
Incidence of Sleep Bruxism in Different Phenotypes of Obstructive Sleep Apnea

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
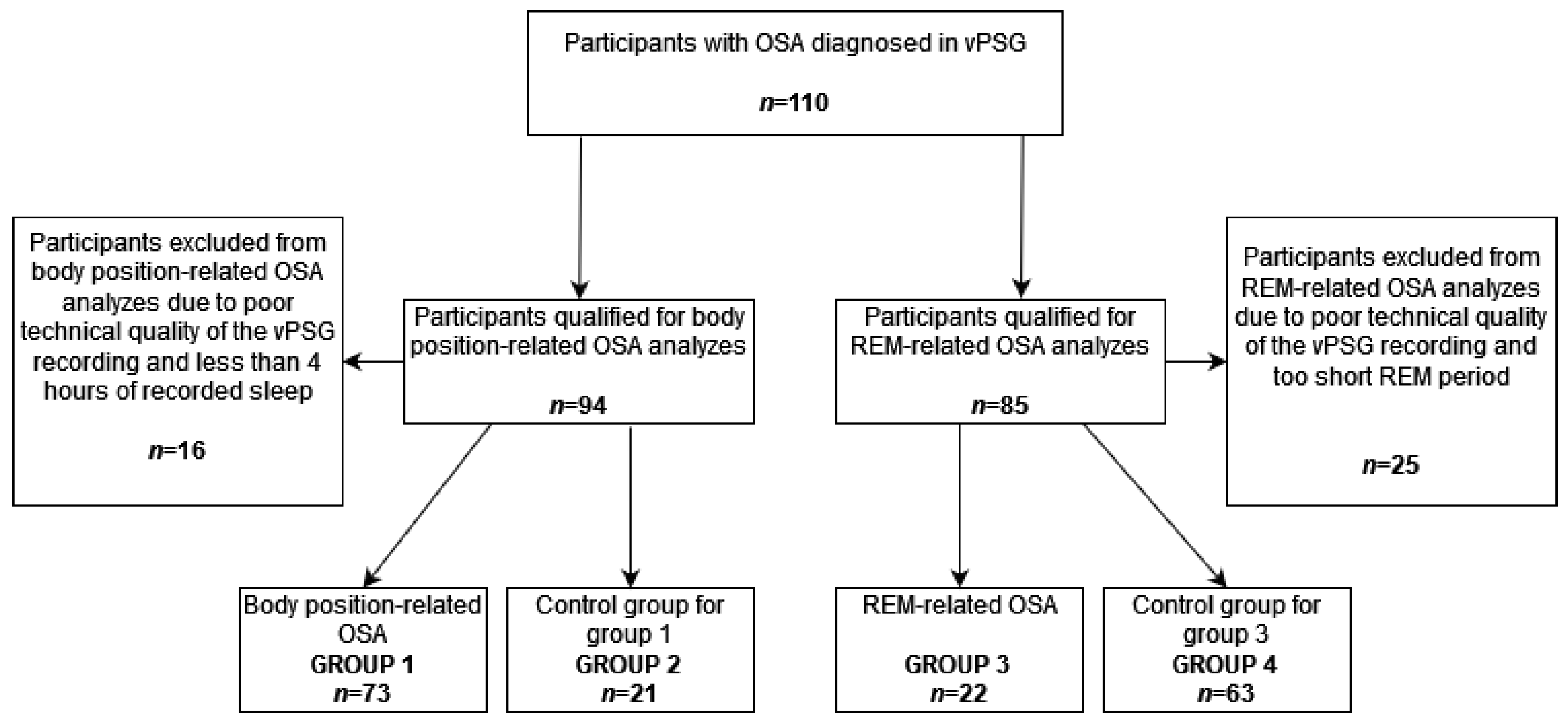
2.1. Participants
2.2. Inclusion and Exclusion Criteria
2.3. Polysomnography
2.3.1. Breathing Parameters
2.3.2. SB Parameters
2.3.3. Sleep Parameters
2.4. Obstructive Sleep Apnea Phenotypes
2.5. Qualification of the Participants into Particular Data Analyses
2.6. Data Analysis
3. Results
3.1. Body Position-Related OSA
3.2. REM-Related OSA
3.3. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Yap, A.U.; Chua, A.P. Sleep bruxism: Current knowledge and contemporary management. J. Conserv. Dent. 2016, 19, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Raphael, K.G.; Santiago, V.; Lobbezoo, F. Is bruxism a disorder or a behaviour? Rethinking the international consensus on defining and grading of bruxism. J. Oral Rehabil. 2016, 43, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manfredini, D.; Serra-Negra, J.; Carboncini, F.; Lobbezoo, F. Current Concepts of Bruxism. Int. J. Prosthodont. 2017, 30, 437–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; De Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Westchester, NY, USA, 2014; pp. 303–311. [Google Scholar]
- da Costa Lopes, A.J.; Cunha, T.C.A.; Monteiro, M.C.M.; Serra-Negra, J.M.; Cabral, L.C.; Júnior, P.C.S. Is there an association between sleep bruxism and obstructive sleep apnea syndrome? A systematic review. Sleep Breath. 2020, 24, 913–921. [Google Scholar] [CrossRef]
- Rundo, J.V. Obstructive sleep apnea basics. Clevel. Clin. J. Med. 2019, 86 (Suppl. S1), 2–9. [Google Scholar] [CrossRef] [Green Version]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Leger, D.; Bayon, V.; Laaban, J.P.; Philip, P. Impact of sleep apnea on economics. Sleep Med. Rev. 2012, 16, 455–462. [Google Scholar] [CrossRef]
- Liu, X.; Yanagawa, T.; Leopold, D.A.; Chang, C.; Ishida, H.; Fujii, N.; Duyn, J.H. Arousal transitions in sleep, wakefulness, and anesthesia are characterized by an orderly sequence of cortical events. NeuroImage 2015, 116, 222–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, T.; Katase, T.; Yamashita, S.; Sugita, H.; Muraki, H.; Mikami, A.; Okura, M.; Ohi, M.; Masuda, Y.; Taniguchi, M. Responsiveness of jaw motor activation to arousals during sleep in patients with obstructive sleep apnea syndrome. J. Clin. Sleep Med. 2013, 9, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, M.; Kato, T.; Kato-Nishimura, K.; Matsuzawa, S.; Mohri, I.; Taniike, M. Associations of sleep bruxism with age, sleep apnea, and daytime problematic behaviors in children. Oral Dis. 2016, 22, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, H.; Kitaura, H.; Hashimoto, T.; Ito, M.; Kinbara, M.; Deguchi, T.; Irokawa, T.; Ohisa, N.; Ogawa, H.; Takano-Yamamoto, T. Relationship between sleep bruxism and sleep respiratory events in patients with obstructive sleep apnea syndrome. Sleep Breath. 2014, 18, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Oksenberg, A.; Arons, E. Sleep bruxism related to obstructive sleep apnea: The effect of continuous positive airway pressure. Sleep Med. 2002, 3, 513–515. [Google Scholar] [CrossRef]
- De Luca Canto, G.; Singh, V.; Gozal, D.; Major, P.W.; Flores-Mir, C. Sleep bruxism and sleep-disordered breathing: A systematic review. J. Oral Facial Pain Headache 2014, 28, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Jokubauskas, L.; Baltrušaitytė, A. Relationship between obstructive sleep apnoea syndrome and sleep bruxism: A systematic review. J. Oral Rehabil. 2017, 44, 144–153. [Google Scholar] [CrossRef]
- Kuang, B.; Li, D.; Lobbezoo, F.; de Vries, R.; Hilgevoord, A.; de Vries, N.; Huynh, N.; Lavigne, G.; Aarab, G. Associations between sleep bruxism and other sleep-related disorders in adults: A systematic review. Sleep Med. 2022, 89, 31–47. [Google Scholar] [CrossRef]
- Martynowicz, H.; Gac, P.; Brzecka, A.; Poreba, R.; Wojakowska, A.; Mazur, G.; Smardz, J.; Wieckiewicz, M. The Relationship between Sleep Bruxism and Obstructive Sleep Apnea Based on Polysomnographic Findings. J. Clin. Med. 2019, 8, 1653. [Google Scholar] [CrossRef] [Green Version]
- Smardz, J.; Martynowicz, H.; Wojakowska, A.; Michalek-Zrabkowska, M.; Mazur, G.; Wieczorek, T.; Wieckiewicz, M. The meaning of the masticatory muscle tonic-type electromyographic pathway correlated with sleep bruxism and sleep-related breathing disorders—A polysomnographic study. Sleep Med. 2020, 68, 131–137. [Google Scholar] [CrossRef]
- Michalek-Zrabkowska, M.; Wieckiewicz, M.; Macek, P.; Gac, P.; Smardz, J.; Wojakowska, A.; Poreba, R.; Mazur, G.; Martynowicz, H. The Relationship between Simple Snoring and Sleep Bruxism: A Polysomnographic Study. Int. J. Environ. Res. Public Health 2020, 17, 8960. [Google Scholar] [CrossRef] [PubMed]
- Smardz, J.; Wieckiewicz, M.; Gac, P.; Poreba, R.; Wojakowska, A.; Mazur, G.; Martynowicz, H. Influence of age and gender on sleep bruxism and snoring in non-apneic snoring patients: A polysomnographic study. J. Sleep Res. 2020, 30, e13178. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Bogunia-Kubik, K.; Mazur, G.; Danel, D.; Smardz, J.; Wojakowska, A.; Poreba, R.; Dratwa, M.; Chaszczewska-Markowska, M.; Winocur, E.; et al. Genetic basis of sleep bruxism and sleep apnea-response to a medical puzzle. Sci. Rep. 2020, 10, 7497. [Google Scholar] [CrossRef] [PubMed]
- Martynowicz, H.; Dymczyk, P.; Dominiak, M.; Kazubowska, K.; Skomro, R.; Poreba, R.; Gac, P.; Wojakowska, A.; Mazur, G.; Wieckiewicz, M. Evaluation of Intensity of Sleep Bruxism in Arterial Hypertension. J. Clin. Med. 2018, 7, 327. [Google Scholar] [CrossRef] [Green Version]
- Wieczorek, T.; Wieckiewicz, M.; Smardz, J.; Wojakowska, A.; Michalek-Zrabkowska, M.; Mazur, G.; Martynowicz, H. Sleep structure in sleep bruxism: A polysomnographic study including bruxism activity phenotypes across sleep stages. J. Sleep Res. 2020, 29, e13028. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudgel, D.W. Sleep Apnea Severity Classification—Revisited. Sleep 2016, 39, 1165–1166. [Google Scholar] [CrossRef]
- Oksenberg, A.; Arons, E.; Nasser, K.; Vander, T.; Radwan, H. REM-related obstructive sleep apnea: The effect of body position. J. Clin. Sleep Med. 2010, 6, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Mokhlesi, B.; Punjabi, N.M. “REM-related” obstructive sleep apnea: An epiphenomenon or a clinically important entity? Sleep 2012, 35, 5–7. [Google Scholar] [CrossRef] [Green Version]
- Guven, S.F.; Ciftci, B.; Lakadamyali, H.; Ciftci, T.U. The high dependency of supine position in obstructive sleep apnea. Saudi Med. J. 2013, 34, 147–152. [Google Scholar]
- Subramani, Y.; Singh, M.; Wong, J.; Kushida, C.A.; Malhotra, A.; Chung, F. Understanding Phenotypes of Obstructive Sleep Apnea: Applications in Anesthesia, Surgery, and Perioperative Medicine. Anesth. Analg. 2017, 124, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhou, B.; Li, Z.; Lu, Q.; Li, S.; Pu, Z.; Luo, F. Gender differences of clinical and polysomnographic findings with obstructive sleep apnea syndrome. Sci. Rep. 2021, 11, 5938. [Google Scholar] [CrossRef] [PubMed]
- Joosten, S.A.; Hamza, K.; Sands, S.; Turton, A.; Berger, P.; Hamilton, G. Phenotypes of patients with mild to moderate obstructive sleep apnoea as confirmed by cluster analysis. Respirology 2012, 17, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Hong, S.-N.; Yang, S.K.; Nam, K.J.; Lim, K.H.; Hwang, S.J.; Seo, M.Y.; Lee, S.H. The effect of body position on airway patency in obstructive sleep apnea: CT imaging analysis. Sleep Breath. 2019, 23, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.; Kumar, M. Influence of body position on severity of obstructive sleep apnea: A systematic review. ISRN Otolaryngol. 2013, 2013, 670381. [Google Scholar] [CrossRef] [Green Version]
- Steffen, A.; Maibücher, L.; König, I.R. Supine position and REM dependence in obstructive sleep apnea: Critical model considerations. Rückenlage- und REM-Bezug bei obstruktiver Schlafapnoe: Kritische Modellbetrachtungen. HNO 2017, 65 (Suppl. S1), 52–58. [Google Scholar] [CrossRef]
- Gabryelska, A.; Białasiewicz, P. Association between excessive daytime sleepiness, REM phenotype and severity of obstructive sleep apnea. Sci. Rep. 2020, 10, 34. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Group 1 (n = 73) | Group 2 (n = 21) | p | |
|---|---|---|---|
| Gender a ^ | 0.46 | ||
| Male | 65.7 (48) | 57.1 (12) | |
| Female | 34.3 (25) | 42.8 (9) | |
| BMI (kg/m2) b * | 28.43 (5.40) | 31.60 (4.43) | 0.02 |
| Body mass a ^ | 0.02 | ||
| Normal | 25.0 (18) | 5.0 (1) | |
| Overweight | 38.9 (28) | 25.0 (5) | |
| Obesity | 36.1 (26) | 70.0 (14) | |
| Age (years) b # | 51.25 (14.08) | 55.48 (10.23) | 0.20 |
| AHI (/h) b * | 23.62 (15.60) | 37.03 (27.64) | 0.01 |
| SL (min) b * | 20.29 (19.49) | 22.12 (21.07) | 0.71 |
| WASO (min) b * | 55.89 (40.05) | 63.97 (38.73) | 0.41 |
| SE (%) b * | 81.26 (10.17) | 79.98 (11.16) | 0.62 |
| N1 (%TST) b * | 6.17 (4.62) | 6.57 (6.42) | 0.75 |
| N2 (%TST) b # | 48.02 (9.45) | 48.51 (12.66) | 0.85 |
| N3 (%TST) b # | 23.61 (9.35) | 23.70 (10.42) | 0.97 |
| REM (%TST) b # | 22.20 (7.65) | 21.23 (9.62) | 0.63 |
| Arousals (/h) b * | 6.59 (5.48) | 7.96 (13.28) | 0.48 |
| OA (/h) b * | 6.85 (10.10) | 15.35 (23.67) | 0.02 |
| MA (/h) b * | 0.14 (0.45) | 1.79 (5.69) | 0.01 |
| CA (/h) b * | 0.74 (2.00) | 1.53 (3.34) | 0.18 |
| ODI/h b * | 23.11 (16.17) | 36.22 (25.86) | 0.01 |
| Average SpO2 (%) b * | 92.77 (1.84) | 91.48 (3.12) | 0.02 |
| Minimal SpO2 (%) b * | 81.44 (6.11) | 78.10 (10.37) | 0.07 |
| SpO2 < 90% (%) b * | 11.22 (17.16) | 21.02 (26.81) | 0.05 |
| Average Desaturation Drop (%) b * | 4.70 (1.56) | 6.06 (3.97) | 0.02 |
| BEI (/h) b * | 4.26 (4.44) | 3.12 (4.69) | 0.31 |
| Phasic Bruxism (/h) b * | 2.18 (3.15) | 1.98 (3.90) | 0.81 |
| Tonic Bruxism (/h) b * | 1.33 (1.48) | 0.75 (0.78) | 0.09 |
| Mixed Bruxism (/h) b * | 0.78 (0.87) | 0.45 (0.59) | 0.11 |
| TST (min) b # | 414.04 (58.07) | 407.26 (65.14) | 0.65 |
| REM Latency (min) b * | 96.60 (59.09) | 92.55 (56.57) | 0.78 |
| REM AHI (/h) b * | 26.04 (19.88) | 36.06 (27.19) | 0.07 |
| Non-REM AHI (/h) b * | 22.56 (16.15) | 37.68 (29.88) | 0.00 |
| Supine AHI (/h) b * | 43.72 (29.65) | 39.77 (32.80) | 0.60 |
| Non-supine AHI (/h) b * | 9.74 (10.44) | 35.15 (27.25) | 0.00 |
| Parameter | Group 1 | Group 2 | p | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| BEI < 2 | 29 | 40 | 12 | 57 | p < 0.05 |
| BEI ≥ 2 | 44 | 60 | 9 | 43 | |
| BEI ≤ 4 | 46 | 63 | 17 | 81 | |
| BEI > 4 | 27 | 37 | 4 | 19 | |
| Group 3 (n = 22) | Group 4 (n = 63) | p | |
|---|---|---|---|
| Gender a ^ | 0.05 | ||
| Male | 50.0 (11) | 73.0 (46) | |
| Female | 50.0 (11) | 27.0 (17) | |
| BMI (kg/m2) b * | 28.59 (6.83) | 29.23 (5.13) | 0.65 |
| Body mass a ^ | 0.52 | ||
| Normal | 27.3 (6) | 21.3 (13) | |
| Overweight | 40.9 (9) | 32.8 (20) | |
| Obesity | 31.8 (7) | 45.9 (28) | |
| Age (years) b # | 49.68 (15.35) | 52.75 (12.67) | 0.36 |
| AHI (/h) b * | 17.76 (10.78) | 29.68 (21.70) | 0.02 |
| SL (min) b * | 18.17 (17.12) | 21.94 (21.32) | 0.46 |
| WASO (min) b * | 52.70 (38.39) | 60.14 (41.12) | 0.46 |
| SE (%) b * | 83.50 (8.49) | 80.14 (11.01) | 0.20 |
| N1 (%TST) b * | 3.89 (3.63) | 7.24 (5.07) | 0.01 |
| N2 (%TST) b # | 47.44 (10.63) | 48.61 (9.91) | 0.64 |
| N3 (%TST) b # | 26.36 (12.69) | 22.90 (8.56) | 0.16 |
| REM (%TST) b # | 22.33 (6.86) | 21.25 (7.35) | 0.55 |
| Arousals (/h) b * | 4.31 (3.16) | 8.09 (9.12) | 0.06 |
| OA (/h) b * | 4.93 (6.16) | 10.62 (17.03) | 0.13 |
| MA (/h) b * | 0.02 (0.07) | 0.73 (3.35) | 0.32 |
| CA (/h) b * | 0.22 (0.44) | 1.16 (2.78) | 0.12 |
| ODI/h b * | 17.17 (10.91) | 29.06 (21.28) | 0.01 |
| Average SpO2 (%) b * | 92.66 (1.65) | 92.52 (2.34) | 0.79 |
| Minimal SpO2 (%) b * | 82.91 (6.75) | 80.13 (7.64) | 0.13 |
| SpO2 < 90% (%) b * | 7.84 (14.32) | 13.71 (19.84) | 0.21 |
| Average Desaturation Drop (%) b * | 4.13 (1.10) | 5.35 (2.73) | 0.05 |
| BEI (/h) b * | 4.40 (4.17) | 4.03 (4.82) | 0.75 |
| Phasic Bruxism (/h) b * | 2.61 (3.17) | 2.10 (3.55) | 0.55 |
| Tonic Bruxism (/h) b * | 1.17 (1.45) | 1.20 (1.38) | 0.93 |
| Mixed Bruxism (/h) b * | 0.68 (0.82) | 0.76 (0.88) | 0.71 |
| TST (min) b # | 422.92 (50.75) | 408.24 (62.96) | 0.33 |
| REM Latency (min) b * | 96.25 (51.51) | 107.12 (55.57) | 0.42 |
| REM AHI (/h) b * | 34.21 (19.05) | 26.52 (23.50) | 0.17 |
| Non-REM AHI (/h) b * | 12.44 (8.74) | 30.46 (22.58) | 0.00 |
| Supine AHI (/h) b * | 30.85 (24.82) | 46.04 (31.26) | 0.04 |
| Non-supine AHI (/h) b * | 9.02 (7.73) | 17.82 (21.49) | 0.06 |
| Predictor | β | Standard Error with β | b | Standard Error with b | t (83) | p |
|---|---|---|---|---|---|---|
| Body position-related OSA | 0.059 | 0.112 | 0.642 | 1.231 | 0.521 | 0.604 |
| Gender—male (0)/female (1) | −0.246 | 0.113 | −2.328 | 1.072 | −2.171 | 0.033 |
| Body mass index | −0.068 | 0.119 | −0.058 | 0.101 | −0.576 | 0.566 |
| Age | −0.085 | 0.117 | −0.029 | 0.040 | −0.727 | 0.469 |
| Diabetes | 0.242 | 0.118 | 3.508 | 1.714 | 2.047 | 0.044 |
| Hypertension | −0.129 | 0.117 | −1.167 | 1.055 | −1.106 | 0.272 |
| Ischemic heart disease | −0.101 | 0.119 | −1.723 | 2.034 | −0.847 | 0.399 |
| Apnea/Hypopnea Index | −0.148 | 0.128 | −0.034 | 0.030 | −1.162 | 0.249 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smardz, J.; Wieckiewicz, M.; Wojakowska, A.; Michalek-Zrabkowska, M.; Poreba, R.; Gac, P.; Mazur, G.; Martynowicz, H. Incidence of Sleep Bruxism in Different Phenotypes of Obstructive Sleep Apnea. J. Clin. Med. 2022, 11, 4091. https://doi.org/10.3390/jcm11144091
Smardz J, Wieckiewicz M, Wojakowska A, Michalek-Zrabkowska M, Poreba R, Gac P, Mazur G, Martynowicz H. Incidence of Sleep Bruxism in Different Phenotypes of Obstructive Sleep Apnea. Journal of Clinical Medicine. 2022; 11(14):4091. https://doi.org/10.3390/jcm11144091
Chicago/Turabian StyleSmardz, Joanna, Mieszko Wieckiewicz, Anna Wojakowska, Monika Michalek-Zrabkowska, Rafal Poreba, Pawel Gac, Grzegorz Mazur, and Helena Martynowicz. 2022. "Incidence of Sleep Bruxism in Different Phenotypes of Obstructive Sleep Apnea" Journal of Clinical Medicine 11, no. 14: 4091. https://doi.org/10.3390/jcm11144091