
Serum and Adipose Dipeptidyl Peptidase 4 in Cardiovascular Surgery Patients: Influence of Dipeptidyl Peptidase 4 Inhibitors

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. ELISA
2.3. Adipose Tissue Collection
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Serum Adipokine Levels and Adipokine Protein Expression in Both SAT and EAT
3.3. Correlation between DPP-4 and Other Parameters in Serum, SAT, and EAT
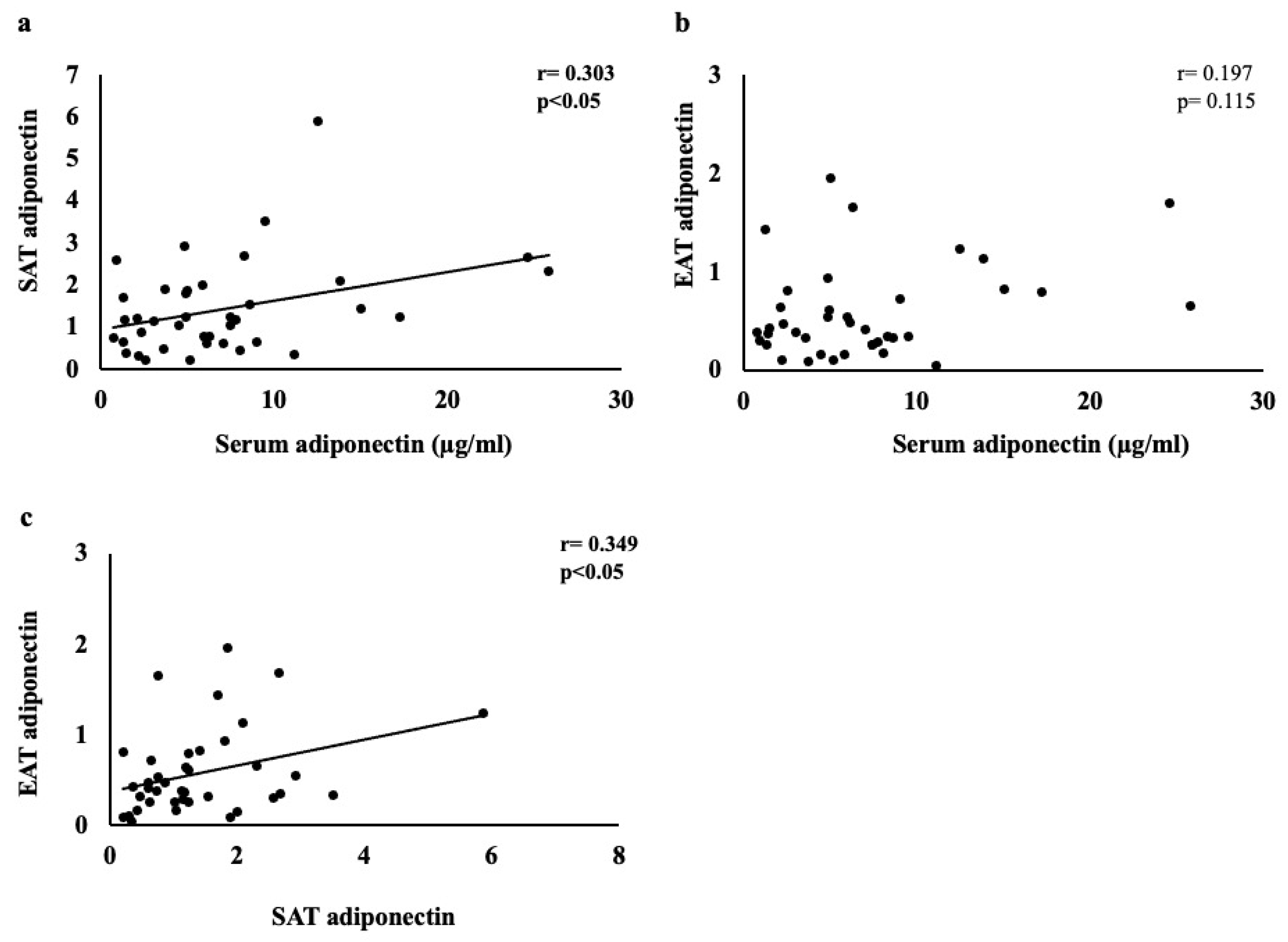
3.4. Correlation between Adiponectin and Other Parameters in Serum, SAT, and EAT
3.5. Effects on Serum, SAT, and EAT between Patient Groups Taking DPP-4 Inhibitors and Those Not Taking Them
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study.GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Lainscak, M.; Blue, L.; Clark, A.L.; Dahlström, U.; Dickstein, K.; Ekman, I.; McDonagh, T.; McMurray, J.J.; Ryder, M.; Stewart, S.; et al. Self-care management of heart failure: Practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2011, 13, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Yazıcı, D.; Özben, B.; Yavuz, D.; Deyneli, O.; Aydın, H.; Tarcin, Ö.; Akalın, S. Epicardial adipose tissue thickness in type 1 diabetic patients. Endocrine 2011, 40, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Mahabadi, A.A.; Lehmann, N.; Möhlenkamp, S.; Pundt, N.; Dykun, I.; Roggenbuck, U.; Moebus, S.; Jöckel, K.H.; Erbel, R.; Kälsch, H.; et al. Noncoronary Measures Enhance the Predictive Value of Cardiac CT Above Traditional Risk Factors and CAC Score in the General Population. JACC Cardiovasc. Imaging 2016, 9, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Elie, A.G.; Jensen, P.S.; Nissen, K.D.; Geraets, I.M.; Xu, A.; Song, E.; Hansen, M.L.; Irmukhamedov, A.; Rasmussen, L.M.; Wang, Y.; et al. Adipokine Imbalance in the Pericardial Cavity of Cardiac and Vascular Disease Patients. PLoS ONE 2016, 11, e0154693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonopoulos, A.S.; Antoniades, C. The role of epicardial adipose tissue in cardiac biology: Classic concepts and emerging roles. J. Physiol. 2017, 595, 3907–3917. [Google Scholar] [CrossRef]
- Shibasaki, I.; Nishikimi, T.; Mochizuki, Y.; Yamada, Y.; Yoshitatsu, M.; Inoue, Y.; Kuwata, T.; Ogawa, H.; Tsuchiya, G.; Ishimitsu, T.; et al. Greater expression of inflammatory cytokines, adrenomedullin, and natriuretic peptide receptor-C in epicardial adipose tissue in coronary artery disease. Regul. Pept. 2010, 165, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Trasancos, Á.; Agra, R.M.; García-Acuña, J.M.; Fernández, Á.L.; González-Juanatey, J.R.; Eiras, S. Omentin treatment of epicardial fat improves its anti-inflammatory activity and paracrine benefit on smooth muscle cells. Obesity 2017, 25, 1042–1049. [Google Scholar] [CrossRef]
- Bettencourt, N.; Toschke, A.M.; Leite, D.; Rocha, J.; Carvalho, M.; Sampaio, F.; Xará, S.; Leite-Moreira, A.; Nagel, E.; Gama, V. Epicardial adipose tissue is an independent predictor of coronary atherosclerotic burden. Int. J. Cardiol. 2012, 158, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, T.; Opolski, G. Pericoronary Adipose Tissue: A Novel Therapeutic Target in Obesity-Related Coronary Atherosclerosis. J. Am. Coll. Nutr. 2015, 34, 244–254. [Google Scholar] [CrossRef]
- Harada, K.; Amano, T.; Kataoka, T.; Takeshita, M.; Harada, K.; Kunimura, A.; Takayama, Y.; Shinoda, N.; Kato, B.; Uetani, T.; et al. Impact of abdominal and epicardial fat on the association between plasma adipocytokine levels and coronary atherosclerosis in non-obese patients. Atherosclerosis 2014, 237, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Sato, F.; Maeda, N.; Yamada, T.; Namazui, H.; Fukuda, S.; Natsukawa, T.; Nagao, H.; Murai, J.; Masuda, S.; Tanaka, Y.; et al. Association of Epicardial, Visceral, and Subcutaneous Fat With Cardiometabolic Diseases. Circ. J. 2018, 82, 502–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorter, P.M.; de Vos, A.M.; van der Graaf, Y.; Stella, P.R.; Doevendans, P.A.; Meijs, M.F.; Prokop, M.; Visseren, F.L. Relation of Epicardial and Pericoronary Fat to Coronary Atherosclerosis and Coronary Artery Calcium in Patients Undergoing Coronary Angiography. Am. J. Cardiol. 2008, 102, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Wang, D.; Zeb, I.; Budoff, M.J.; Harman, S.M.; Miller, V.; Brinton, E.A.; El Khoudary, S.R.; Manson, J.E.; Sowers, M.R.; et al. Intra-thoracic fat, cardiometabolic risk factors, and subclinical cardiovascular disease in healthy, recently menopausal women screened for the Kronos Early Estrogen Prevention Study (KEEPS). Atherosclerosis 2012, 221, 198–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahabadi, A.A.; Lehmann, N.; Kälsch, H.; Robens, T.; Bauer, M.; Dykun, I.; Budde, T.; Moebus, S.; Jöckel, K.H.; Erbel, R.; et al. Association of Epicardial Adipose Tissue With Progression of Coronary Artery Calcification Is More Pronounced in the Early Phase of Atherosclerosis: Results From the Heinz Nixdorf Recall Study. JACC Cardiovasc. Imaging 2014, 7, 909–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.J.; Pedley, A.; Hoffmann, U.; Massaro, J.M.; Levy, D.; Long, M.T. Visceral and Intrahepatic Fat Are Associated with Cardiometabolic Risk Factors Above Other Ectopic Fat Depots: The Framingham Heart Study. Am. J. Med. 2018, 131, 684–692.e12. [Google Scholar] [CrossRef]
- Iacobellis, G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nat. Rev. Endocrinol. 2015, 11, 363–371. [Google Scholar] [CrossRef]
- Wu, F.Z.; Wu, C.C.; Kuo, P.-L.; Wu, M.-T. Differential impacts of cardiac and abdominal ectopic fat deposits on cardiometabolic risk stratification. BMC Cardiovasc. Disord. 2016, 16, 20. [Google Scholar] [CrossRef] [Green Version]
- Matteucci, E.; Giampietro, O. Dipeptidyl Peptidase-4 (CD26): Knowing the Function before Inhibiting the Enzyme. Curr. Med. Chem. 2009, 16, 2943–2951. [Google Scholar] [CrossRef]
- Yazbeck, R.; Howarth, G.S.; Abbott, C. Dipeptidyl peptidase inhibitors, an emerging drug class for inflammatory disease? Trends Pharmacol. Sci. 2009, 30, 600–607. [Google Scholar] [CrossRef]
- Klemann, C.; Wagner, L.; Stephan, M.; von Hörsten, S. Cut to the chase: A review of CD26/dipeptidyl peptidase-4′s (DPP4) entanglement in the immune system. Clin. Exp. Immunol. 2016, 185, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.; Egan, J.M. The Role of Incretins in Glucose Homeostasis and Diabetes Treatment. Pharmacol. Rev. 2008, 60, 470–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggio, L.L.; Drucker, D.J. Biology of Incretins: GLP-1 and GIP. Gastroenterology 2007, 132, 2131–2157. [Google Scholar] [CrossRef] [PubMed]
- Lamers, D.; Famulla, S.; Wronkowitz, N.; Hartwig, S.; Lehr, S.; Ouwens, D.M.; Eckardt, K.; Kaufman, J.M.; Ryden, M.; Müller, S.; et al. Dipeptidyl Peptidase 4 Is a Novel Adipokine Potentially Linking Obesity to the Metabolic Syndrome. Diabetes 2011, 60, 1917–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinitsky, M.Y.; Dyleva, Y.A.; Uchasova, E.G.; Belik, E.V.; Yuzhalin, A.E.; Gruzdeva, O.V.; Matveeva, V.G.; Ponasenko, A.V. Adipokine gene expression in adipocytes isolated from different fat depots of coronary artery disease patients. Arch. Physiol. Biochem. 2022, 128, 261–269. [Google Scholar] [CrossRef]
- White, W.B.; Cannon, C.P.; Heller, S.R.; Nissen, S.E.; Bergenstal, R.M.; Bakris, G.L.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; et al. Alogliptin after Acute Coronary Syndrome in Patients with Type 2 Diabetes. N. Engl. J. Med. 2013, 369, 1327–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef] [Green Version]
- Kadowaki, T.; Wang, G.; Rosenstock, J.; Yabe, D.; Peng, Y.; Kanasaki, K.; Mu, Y.; Mattheus, M.; Keller, A.; Okamura, T.; et al. Effect of linagliptin, a dipeptidyl peptidase-4 inhibitor, compared with the sulfonylurea glimepiride on cardiovascular outcomes in Asians with type 2 diabetes: Subgroup analysis of the randomized CAROLINA® trial. Diabetol. Int. 2020, 12, 87–100. [Google Scholar] [CrossRef]
- Inagaki, N.; Yang, W.; Watada, H.; Ji, L.; Schnaidt, S.; Pfarr, E.; Okamura, T.; Johansen, O.E.; George, J.T.; von Eynatten, M.; et al. Linagliptin and cardiorenal outcomes in Asians with type 2 diabetes mellitus and established cardiovascular and/or kidney disease: Subgroup analysis of the randomized CARMELINA® trial. Diabetol. Int. 2019, 11, 129–141. [Google Scholar] [CrossRef]
- Kos, K.; Baker, A.R.; Jernas, M.; Harte, A.L.; Clapham, J.C.; O’Hare, J.P.; Carlsson, L.; Kumar, S.; McTernan, P.G. DPP-IV inhibition enhances the antilipolytic action of NPY in human adipose tissue. Diabetes Obes. Metab. 2009, 11, 285–292. [Google Scholar] [CrossRef]
- Iwaki-Egawa, S.; Watanabe, Y.; Kikuya, Y.; Fujimoto, Y. Dipeptidyl peptidase IV from human serum: Purification, characterization, and N-terminal amino acid sequence. J. Biochem. 1998, 124, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Ahrén, B. Dipeptidyl Peptidase-4 Inhibitors: Clinical Data and Clinical Implications. Diabetes Care 2007, 30, 1344–1350. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Nangaku, M.; Nishiyama, A. The Role of Incretins in Salt-Sensitive Hypertension: The Potential Use of Dipeptidyl Peptidase-IV Inhibitors. Curr. Opin. Nephrol. Hypertens. 2011, 20, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Agra, R.M.; Fernández-Trasancos, Á.; Díaz-Rodríguez, E.; Cordero, A.; Varela-Román, A.; Gómez-Otero, I.; Canoa, J.N.L.; Fernández, Á.L.; Martínez-Cereijo, J.M.; González-Juanatey, J.R.; et al. Nutrients Restriction Upregulates Adiponectin in Epicardial or Subcutaneous Adipose Tissue: Impact in de Novo Heart Failure Patients. Int. J. Med. Sci. 2018, 15, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, J.P.; Richards, A.A.; Hickman, I.J.; Macdonald, G.A.; Prins, J.B. Adiponectin—A Key Adipokine in the Metabolic Syndrome. Diabetes Obes. Metab. 2006, 8, 264–280. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Li, L.; Wang, X.; Greene, T.; Balakrishnan, V.; Madero, M.; Pereira, A.A.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; et al. Adiponectin and Mortality in Patients With Chronic Kidney Disease. J. Am. Soc. Nephrol. 2006, 17, 2599–2606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruzdeva, O.; Uchasova, E.; Dyleva, Y.; Borodkina, D.; Akbasheva, O.; Antonova, L.; Matveeva, V.; Belik, E.; Ivanov, S.; Sotnikov, A.; et al. Adipocytes Directly Affect Coronary Artery Disease Pathogenesis via Induction of Adipokine and Cytokine Imbalances. Front. Immunol. 2019, 10, 2163. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbons, T.P.; Czech, M.P. Epicardial and Perivascular Adipose Tissues and Their Influence on Cardiovascular Disease: Basic Mechanisms and Clinical Associations. J. Am. Heart Assoc. 2014, 3, e000582. [Google Scholar] [CrossRef] [Green Version]
- Greenstein, A.S.; Khavandi, K.; Withers, S.B.; Sonoyama, K.; Clancy, O.; Jeziorska, M.; Laing, I.; Yates, A.P.; Pemberton, P.W.; Malik, R.A.; et al. Local Inflammation and Hypoxia Abolish the Protective Anticontractile Properties of Perivascular Fat in Obese Patients. Circulation 2009, 119, 1661–1670. [Google Scholar] [CrossRef] [Green Version]
- Mazurek, T.; Zhang, L.; Zalewski, A.; Mannion, J.D.; Diehl, J.T.; Arafat, H.; Sarov-Blat, L.; O’Brien, S.; Keiper, E.A.; Johnson, A.G.; et al. Human Epicardial Adipose Tissue Is a Source of Inflammatory Mediators. Circulation 2003, 108, 2460–2466. [Google Scholar] [CrossRef] [Green Version]
- Adegoke, T.E.; Sabinari, I.W.; Areola, E.D.; Ajao, F.; Asafa, O.O.; Soluoku, T.K.; Bello, A.; Adesanmi, A.M.; Yusuf, S.O.; Omoleye, A.; et al. Inhibition of dipeptidyl peptidase-4 averts free fatty acids deposition in the hearts of oral estrogen–progestin contraceptive-induced hyperinsulinemic female rats. Can. J. Physiol. Pharmacol. 2021, 99, 1316–1323. [Google Scholar] [CrossRef]
- Onogi, Y.; Wada, T.; Kamiya, C.; Inata, K.; Matsuzawa, T.; Inaba, Y.; Kimura, K.; Inoue, H.; Yamamoto, S.; Ishii, Y.; et al. PDGFRβ Regulates Adipose Tissue Expansion and Glucose Metabolism via Vascular Remodeling in Diet-Induced Obesity. Diabetes 2017, 66, 1008–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkmen, K.; Kayikcioglu, H.; Ozbek, O.; Solak, Y.; Kayrak, M.; Samur, C.; Anil, M.; Zeki Tonbul, H.Z. The Relationship between Epicardial Adipose Tissue and Malnutrition, Inflammation, Atherosclerosis/Calcification Syndrome in ESRD Patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 1920–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Marco, L.G.; Bellasi, A.; Kim, S.; Chen, Z.; Block, G.A.; Raggi, P. Epicardial adipose tissue predicts mortality in incident hemodialysis patients: A substudy of the Renagel in New Dialysis trial. Nephrol. Dial. Transplant. 2013, 28, 2586–2595. [Google Scholar] [CrossRef] [Green Version]
- Middeldorp, M.E.; Pathak, R.K.; Meredith, M.; Mehta, A.B.; Elliott, A.D.; Mahajan, R.; Twomey, D.; Gallagher, C.; Hendriks, J.M.L.; Linz, D.; et al. PREVEntion and regReSsive Effect of weight-loss and risk factor modification on Atrial Fibrillation: The REVERSE-AF study. Europace 2018, 20, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Nalliah, C.J.; Bell, J.R.; Raaijmakers, A.J.; Waddell, H.M.; Wells, S.P.; Bernasochi, G.B.; Montgomery, M.K.; Binny, S.; Watts, T.; Joshi, S.B.; et al. Epicardial Adipose Tissue Accumulation Confers Atrial Conduction Abnormality. J. Am. Coll. Cardiol. 2020, 76, 1197–1211. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Chilton, E.; Raman, J.; Saxena, P.; McFarlane, C.; Trollope, A.F.; Kinobe, R.; Chilton, L. Are Interactions between Epicardial Adipose Tissue, Cardiac Fibroblasts and Cardiac Myocytes Instrumental in Atrial Fibrosis and Atrial Fibrillation? Cells 2021, 10, 2501. [Google Scholar] [CrossRef]
- Bilal, M.; Nawaz, A.; Kado, T.; Aslam, M.R.; Igarashi, Y.; Nishimura, A.; Watanabe, Y.; Kuwano, T.; Liu, J.; Miwa, H.; et al. Fate of adipocyte progenitors during adipogenesis in mice fed a high-fat diet. Mol. Metab. 2021, 54, 101328. [Google Scholar] [CrossRef]
- Watanabe, E.; Wada, T.; Okekawa, A.; Kitamura, F.; Komatsu, G.; Onogi, Y.; Yamamoto, S.; Sasahara, M.; Kitada, M.; Koya, D.; et al. Stromal cell-derived factor 1 (SDF1) attenuates platelet-derived growth factor-B (PDGF-B)-induced vascular remodeling for adipose tissue expansion in obesity. Angiogenesis 2020, 23, 667–684. [Google Scholar] [CrossRef] [PubMed]
- Aso, Y.; Kase, M.; Sagara, M.; Sakurai, S.; Iijima, T.; Tomaru, T.; Jojima, T.; Usui, I. Teneligliptin, a DPP-4 Inhibitor, Decreases Plasma Levels of Inflammatory Chemokines During a Standard Meal Test in Patients With Type 2 Diabetes. Am. J. Med. Sci. 2020, 360, 261–267. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients, Number | 40 |
|---|---|
| Male, n (%) | 25 (62.5) |
| Age, years | 67.5 ± 13.8 |
| BMI, kg/m2 | 24.7 ± 4.4 |
| Diagnosis | |
| Ischemic heart disease, n (%) | 13 (32.5) |
| Valvular disease, n (%) | 24 (60.0) |
| Aortic disease, n (%) | 11 (27.5) |
| Atherosclerosis b, n (%) | 17 (42.5) |
| NYHA | 2.1 ± 1.2 |
| ECG | |
| Atrial fibrillation | 11 (27.5) |
| Comorbidity | |
| Diabetes, n (%) | 15 (37.5) |
| DPP-4 inhibitors (+), n (%) | 10 (25.0) |
| Sitagliptin, n (%) | 5 (50.0) |
| Teneligliptin, n (%) | 3 (30.0) |
| Linagliptin, n (%) | 1 (10.0) |
| Vildagliptin, n (%) | 1 (10.0) |
| Hypertension, n (%) | 29 (72.5) |
| Dyslipidemia, n (%) | 17 (42.5) |
| Smoking, n (%) | 5 (12.5) |
| Hemodialysis, n (%) | 4 (10.0) |
| Fasting blood glucose, mg/dL | 117.8 ± 34.2 |
| Creatinine, mg/dL | 1.25 ± 1.30 |
| eGFR, mL/min/1.73 m2 | 62.3 ± 25.4 |
| Total cholesterol a, mg/dL | 175.1 ± 40.2 |
| High-density-lipoprotein cholesterol, mg/dL | 51.8± 16.9 |
| Low-density-lipoprotein cholesterol, mg/dL | 98.2 ± 29.1 |
| Triglycerides, mg/dL | 114.5 ± 69.0 |
| Triglycerides/high-density lipoprotein cholesterol | 2.4 ± 1.6 |
| C-reactive protein, mg/dL | 1.0 ± 1.8 |
| BNP, pg/mL | 329.9 ± 490.7 |
| Hemoglobin A1c, % | 6.2 ± 0.9 |
| TTE | |
| AoD, mm | 32.5 ± 8.3 |
| LAD, mm | 44.2 ± 9.5 |
| EF, % | 56.7 ± 9.0 |
| Number of coronary artery lesions, ischemic heart disease (13 patients) | 2.3 ± 0.9 |
| Serum levels | |
| Adiponectin, µg/mL | 7.0 ± 5.9 |
| Leptin a, pg/mL | 5712.6 ± 6095.4 |
| DPP-4 a, ng/mL | 172.6 ± 57.6 |
| DPP-4 activity, RFU/s | 3.8 ± 1.7 |
| Subcutaneous adipose | |
| DPP-4 | 1.15 ± 0.71 |
| Adiponectin | 1.41 ± 1.10 |
| TNFα | 2.32 ± 1.22 |
| Epicardial adipose | |
| DPP-4 | 0.86 ± 0.63 |
| Adiponectin | 0.58 ± 0.47 |
| TNFα | 1.86 ± 1.15 |
| Spearman’s Rank | |
|---|---|
| Serum DPP-4 level (ng/mL) | |
| BMI | 0.109 (0.528) |
| Hypertension | −0.357 (0.033 *) |
| Triglycerides/high-density lipoprotein cholesterol | −0.068 (0.694) |
| Serum DPP-4 activity | 0.618 (<0.001 ***) |
| Serum DPP-4 activity (RFU/s) | |
| BMI | −0.164 (0.312) |
| Diabetes mellitus | −0.333 (0.036 *) |
| Fasting blood glucose | −0.347 (0.028 *) |
| Triglycerides/high-density-lipoprotein cholesterol | −0.207 (0.199) |
| Serum DPP-4 level | 0.618 (<0.001 ***) |
| Subcutaneous adipose adiponectin | 0.433 (0.003 **) |
| Epicardial adipose adiponectin | 0.355 (0.012 *) |
| Subcutaneous adipose tissue DPP-4 | |
| BMI | 0.180 (0.267) |
| Atherosclerosis a | 0.458 (0.003 **) |
| Diabetes mellitus | 0.427 (0.016 *) |
| DPP-4 inhibitors | 0.430 (0.006 **) |
| Fasting blood glucose | 0.330 (0.044 *) |
| Triglycerides/high-density-lipoprotein cholesterol | −0.170 (0.296) |
| Epicardial adipose tissue DPP-4 | 0.327 (0.020 *) |
| Subcutaneous adipose tissue adiponectin | −0.293 (0.035 *) |
| Epicardial adipose tissue DPP-4 | |
| BMI | 0.169 (0.298) |
| Atrial fibrillation | 0.323 (0.042 *) |
| Triglycerides/high-density lipoprotein cholesterol | −0.249 (0.121) |
| eGFR | −0.319 (0.045 *) |
| Subcutaneous adipose tissue DPP-4 | 0.327 (0.020 *) |
| Serum adiponectin level | 0.301 (0.031 *) |
| Spearman’s Rank | |
|---|---|
| Serum Adiponectin (µg/mL) | |
| Age | 0.268 (0.049 *) |
| BMI | −0.276 (0.045 *) |
| Hemodialysis | 0.291 (0.036 *) |
| NYHA | 0.435 (0.003 **) |
| Atrial fibrillation | 0.420 (0.004 **) |
| Creatinine | 0.275 (0.045 *) |
| eGFR | −0.406 (0.005 **) |
| Triglycerides | −0.460 (0.002 **) |
| C-reactive protein | 0.328 (0.021 *) |
| Triglycerides/high-density lipoprotein cholesterol | −0.428 (0.003 **) |
| BNP | 0.738 (<0.01 **) |
| LAD | 0.315 (0.027 *) |
| Subcutaneous adipose tissue adiponectin | 0.303 (0.030 *) |
| Epicardial adipose tissue DPP-4 | 0.301 (0.031 *) |
| Subcutaneous adipose tissue adiponectin | |
| BMI | −0.215 (0.095) |
| Aortic disease | −0.303 (0.031 *) |
| NYHA | 0.347 (0.015 *) |
| Diabetes mellitus | −0.365 (0.011 *) |
| DPP-4 inhibitors (+) | −0.438 (0.003 **) |
| Triglycerides/high-density-lipoprotein cholesterol | −0.033 (0.421) |
| Leptin | −0.512 (0.002 **) |
| DPP-4 activity | 0.433 (0.003 **) |
| Subcutaneous-adipose-tissue DPP-4 | −0.293 (0.035 *) |
| Epicardial adipose tissue adiponectin | 0.341 (0.017 *) |
| Epicardial adipose tissue Adiponectin | |
| BMI | −0.289 (0.035 *) |
| Aortic disease | −0.439 (0.002 **) |
| NYHA | 0.297 (0.031 *) |
| Hypertension | −0.279 (0.041 *) |
| Total cholesterol | −0.274 (0.046 *) |
| Triglycerides | −0.292 (0.034 *) |
| Triglycerides/high-density-lipoprotein cholesterol | −0.158 (0.165) |
| AoD | −0.328 (0.021 *) |
| Leptin | −0.615 (<0.001 ***) |
| DPP-4 activity | 0.355 (0.012 *) |
| Subcutaneous adipose tissue Adiponectin | 0.341 (0.017 *) |
| DPP-4 Inhibitors (−) | DPP-4 Inhibitors (+) | p-Value c | Effect Size e | |
|---|---|---|---|---|
| Patients, Number | 30 | 10 | ||
| Male, n (%) | 19 (63.3) | 6 (60.0) | 0.850 | |
| Age, years | 66.6 ± 15.2 | 70.0 ± 7.5 | 0.939 d | |
| BMI, kg/m2 | 24.4 ± 4.6 | 25.5 ± 3.4 | 0.612 d | |
| Diagnosis | ||||
| Ischemic heart disease, n (%) | 11 (36.7) | 6 (60.0) | 0.196 | |
| Valvular disease, n (%) | 13 (43.3) | 3 (30.0) | 0.456 | |
| Aortic disease, n (%) | 6 (20.0) | 1 (10.0) | 0.471 | |
| Atherosclerosis b, n (%) | 9 (30.0) | 6 (60.0) | 0.090 | |
| NYHA | 2.2 ± 1.2 | 1.8 ± 1.0 | 0.414 d | |
| ECG | ||||
| Atrial fibrillation | 9 (30.0) | 2 (20.0) | 0.540 | |
| Comorbidity | ||||
| Diabetes, n (%) | 5 (16.7) | 10 (100) | <0.001 *** | |
| Hypertension, n (%) | 20 (66.7) | 9 (90.0) | 0.152 | |
| Dyslipidemia, n (%) | 12 (40.0) | 5 (50.0) | 0.580 | |
| Smoking, n (%) | 3 (10.0) | 2 (20.0) | 0.408 | |
| Hemodialysis, n (%) | 4 (13.3) | 0 (0) | 0.224 | |
| Fasting blood glucose, mg/dL | 106.0 ± 20.4 | 152.9 ± 40.9 | <0.001 ***d | |
| Creatinine, mg/dL | 1.37 ±1.45 | 0.90 ± 0.20 | 0.747 d | |
| eGFR, mL/min/1.73 m2 | 62.0 ± 27.2 | 63.0 ± 16.8 | 0.770 d | |
| Total cholesterol a, mg/dL | 179.8 ± 36.5 | 161.6 ± 46.6 | 0.495 d | |
| High-density-lipoprotein cholesterol, mg/dL | 52.1 ± 13.2 | 50.9 ± 25.4 | 0.286 d | |
| Low-density-lipoprotein cholesterol, mg/dL | 102.2 ± 27.6 | 86.1 ± 30.2 | 0.148 d | |
| Triglycerides, mg/dL | 115.2 ± 64.7 | 120.5 ± 79.1 | 0.890 d | |
| C-reactive protein, mg/dL | 0.89 ± 1.77 | 1.14 ± 1.83 | 0.469 d | |
| BNP, pg/mL | 388.3 ± 538.0 | 154.7 ± 130.2 | 0.770 d | |
| Hemoglobin A1c, % | 5.9 ± 0.6 | 7.3 ± 0.8 | <0.001 ***d | |
| TTE | ||||
| AoD, mm | 32.7 ± 9.1 | 31.7 ± 3.1 | 0.961 d | |
| LAD, mm | 45.2 ± 10.3 | 41.1 ± 4.0 | 0.348 d | |
| EF, % | 56.7 ± 10.2 | 56.6 ± 8.7 | 0.842 d | |
| Number of coronary-artery lesions, vessel disease | 0.7 ± 1.2 | 1.1 ± 1.3 | 0.396d | |
| Serum levels | ||||
| Adiponectin, µg/mL | 7.6 ± 6.4 | 5.3 ± 3.3 | 0.516 | γ = 0.26 |
| Leptin a, pg/mL | 6825.9 ± 7010.7 | 8543.3 ± 8702.9 | 0.368 | γ = 0.10 |
| DPP-4 a, ng/mL | 165.0 ± 50.2 | 192.5 ± 72.9 | 0.374 | γ = 0.15 |
| DPP-4 activity, RFU/s | 4.1 ± 1.6 | 2.8 ± 1.9 | 0.072 | γ = 0.29 |
| Subcutaneous adipose | ||||
| DPP-4 | 0.98 ± 0.64 | 1.66 ± 0.68 | 0.006 ** | γ = 0.59 |
| Adiponectin | 1.63 ± 1.17 | 0.74± 0.46 | 0.005 ** | γ = 0.49 |
| Epicardial adipose | ||||
| DPP-4 | 0.90 ± 0.68 | 0.73 ± 0.46 | 0.678 | γ = 0.07 |
| Adiponectin | 0.58± 0.45 | 0.57 ± 0.55 | 0.740 | γ = 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibasaki, I.; Nakajima, T.; Fukuda, T.; Hasegawa, T.; Ogawa, H.; Tsuchiya, G.; Takei, Y.; Tezuka, M.; Kato, T.; Kanazawa, Y.; et al. Serum and Adipose Dipeptidyl Peptidase 4 in Cardiovascular Surgery Patients: Influence of Dipeptidyl Peptidase 4 Inhibitors. J. Clin. Med. 2022, 11, 4333. https://doi.org/10.3390/jcm11154333
Shibasaki I, Nakajima T, Fukuda T, Hasegawa T, Ogawa H, Tsuchiya G, Takei Y, Tezuka M, Kato T, Kanazawa Y, et al. Serum and Adipose Dipeptidyl Peptidase 4 in Cardiovascular Surgery Patients: Influence of Dipeptidyl Peptidase 4 Inhibitors. Journal of Clinical Medicine. 2022; 11(15):4333. https://doi.org/10.3390/jcm11154333
Chicago/Turabian StyleShibasaki, Ikuko, Toshiaki Nakajima, Taira Fukuda, Takaaki Hasegawa, Hironaga Ogawa, Go Tsuchiya, Yusuke Takei, Masahiro Tezuka, Takashi Kato, Yuta Kanazawa, and et al. 2022. "Serum and Adipose Dipeptidyl Peptidase 4 in Cardiovascular Surgery Patients: Influence of Dipeptidyl Peptidase 4 Inhibitors" Journal of Clinical Medicine 11, no. 15: 4333. https://doi.org/10.3390/jcm11154333