
Sleeve Gastrectomy-Induced Body Mass Index Reduction Increases the Intensity of Taste Perception’s and Reduces Bitter-Induced Pleasantness in Severe Obesity

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Basic Tastes Testing
2.3. Data Analysis
3. Results
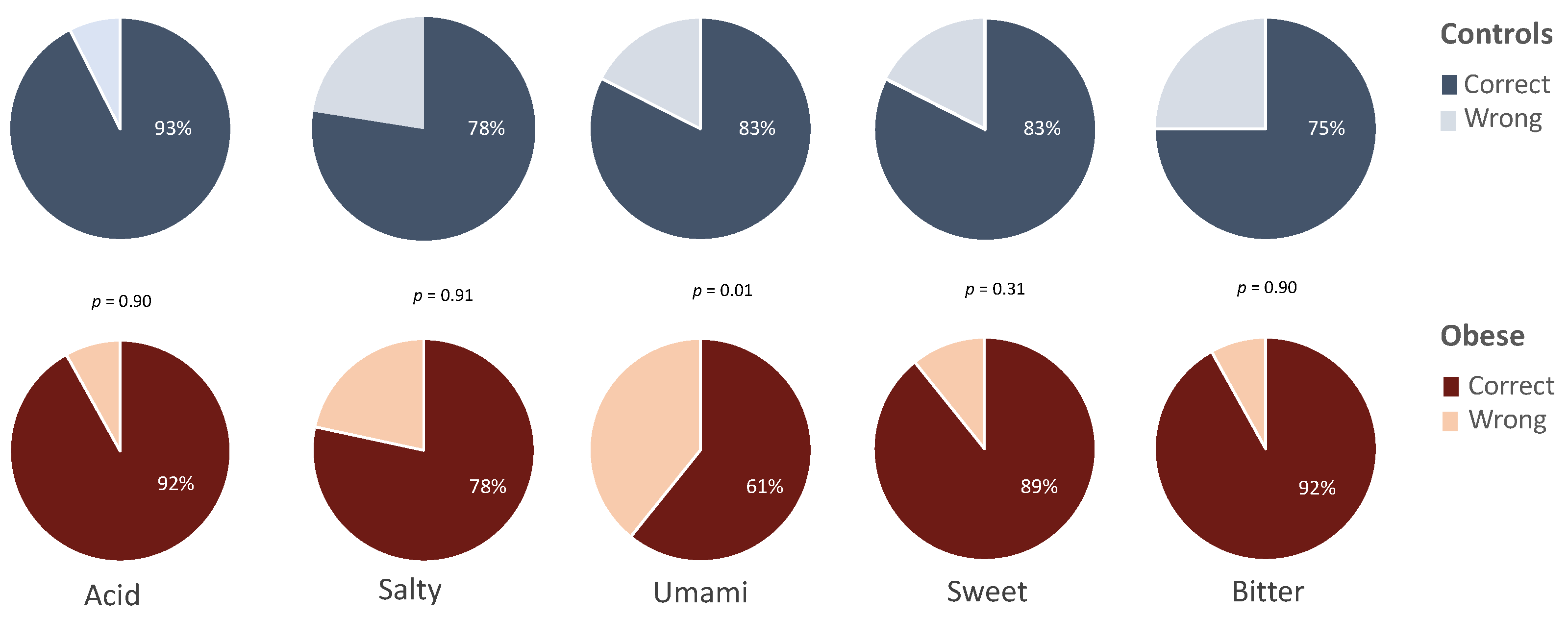
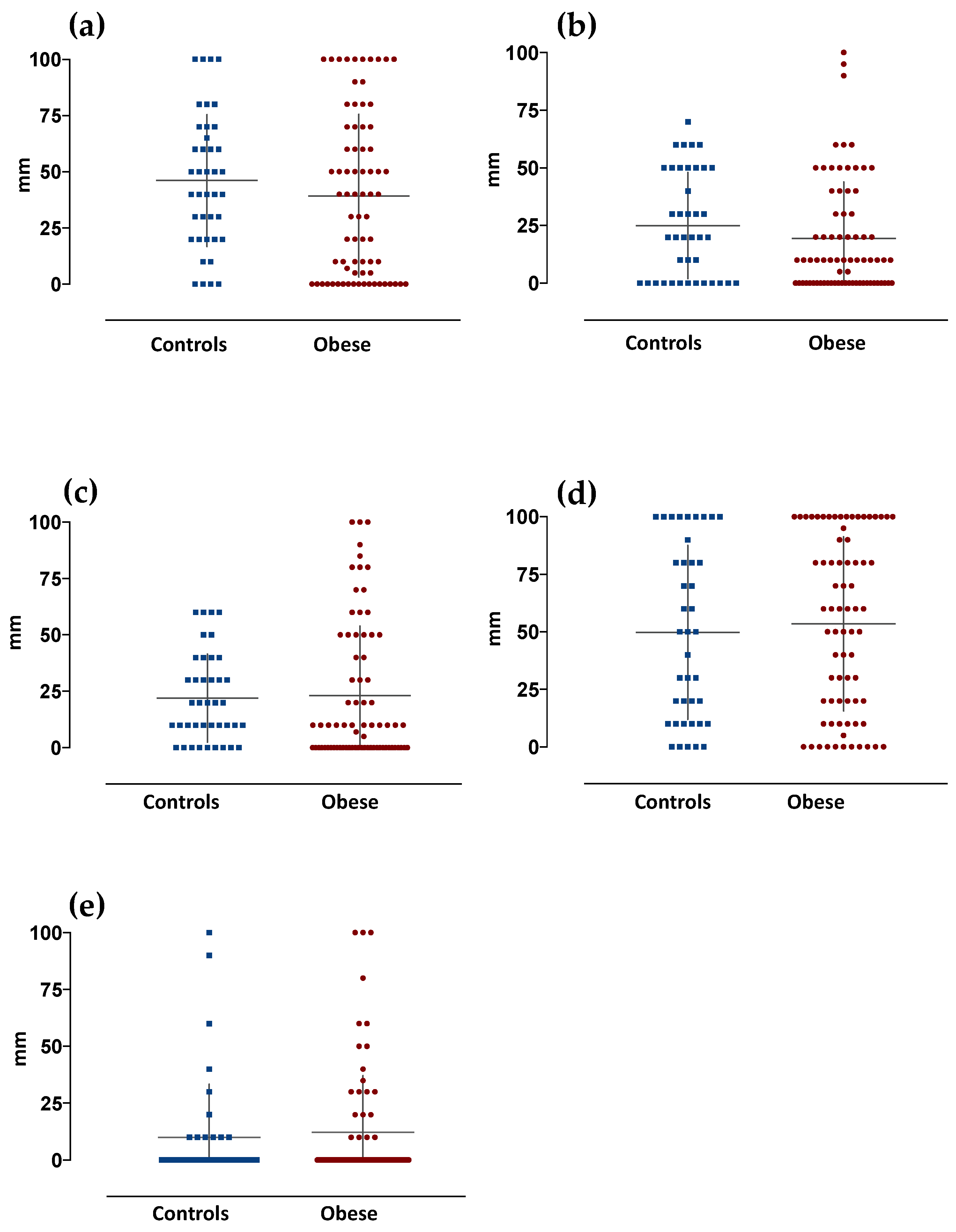
3.1. Basic Tastes Identification, Relative Intensity and Pleasantness-Induced Perception in Control and Obese Subjects
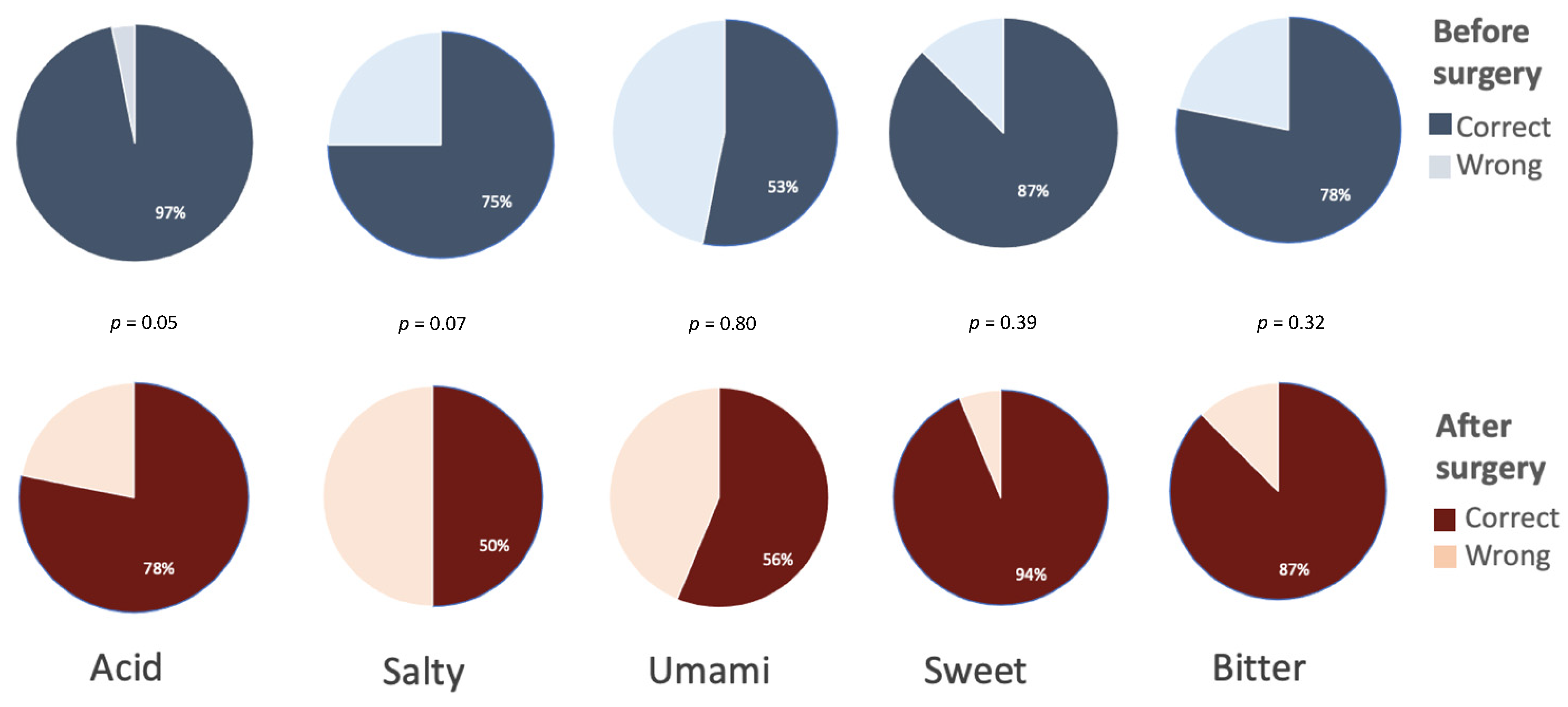
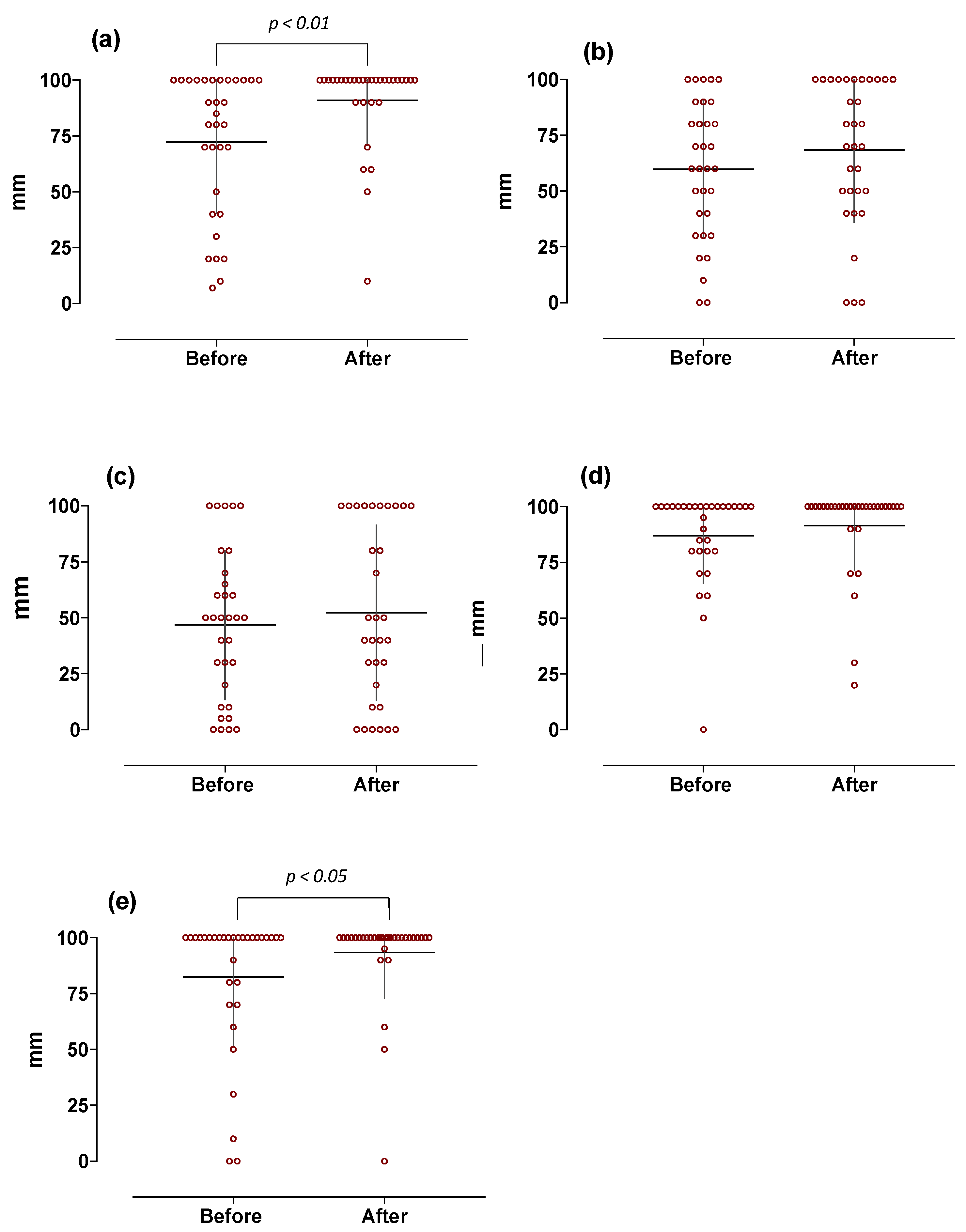
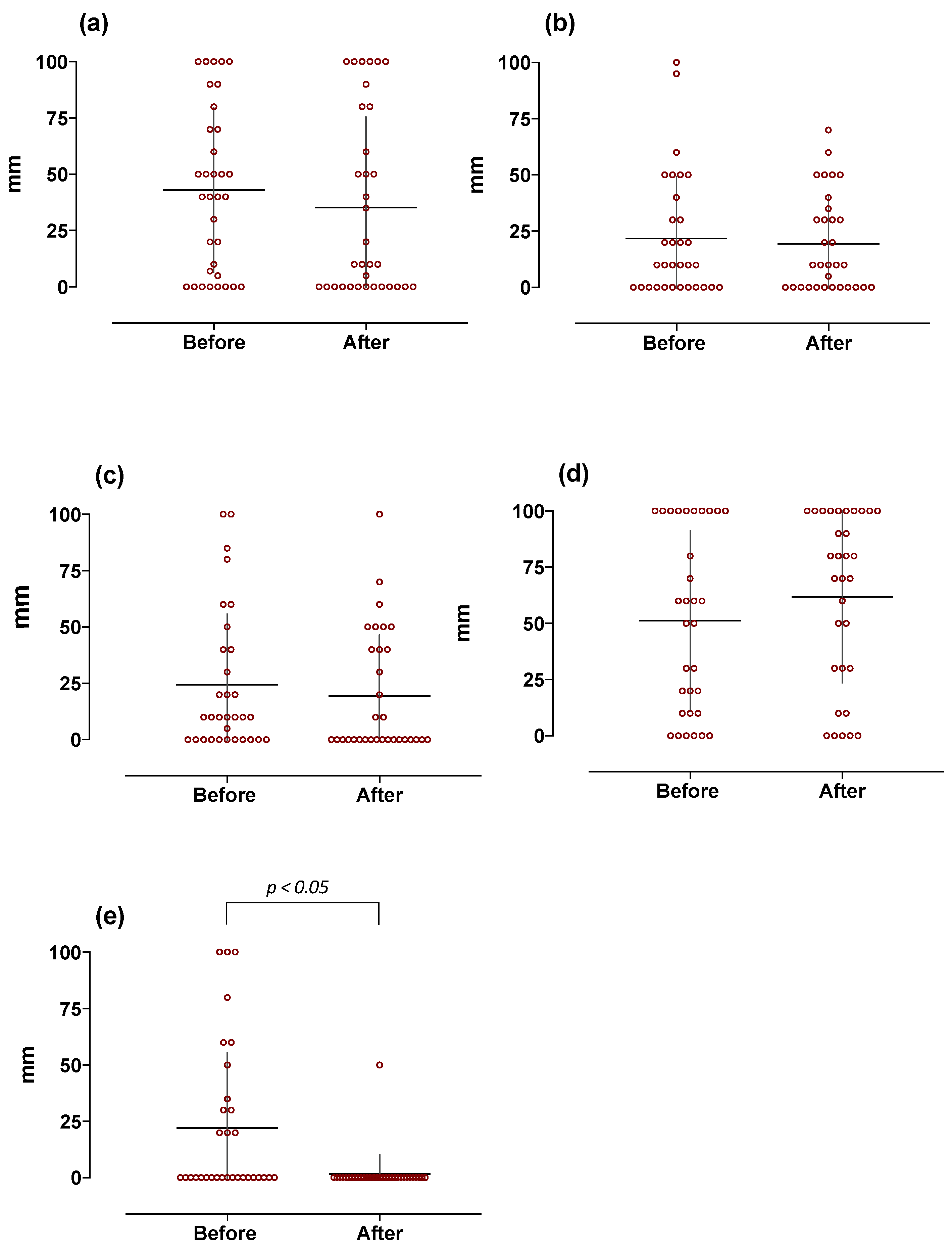
3.2. Weight-Loss Induced Basic Tastes Identification, Relative Intensity and Pleasantness-Induced Perception in Obese Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Jaacks, L.M.; Vandevijvere, S.; Pan, A.; McGowan, C.J.; Wallace, C.; Imamura, F.; Mozaffarian, D.; Swinburn, B.; Ezzati, M. The obesity transition: Stages of the global epidemic. Lancet Diabetes Endocrinol. 2019, 7, 231–240. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Furth, S.; Zoccali, C. Obesity and kidney disease: Hidden consequences of the epidemic. Braz. J. Nephrol. 2017, 14, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthoud, H.-R.; Zheng, H. Modulation of taste responsiveness and food preference by obesity and weight loss. Physiol. Behav. 2012, 107, 527–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrandies, W.; Zschieschang, R. Olfactory and gustatory functions and its relation to body weight. Physiol. Behav. 2015, 142, 1–4. [Google Scholar] [CrossRef]
- Kure Liu, C.; Joseph, P.V.; Feldman, D.E.; Kroll, D.S.; Burns, J.A.; Manza, P.; Volkow, N.D.; Wang, G.J. Brain Imaging of Taste Perception in Obesity: A Review. Curr. Nutr. Rep. 2019, 8, 108–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarnelli, G.; Annunziata, G.; Magno, S.; Oriolo, C.; Savastano, S.; Colao, A. Taste and the Gastrointestinal tract: From physiology to potential therapeutic target for obesity. Int. J. Obes. Suppl. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Roper, S.D.; Chaudhari, N. Taste buds: Cells, signals and synapses. Nat. Rev. Neurosci. 2017, 18, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Di Salle, F.; Cantone, E.; Savarese, M.F.; Aragri, A.; Prinster, A.; Nicolai, E.; Sarnelli, G.; Iengo, M.; Buyckx, M.; Cuomo, R. Effect of Carbonation on Brain Processing of Sweet Stimuli in Humans. Gastroenterology 2013, 145, 537–539.e3. [Google Scholar] [CrossRef] [PubMed]
- Prinster, A.; Cantone, E.; Verlezza, V.; Magliulo, M.; Sarnelli, G.; Iengo, M.; Cuomo, R.; Di Salle, F.; Esposito, F. Cortical representation of different taste modalities on the gustatory cortex: A pilot study. PLoS ONE 2017, 12, e0190164. [Google Scholar] [CrossRef] [Green Version]
- Latorre, R.; Huynh, J.; Mazzoni, M.; Gupta, A.; Bonora, E.; Clavenzani, P.; Chang, L.; Mayer, E.A.; de Giorgio, R.; Sternini, C. Expression of the Bitter Taste Receptor, T2R38, in Enteroendocrine Cells of the Colonic Mucosa of Overweight/Obese vs. Lean Subjects. PLoS ONE 2016, 11, e0147468. [Google Scholar] [CrossRef] [PubMed]
- Al-Alsheikh, A.S.; Alabdulkader, S.; Johnson, B.; Goldstone, A.P.; Miras, A.D. Effect of Obesity Surgery on Taste. Nutrients 2022, 14, 866. [Google Scholar] [CrossRef] [PubMed]
- Umabiki, M.; Tsuzaki, K.; Kotani, K.; Nagai, N.; Sano, Y.; Matsuoka, Y.; Kitaoka, K.; Okami, Y.; Sakane, N.; Higashi, A. The Improvement of Sweet Taste Sensitivity with Decrease in Serum Leptin Levels during Weight Loss in Obese Females. Tohoku J. Exp. Med. 2010, 220, 267–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miras, A.D.; Jackson, R.N.; Jackson, S.N.; Goldstone, A.P.; Olbers, T.; Hackenberg, T.; Spector, A.C.; le Roux, C.W. Gastric bypass surgery for obesity decreases the reward value of a sweet-fat stimulus as assessed in a progressive ratio task. Am. J. Clin. Nutr. 2012, 96, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Sauer, H.; Ohla, K.; Dammann, D.; Teufel, M.; Zipfel, S.; Enck, P.; Mack, I. Changes in Gustatory Function and Taste Preference following Weight Loss. J. Pediatr. 2017, 182, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Gero, D.; Dib, F.; Ribeiro-Parenti, L.; Arapis, K.; Chosidow, D.; Marmuse, J.-P. Desire for Core Tastes Decreases after Sleeve Gastrectomy: A Single-Center Longitudinal Observational Study with 6-Month Follow-up. Obes. Surg. 2017, 27, 2919–2926. [Google Scholar] [CrossRef]
- Le Roux, C.W.; Heneghan, H.M. Bariatric Surgery for Obesity. Med. Clin. N. Am. 2018, 102, 165–182. [Google Scholar] [CrossRef]
- De Luca, M.; Angrisani, L.; Himpens, J.; Busetto, L.; Scopinaro, N.; Weiner, R.; Sartori, A.; Stier, C.; Lakdawala, M.; Bhasker, A.G.; et al. Indications for surgery for obe-sity and weight-related diseases: Position statements from the International Federation for the Surgery of Obesi-ty and Metabolic Disorders (IFSO). Obes. Surg. 2016, 26, 1659–1696. [Google Scholar] [CrossRef]
- Shoar, S.; Naderan, M.; Shoar, N.; Modukuru, V.R.; Mahmoodzadeh, H. Alteration Pattern of Taste Perception after Bariatric Surgery: A Systematic Review of Four Taste Domains. Obes. Surg. 2019, 29, 1542–1550. [Google Scholar] [CrossRef]
- Altun, H.; Hanci, D.; Altun, H.; Batman, B.; Serin, R.K.; Karip, A.B.; Akyuz, U. Improved Gustatory Sensitivity in Mor-bidly Obese Patients after Laparoscopic Sleeve Gastrectomy. Ann. Otol. Rhinol. Laryngol. 2016, 125, 536–540. [Google Scholar] [CrossRef]
- Kapoor, N.; Al-Najim, W.; Le Roux, C.W.; Docherty, N.G. Shifts in Food Preferences after Bariatric Surgery: Observational Reports and Proposed Mechanisms. Curr. Obes. Rep. 2017, 6, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Rohde, K.; Schamarek, I.; Blüher, M. Consequences of Obesity on the Sense of Taste: Taste Buds as Treatment Targets? Diabetes Metab. J. 2020, 44, 509–528. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Mohebbi, M.; Unrath, M.; Hummel, C.; Hummel, T. Different Neural Processing of Umami and Salty Taste Determined by Umami Identification Ability Independent of Repeated Umami Exposure. Neuroscience 2018, 383, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Hong, G.; Matsuyama, Y.; Wang, W.; Izumi, S.; Izumi, M.; Toda, T.; Kudo, T.A. Association of Oral Fat Sensitivity with Body Mass Index, Taste Preference, and Eating Habits in Healthy Japanese Young Adults. Tohoku J. Exp. Med. 2016, 238, 93–103. [Google Scholar] [CrossRef] [Green Version]
- Pepino, M.Y.; Finkbeiner, S.; Beauchamp, G.K.; Mennella, J.A. Obese Women Have Lower Monosodium Glutamate Taste Sensitivity and Prefer Higher Concentrations Than Do Normal-weight Women. Obesity 2010, 18, 959–965. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, G.K. Sensory and receptor responses to umami: An overview of pioneering work. Am. J. Clin. Nutr. 2009, 90, 723S–727S. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, K.; Penney, N.; Darzi, A.; Purkayastha, S. Taste Changes after Bariatric Surgery: A Systematic Review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [Green Version]
- Schiavo, L.; Aliberti, S.M.; Calabrese, P.; Senatore, A.M.; Severino, L.; Sarno, G.; Iannelli, A.; Pilone, V. Changes in Food Choice, Taste, Desire, and Enjoyment 1 Year after Sleeve Gastrectomy: A Prospective Study. Nutrients 2022, 14, 2060. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; Al-Qahtani, F.S.; Zamakhshary, M.; BinDhim, N.F. Food Taste, Dietary Consumption, and Food Preference Perception of Changes following Bariatric Surgery in the Saudi Population: A Cross-Sectional Study. Nutrients 2021, 13, 3401. [Google Scholar] [CrossRef]
- Berro, C.; Pendolino, A.L.; Foletto, M.; Facciolo, M.C.; Maculan, P.; Prevedello, L.; Giuntoli, D.G.; Scarpa, B.; Pavan, C.; Andrews, P.J.; et al. Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy. Medicina 2021, 57, 913. [Google Scholar] [CrossRef]
- Koh, G.Y.; Rowling, M.J.; Pritchard, S.K. Possible role of type 1 and type 2 taste receptors on obesity-induced inflammation. Nutr. Rev. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, A.; Choo, E.; Koh, A.; Dando, R. Inflammation arising from obesity reduces taste bud abundance and inhibits renewal. PLoS Biol. 2018, 16, e2001959. [Google Scholar] [CrossRef] [Green Version]
- Vignini, A.; Borroni, F.; Sabbatinelli, J.; Pugnaloni, S.; Alia, S.; Taus, M.; Ferrante, L.; Mazzanti, L.; Fabri, M. General Decrease of Taste Sensitivity Is Related to Increase of BMI: A Simple Method to Monitor Eating Behavior. Dis. Markers 2019, 2019, 2978026. [Google Scholar] [CrossRef] [Green Version]
- Karmous, I.; Plesník, J.; Khan, A.S.; Šerý, O.; Abid, A.; Mankai, A.; Aouidet, A.; Khan, N.A. Orosensory detection of bitter in fat-taster healthy and obese participants: Genetic polymorphism of CD36 and TAS2R38. Clin. Nutr. 2017, 37, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, P.; Sarnelli, G.; Pesce, M.; Zito, F.P.; Alessandro, A.D.; Verlezza, V.; Palumbo, I.; Turco, F.; Esposito, K.; Cuomo, R. The Bitter Taste Receptor Agonist Quinine Reduces Calorie Intake and Increases the Postprandial Release of Cholecystokinin in Healthy Subjects. J. Neurogastroenterol. Motil. 2015, 21, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, G.; Camacho, M.; Fernandes, A.B.; Cotovio, G.; Torres, S.; Oliveira-Maia, A.J. Reward-related gustatory and psychometric predictors of weight loss following bariatric surgery: A multicenter cohort study. Am. J. Clin. Nutr. 2021, 113, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Monteleone, P.; Esposito, F.; Prinster, A.; Volpe, U.; Cantone, E.; Pellegrino, F.; Canna, A.; Milano, W.; Aiello, M.; et al. Altered processing of rewarding and aversive basic taste stimuli in symptomatic women with anorexia nervosa and bulimia nervosa: An fMRI study. J. Psychiatr. Res. 2017, 90, 94–101. [Google Scholar] [CrossRef]
- Wilkie, L.M.; Phillips, E.D.C. Heterogeneous binary interactions of taste primaries: Perceptual outcomes, physiology, and future directions. Neurosci. Biobehav. Rev. 2014, 47, 70–86. [Google Scholar] [CrossRef]
- Walters, D.E. How are bitter and sweet tastes related? Trends Food Sci. Technol. 1996, 7, 399–403. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population (n) | Gender (M/F) | Age (Years) | BMI (kg/m2) |
|---|---|---|---|
| Controls (40) | 14/26 | 30 ± 11 | 23 ± 3 |
| Obese (74) | 30/44 | 37 ± 11 | 46 ± 7.4 * |
| Sour | Salty | Umami | Sweet | Bitter | |
|---|---|---|---|---|---|
| Controls (40) | 80 ± 16 | 60 ± 24 | 50 ± 24 | 83 ± 24 | 90 ± 17 |
| Obese (74) | 78 ± 28 | 64 ± 31 | 51 ± 34 | 83 ± 22 | 87 ± 25 |
| p | 0.65 | 0.38 | 0.78 | 0.87 | 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rurgo, S.; Cantone, E.; Pesce, M.; Efficie, E.; Musella, M.; Polese, B.; De Conno, B.; Pagliaro, M.; Seguella, L.; Guida, B.; et al. Sleeve Gastrectomy-Induced Body Mass Index Reduction Increases the Intensity of Taste Perception’s and Reduces Bitter-Induced Pleasantness in Severe Obesity. J. Clin. Med. 2022, 11, 3957. https://doi.org/10.3390/jcm11143957
Rurgo S, Cantone E, Pesce M, Efficie E, Musella M, Polese B, De Conno B, Pagliaro M, Seguella L, Guida B, et al. Sleeve Gastrectomy-Induced Body Mass Index Reduction Increases the Intensity of Taste Perception’s and Reduces Bitter-Induced Pleasantness in Severe Obesity. Journal of Clinical Medicine. 2022; 11(14):3957. https://doi.org/10.3390/jcm11143957
Chicago/Turabian StyleRurgo, Sara, Elena Cantone, Marcella Pesce, Eleonora Efficie, Mario Musella, Barbara Polese, Barbara De Conno, Marta Pagliaro, Luisa Seguella, Bruna Guida, and et al. 2022. "Sleeve Gastrectomy-Induced Body Mass Index Reduction Increases the Intensity of Taste Perception’s and Reduces Bitter-Induced Pleasantness in Severe Obesity" Journal of Clinical Medicine 11, no. 14: 3957. https://doi.org/10.3390/jcm11143957