
Dermoscopic Features of Acute, Subacute, Chronic and Intermittent Subtypes of Cutaneous Lupus Erythematosus in Caucasians


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Acute Cutaneous Lupus Erythematosus (ACLE)
3.2. Subacute Cutaneous Lupus Erythematosus (SCLE)
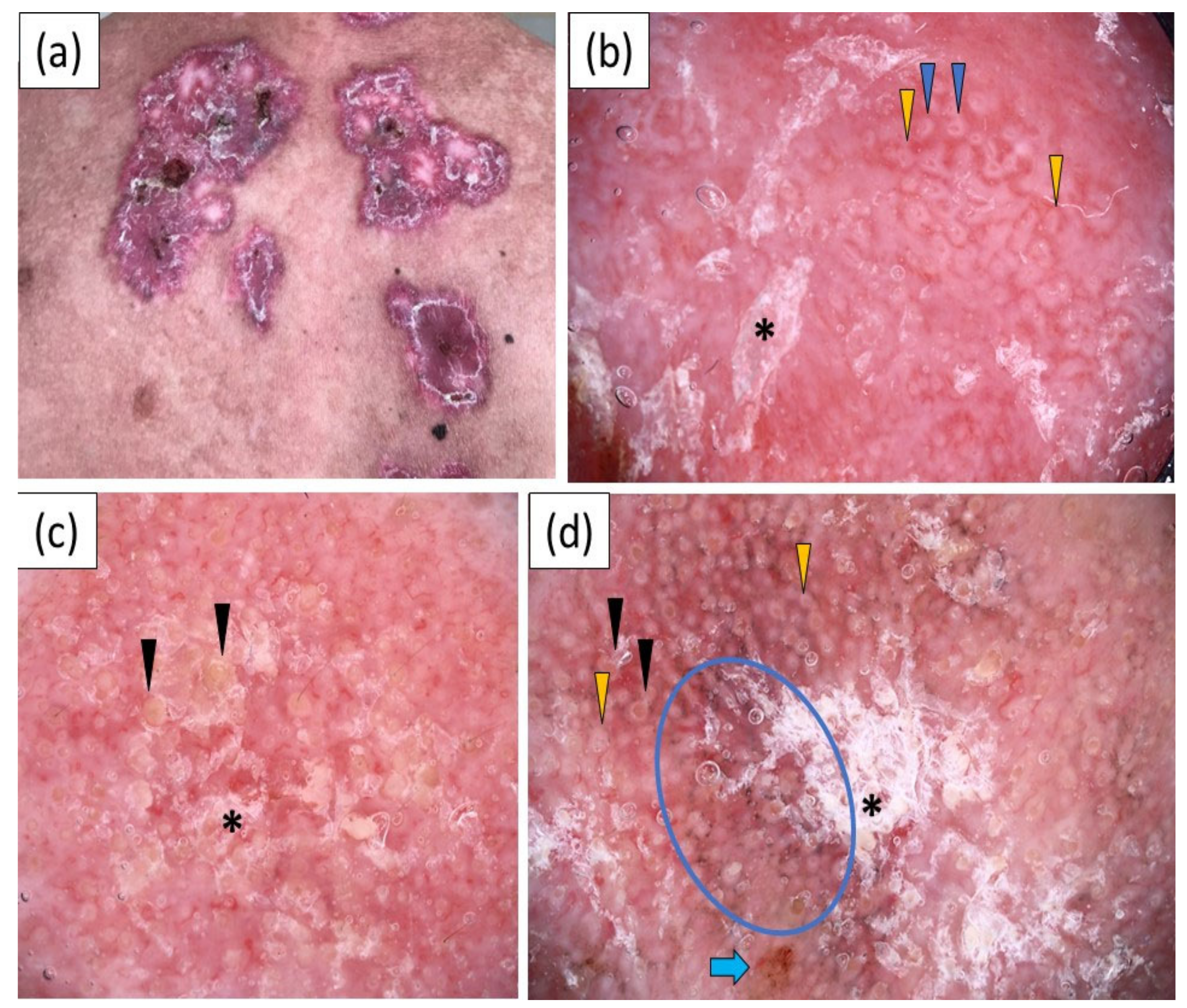
3.3. Chronic Cutaneous Lupus Erythematosus (CCLE)
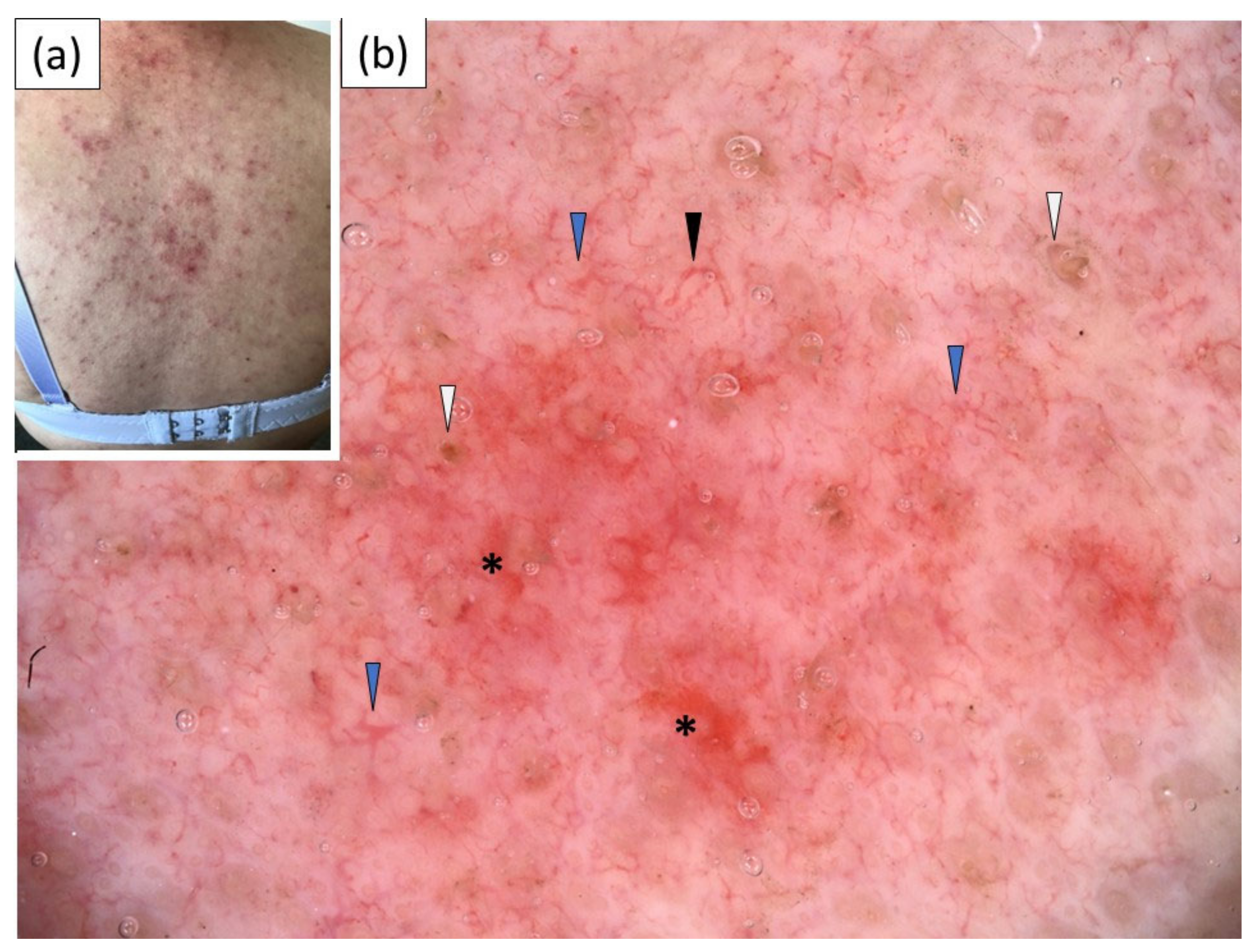
3.4. Intermittent Cutaneous Lupus Erythematosus (ICLE)/Lupus Erythematosus Tumidus (LET)
3.5. Comparison of the Dermoscopic Features of ACLE, SCLE, CCLE and LET
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuhn, A.; Landmann, A. The classification and diagnosis of cutaneous lupus erythematosus. J. Autoimmun. 2014, 48–49, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Patsinakidis, N.; Kautz, O.; Gibbs, B.F.; Raap, U. Lupus erythematosus tumidus: Clinical perspectives. Clin. Cosmet. Investig. Dermatol. 2019, 12, 707–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behera, B.; Palit, A.; Sethy, M.; Nayak, A.K.; Dash, S.; Ayyanar, P. Dermoscopic features of acute cutaneous lupus erythematosus: A retrospective analysis from a tertiary care centre of East India. Australas. J. Dermatol. 2021, 62, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Errichetti, E.; Piccirillo, A.; Viola, L.; Stinco, G. Dermoscopy of subacute cutaneous lupus erythematosus. Int. J. Dermatol. 2016, 55, e605–e607. [Google Scholar] [CrossRef]
- Kim, I.S.; Kim, B.R.; Youn, S.W. Differentiation of Jessner’s lymphocytic infiltration of the skin from various chronic cutaneous lupus erythematosus subtypes by quantitative computer-aided image analysis. Dermatology 2016, 232, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Behera, B.; Kumari, R.; Mohan Thappa, D.; Gochhait, D.; Ayyanar, P. Dermoscopy in the diagnosis of generalized acute cutaneous lupus erythematosus. Int. J. Dermatol. 2021, 60, e306–e308. [Google Scholar] [CrossRef]
- Apalla, Z.; Papadimitriou, I.; Iordanidis, D.; Errichetti, E.; Kyrgidis, A.; Rakowska, A.; Sotiriou, E.; Vakirlis, E.; Bakirtzi, A.; Liopyris, K.; et al. The dermatoscopic spectrum of cutaneous lupus erythematosus: A retrospective analysis by clinical subtype with clinicopathological correlation. Dermatol. Ther. 2020, 33, e14514. [Google Scholar] [CrossRef]
- Fathy, H.; Ghanim, B.M.; Refat, S.; Awad, A. Dermoscopic criteria of discoid lupus erythematosus: An observational cross-sectional study of 28 patients. Indian J. Dermatol. Venereol. Leprol. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Gomez-Quispe, H.; de Las Heras-Alonso, M.E.; Lobato-Berezo, A.; Velasco-Tamariz, V.; Pindado-Ortega, C.; Moreno-Arrones, O.M.; Vañó-Galván, S.; Saceda-Corralo, D. Trichoscopic findings of discoid lupus erythematosus alopecia: A cross-sectional study. J. Am. Acad. Dermatol. 2021, 84, 804–806. [Google Scholar] [CrossRef]
- Karadag Köse, Ö.; Tulin Gulec, A. Evaluation of a handheld dermatoscope in clinical diagnosis of primary cicatricial alopecias. Dermatol. Ther. 2019, 9, 525–535. [Google Scholar] [CrossRef] [Green Version]
- Salah, E. Clinical and dermoscopic spectrum of discoid lupus erythematosus: Novel observations from lips and oral mucosa. Int. J. Dermatol. 2018, 57, 830–836. [Google Scholar] [CrossRef]
- Chiramel, M.J.; Sharma, V.K.; Khandpur, S.; Sreenivas, V. Relevance of trichoscopy in the differential diagnosis of alopecia: A cross-sectional study from North India. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 651–658. [Google Scholar]
- Abedini, R.; Hesari, K.K.; Daneshpazhooh, M.; Ansari, M.S.; Tohidinik, H.R.; Ansari, M. Validity of trichoscopy in the diagnosis of primary cicatricial alopecias. Int. J. Dermatol. 2016, 55, 1106–1114. [Google Scholar] [CrossRef]
- Nikam, V.V.; Mehta, H.H. A nonrandomized study of trichoscopy patterns using nonpolarized (contact) and polarized (noncontact) dermatoscopy in hair and shaft disorders. Int. J. Trichol. 2014, 6, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Qi, A.; Zhao, Y.; Zhang, X.; Li, S.; Cao, H.; Zhang, X. Clinical features of primary cicatricial alopecia in Chinese patients. Indian J. Dermatol. Venereol. Leprol. 2014, 80, 306–312. [Google Scholar]
- Shim, W.H.; Jwa, S.W.; Song, M.; Kim, H.S.; Ko, H.C.; Kim, B.S.; Kim, M.B. Dermoscopic approach to a small round to oval hairless patch on the scalp. Ann. Dermatol. 2014, 26, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Lallas, A.; Argenziano, G.; Apalla, Z.; Gourhant, J.Y.; Zaballos, P.; Di Lernia, V.; Moscarella, E.; Longo, C.; Zalaudek, I. Dermoscopic patterns of common facial inflammatory skin diseases. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 609–614. [Google Scholar] [CrossRef]
- Lallas, A.; Apalla, Z.; Lefaki, I.; Sotiriou, E.; Lazaridou, E.; Ioannides, D.; Tiodorovic-Zivkovic, D.; Sidiropoulos, T.; Konstantinou, D.; di Lernia, V.; et al. Dermoscopy of discoid lupus erythematosus. Br. J. Dermatol. 2013, 168, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Zychowska, M.; Zychowska, M. Dermoscopy of discoid lupus erythematosus—A systematic review of the literature. Int. J. Dermatol. 2021, 60, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Mazzilli, S.; Vollono, L.; Diluvio, L.; Botti, E.; Costanza, G.; Campione, E.; Donati, M.; di Prete, M.; Orlandi, A.; Bianchi, L.; et al. The combined role of clinical, reflectance confocal microscopy and dermoscopy applied to chronic discoid cutaneous lupus and subacute lupus erythematosus: A case series and literature review. Lupus 2021, 30, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Errichetti, E.; Lallas, A.; De Marchi, G.; Apalla, Z.; Zabotti, A.; De Vita, S.; Stinco, G. Dermoscopy in the differential diagnosis between malar rash of systemic lupus erythematosus and erythematotelangiectatic rosacea: An observational study. Lupus 2019, 28, 1583–1588. [Google Scholar] [CrossRef]
- Behera, B.; Nayak, A.K.; Dash, S.; Sethy, M. Subacute cutaneous lupus erythematosus: Diagnosis and follow up by dermoscopy. Indian Dermatol. Online J. 2021, 12, 755–757. [Google Scholar] [CrossRef]
- Behera, B.; Kumari, R.; Gochhait, D.; Ayyanar, P. Dermoscopic appearance of an annular subacute cutaneous lupus erythematosus. Dermatol. Pract. Concept. 2021, 11, e2021013. [Google Scholar] [CrossRef]
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.P.; Ioannides, D.; Lacarrubba, F.; et al. Standarization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2020, 182, 454–467. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | CLE | |||
|---|---|---|---|---|
| ACLE n = 10 | SCLE n = 11 | CCLE n = 26 | LET n = 7 | |
| Gender, n (%) | ||||
| Male | 3 (30.0) | 4 (36.4) | 12 (46.2) | 4 (57.1) |
| Female | 7 (70.0) | 7 (63.6) | 14 (63.8) | 3 (42.9) |
| Age, years | ||||
| Mean ± SD | 50.3 ± 12.2 | 61.4 ± 14.8 | 40.6 ± 14.9 | 49.7 ± 11.9 |
| Median (range) | 53 (34–66) | 64 (42–84) | 38 (15–76) | 49 (29–64) |
| Fitzpatrick skin phototype, n (%) | ||||
| I | 3 (30.0) | 4 (36.4) | 9 (34.6) | 3 (42.9) |
| II | 6 (60.0) | 7 (63.6) | 13 (50.0) | 4 (57.1) |
| III | 1 (10.0) | 0 (0.0) | 4 (15.4) | 0 (0.0) |
| Disease duration, months | ||||
| Mean ± SD | 5.8 ± 3.5 | 5.9 ± 6.9 | 33.2 ±56 | 16.2 ± 20.8 |
| Median (range) | 6 (1–12) | 4 (0.5–24) | 11 (3–216) | 9 (0.5–60) |
| Dermoscopic Characteristics | ACLE n = 10 | SCLE n = 11 | CCLE n = 26 | LET n = 7 | p Value |
|---|---|---|---|---|---|
| Morphology of vessels, n (%) | |||||
| Dotted | 3 (30.0) | 7 (63.6) | 5 (19.2) | 3 (42.9) | 0.07 |
| Linear | 9 (90.0) | 8 (72.7) | 22 (84.6) | 6 (85.7) | 1.00 |
| Linear with branches | 8 (80.0) | 8 (72.7) | 19 (73.1) | 4 (57.1) | 1.00 |
| Thick | 2 (20.0) | 2 (18.2) | 10 (38.5) | 2 (28.6) | 0.55 |
| Thin | 8 (80.0) | 8 (72.7) | 18 (69.2) | 4 (57.1) | 1.00 |
| Linear curved | 7 (70.0) | 8 (72.7) | 21 (80.8) | 4 (57.1) | 1.00 |
| Polymorphous | 10 (100.0) | 9 (81.8) | 21 (80.8) | 7 (100.0) | 1.00 |
| Distribution of vessels, n (%) | |||||
| Uniform | 1 (10.0) | 3 (27.3) | 2 (7.7) | 1 (14.3) | 0.44 |
| Clustered | 0 (0.0) | 1 (9.1) | 0 (0.0) | 0 (0.0) | 0.26 |
| Peripheral | 0 (0.0) | 0 (0.0) | 5 (19.2) | 0 (0.0) | 0.11 |
| Unspecific | 8 (80.0) | 7 (63.6) | 17 (65.4) | 6 (85.7) | 1.00 |
| Color of scales, n (%) | |||||
| White | 3 (30.0) | 7 (63.6) | 20 (76.9) | 0 (0.0) | 1.00 |
| Yellow | 2 (20.0) | 1 (9.1) | 10 (38.5) | 0 (0.0) | 0.09 |
| Distribution of scales, n (%) | |||||
| Diffuse | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0.0) | 0.33 |
| Central | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0.0) | 0.33 |
| Peripheral | 0 (0.0) | 1 (9.1) | 5 (19.2) | 0 (0.0) | 0.27 |
| Patchy | 4 (40.0 | 8 (72.7) | 16 (61.5) | 0 (0.0) | 1.00 |
| Follicular findings, n (%) | |||||
| Rosettes | 0 (0.0) | 0 (0.0) | 8 (30.8) | 0 (0.0) | 0.02 |
| Follicular plugs | 2 (20.0) | 2 (18.2) | 18 (69.2) | 3 (42.9) | 0.01 |
| Follicular red dots | 0 (0.0) | 0 (0.0) | 10 (38.5) | 0 (0.0) | <0.01 |
| Perifollicular white halo | 0 (0.0) | 0 (0.0) | 14 (53.8) | 0 (0.0) | <0.01 |
| Perifollicular pigmentation | 0 (0.0) | 0 (0.0) | 5 (19.2) | 0 (0.0) | 0.11 |
| Perifollicular scaling | 1 (10.0) | 0 (0.0) | 6 (23.1) | 0 (0.0) | 0.16 |
| Morphologies/colors, n (%) | |||||
| White structureless areas | 1 (10.0) | 0 (0.0) | 12 (46.2) | 1 (14.3) | 0.01 |
| Pink structureless areas | 0 (0.0) | 1 (9.1) | 13 (50.0) | 0 (0.0) | <0.01 |
| Yellow structureless areas | 1 (10.0) | 0 (0.0) | 5 (19.2) | 0 (0.0) | 0.26 |
| Dots/globules | 5 (50.0) | 3 (27.3) | 14 (53.8) | 1 (14.3) | 0.18 |
| Red globules | 2 (20.0) | 0 (0.0) | 5 (19.2) | 1 (14.3) | 0.14 |
| Gray–brown dots | 1 (10.0) | 2 (18.2) | 10 (38.5) | 0 (0.0) | 0.09 |
| Gray–brown globules | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0.0) | 0.33 |
| White–yellowish globules | 0 (0.0) | 1 (9.1) | 1 (3.8) | 1 (14.3) | 0.57 |
| White Lines | 0 (0.0) | 0 (0.0) | 2 (7.7) | 0 (0.0) | 0.54 |
| Specific clues, n (%) | |||||
| Peripheral pigmentation | 2 (20.0) | 5 (45.5) | 10 (38.5) | 0 (0.0) | 0.14 |
| Yellowish crust | 1 (10.0) | 2 (18.2) | 6 (23.1) | 0 (0.0) | 0.47 |
| Erosion | 1 (10.0) | 2 (18.2) | 10 (38.5) | 0 (0.0) | 0.10 |
| “sticky fiber” sign | 1 (10.0) | 1 (9.1) | 1 (3.8) | 0 (0.0) | 0.76 |
| Pink–red background | 10 (100.0) | 10 (90.9) | 18 (69.2) | 6 (85.7) | 1.00 |
| Dilated follicles | 3 (30.0) | 3 (27.3) | 10 (38.5) | 1 (14.7) | 0.65 |
| Red hemorrhagic areas | 5 (50.0) | 4 (36.4) | 13 (50.0) | 2 (28.6) | 0.69 |
| Comedo-like openings | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0.0) | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żychowska, M.; Reich, A. Dermoscopic Features of Acute, Subacute, Chronic and Intermittent Subtypes of Cutaneous Lupus Erythematosus in Caucasians. J. Clin. Med. 2022, 11, 4088. https://doi.org/10.3390/jcm11144088
Żychowska M, Reich A. Dermoscopic Features of Acute, Subacute, Chronic and Intermittent Subtypes of Cutaneous Lupus Erythematosus in Caucasians. Journal of Clinical Medicine. 2022; 11(14):4088. https://doi.org/10.3390/jcm11144088
Chicago/Turabian StyleŻychowska, Magdalena, and Adam Reich. 2022. "Dermoscopic Features of Acute, Subacute, Chronic and Intermittent Subtypes of Cutaneous Lupus Erythematosus in Caucasians" Journal of Clinical Medicine 11, no. 14: 4088. https://doi.org/10.3390/jcm11144088