% |
| NCT03627767 (JADE REGIMEN) [32] | III | ≥12 years | Abrocitinib, placebo | n/a (assessment of treatment modification on AD symptoms/flares) |
| NCT03720470 (JADE COMPARE) [33] | III | ≥18 years | Abrocitinib, dupilumab, placebo |
Patients with EASI-75 at week 12:
- 100 mg: 58.7% - 200 mg: 70.3% - dupilumab: 58.1% - placebo: 27.1%
Patients with IGA 0/1 at week 12:
- 100 mg: 36.6% - 200 mg: 48.4% - dupilumab: 36.5% - placebo: 14% |
| NCT03422822 (JADE EXTEND) [34] | III | ≥12 years | Abrocitinib (extension study after switching from dupilumab) |
Patients (Dupilumab-responders) with EASI-75 at week 12:
- 100 mg: 90.2% - 200 mg: 93.5%
Patients (Dupilumab-non-responders) with EASI-75 at week 12:
- 100 mg: 67.7% - 200 mg: 80% |
| NCT05375929 * | III | ≥12 years | Abrocitinib | Not yet recruiting |
| SHR0302 (systemic selective JAK 1 inhibitor) | ||||
| NCT04717310 (MARBLE-23) * | II/III | ≥12 | SHR0302 (oint), vehicle | Recruiting |
| NCT04162899 [35] | II | 18–75 | SHR0302 |
Patients with IGA 0/1 at week 12:
- 4 mg: 25.7% - 8 mg: 54.3% - placebo: 5.7% |
| NCT04875169 * | III | ≥12 | SHR0302, placebo | Active, not recruiting |
| JAK Inhibitor | IC50 Values (nM) | Indications | |||
|---|---|---|---|---|---|
| JAK1 | JAK2 | JAK3 | TYK2 | ||
| Baricitinib (JAK1/2) | 4.0 | 6.6 | 787 | 61 | AD |
| Upadacitinib (JAK1) | 43 | 120 | 2300 | 4700 | AD, RA, AS |
| Abrocitinib (JAK1) | 29 | 803 | >10.000 | 1259 | AD |
| Tofacitinib (JAK1/2/3) | 15 | 77 | 55 | 489 | RA, AS, PsA, UC, JIA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsiogka, A.; Kyriazopoulou, M.; Kontochristopoulos, G.; Nicolaidou, E.; Stratigos, A.; Rigopoulos, D.; Gregoriou, S. The JAK/STAT Pathway and Its Selective Inhibition in the Treatment of Atopic Dermatitis: A Systematic Review. J. Clin. Med. 2022, 11, 4431. https://doi.org/10.3390/jcm11154431
Tsiogka A, Kyriazopoulou M, Kontochristopoulos G, Nicolaidou E, Stratigos A, Rigopoulos D, Gregoriou S. The JAK/STAT Pathway and Its Selective Inhibition in the Treatment of Atopic Dermatitis: A Systematic Review. Journal of Clinical Medicine. 2022; 11(15):4431. https://doi.org/10.3390/jcm11154431
Chicago/Turabian StyleTsiogka, Aikaterini, Maria Kyriazopoulou, George Kontochristopoulos, Electra Nicolaidou, Alexander Stratigos, Dimitris Rigopoulos, and Stamatios Gregoriou. 2022. "The JAK/STAT Pathway and Its Selective Inhibition in the Treatment of Atopic Dermatitis: A Systematic Review" Journal of Clinical Medicine 11, no. 15: 4431. https://doi.org/10.3390/jcm11154431