1. Introduction
Epiretinal membranes (ERMs) develop above the internal limiting membrane (ILM) of the retina and represent a relatively common macular finding. Their appearance varies widely from patient to patient, ranging from a translucent wrinkling of the inner retinal surface, all the way to an extensive, thick, epiretinal cellular proliferation [
1].
The retinal surgeon benefits greatly from a precise preoperative view of the ERM, which is made possible by continuous advancements in imaging technology.
Thanks to its high-definition cross-sectional scans, optical coherence tomography (OCT) has revolutionized the diagnostic visualization of ERMs [
2]. Other common imaging techniques such as fundus autofluorescence (FAF) and enface OCT technology have also been shown to be effective at visualizing ERMs and, in some cases, even at predicting certain post-operative outcomes [
3].
The novel retromode imaging (RMI) is a noncontact and a noninvasive imaging method that relies on the newly introduced confocal scanning laser ophthalmoscopic technology. Briefly, there are two kinds of light returning back from the fundus once it is illuminated, a direct reflex and a scattered light. Retromode imaging uses a laterally deviated confocal aperture with a central stop to block the direct light reflex and to collect the backscattered light from one direction [
4]. This enables the formation of pseudo-3D images, through the creation of a shadow to one side of the abnormal feature that is being investigated, which eventually enhances the contrast of the lesion. Knowing the ability of infrared lasers to penetrate deeper retinal layers, retromode imaging with infrared laser-technology has been used to evaluate retinal pathological changes in several retinal and choroidal diseases [
5].
RMI is performed by a scanning laser ophthalmoscope (SLO) working at an infrared wavelength, which creates a pseudo three-dimensional image with highly contrasting margins of retinal abnormalities (e.g., neurosensory detachments, retinal holes, retinoschisis and intraretinal cystic fluid) [
6]. However, to the best of our knowledge, there are no reports describing the retromode imaging of ERMs.
The main outcome of this study was to evaluate morphological features, such as the area of retinal folds and the area of intraretinal cystic spaces, in eyes with ERM. This was achieved by cropping and overlapping images of the ERMs using noninvasive retromode imaging and comparing these to color fundus images. Moreover, we examined the correlation between retromode findings and fundus autofluorescence (FAF).
2. Materials and Methods
The study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee (protocol ID number 3680/20). Written informed consent for participation to the research was obtained from the patients after explanation of the purpose and the process of the study.
We performed a monocentric prospective case-series study enrolling patients with an ERM who attended the ophthalmology unit at the Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy, from 1 January–1 July 2021.
A comprehensive ocular examination, including measurements of the refractive error (spherical equivalent) and the best correct visual acuity, and a dilated macular examination (through indirect ophthalmoscopy) were performed on the day of enrollment. Patients then received a thorough posterior pole investigation through various imaging techniques (i.e., RMI, FAF, color fundus photography and OCT B-scanning). All scans were performed using the Mirante SLO/OCT (Nidek Co, Gamagori, Japan), providing an image field of 40 degrees, an optical resolution of 16 to 20 μm and an image size of up to 1024 × 720 pixels. Inclusion criteria were the presence of an epiretinal membrane confirmed via OCT-B scans with no other concomitant intraocular disease. Eyes with a history of ocular trauma, previous intraocular surgery (with the exception of cataract surgery) or any abnormal intraocular findings (i.e., diabetic retinopathy, neovascular age-related macular degeneration, retinal angiomatous proliferation, angioid streaks, pathological myopia, retinal detachment), were excluded from the study. Images with poor quality due to severe cataracts or unstable fixation were also a reason for exclusion.
After the examinations were performed (1–6 months), all included patients underwent surgery for peeling of the ERM. This was performed by two expert vitreo-retinal surgeons, using 23- or 25-gauge pars plana vitrectomy (PPV) (Constellation Vision System, Alcon, Fort Worth, TX, USA) according to the surgeon’s choice, as already described by Savastano et al. [
7].
2.1. Images Detection
After completing OCT scans of the entire area within the vascular arcades, the fundus was investigated using fundus photography, FAF and retromode imaging. The OCT acquisition protocol consisted of a 6 × 6 mm (mm) three-dimensional vertical scanning area, centered on the fovea comprising 512 × 128 scans. Color photos from Nidek Mirante had a 45-degree field of view with a resolution of 1024 × 720 pixels. Three separate laser wavelengths (red—670 nm, green—532 nm, blue—488 nm) are combined to create color pictures, which are then connected to a specific sensor for each wavelength. A blue-light excitation wavelength of 488 nm (emission > 500 nm) is used to obtain fundus autofluorescence (FAF), whereas the retromode imaging system uses an infrared laser light (790 nm). A right-deviated aperture and a left-deviated aperture were used to obtain two separate retromode pictures per eye. All the tomographic images were acquired, averaging up to 30 frames per image.
2.2. Data Analysis
Image processing was performed using the ImageJ software (National Institutes of Health, MD, USA).
Fundus Autofluorescence, retromode and fundus photography images were cropped and superimposed to have topographic correspondence, and the surface area of each image was measured in square mm2.
All images were reviewed separately by two authors to identify, record and interpret the various morphologic alterations associated with ERM. In case of disagreement between the two, a third expert would choose which of the measurements was more accurate.
All images were exported as high-quality tiff files and were collected using the REDCap platform (Vanderbilt University), a secure web application for building and managing online surveys and databases [
8].
We matched retromode images with color fundus photographs, FAF images and OCT B-scans using various reference points.
The optic nerve’s superior and inferior margins and retinal blood vessels on color fundus photography (blue lines and orange lines, respectively) were matched with their counterparts identified on retromode images, as shown in
Figure 1. On the other hand, while FAF images were matched to retromode images using the retinal blood vessels alone (orange lines
Figure 2), for OCT B-scans we used both the neuroretinal rim (grey lines) and the extension of the ERM itself. Particularly, the ERM margins on OCT images were projected onto the retromode image through
orange lines, whereas black lines parallel to those originating from the neuroretinal rim were used to project the cystic spaces identified on OCT B-scans to their retromode counterparts (
Figure 3).
2.3. Statistical Analysis
All statistical analyses were performed using SPSS version 27 (IBM-SPSS, Chicago, IL, USA). Quantitative variables were expressed as mean and standard deviation (SD), whereas qualitative variables were displayed as percentages. According to the normality test results, the Student’s
t-test was used to compare the independent and paired samples. Pearson’s chi-squared test was used to analyze the distribution of the areas of retinal folds among the different multimodal imaging techniques. For each imaging modality, interobserver agreement was calculated using a kappa statistic [
9]. The interobserver agreement between the two examiners was not inferior to 0.93 for each comparison. A
p value of less than 0.5 was considered statistically significant.
3. Results
Twenty-one eyes (21 patients) with an epiretinal membrane were included. Twelve patients (57.1%) were male, nine (42.9%) were female and the mean age was 68.38 ± 7.89 years with a range of 51 to 83 years. Snellen best-corrected visual acuity (BCVA) ranged from 20/320 to 20/25.
The mean area of retinal folds in the FAF images was 5.67 ± 2.15 mm
2 (range 3.12–11.02 mm
2), whereas those in the fundus photographs and RMI were 10.58 ± 3.45 mm
2 (range 5.24–15.62 mm
2) and 11.85 ± 3.91 mm
2 (range 19.98–11.85 mm
2), respectively (
Table 1).
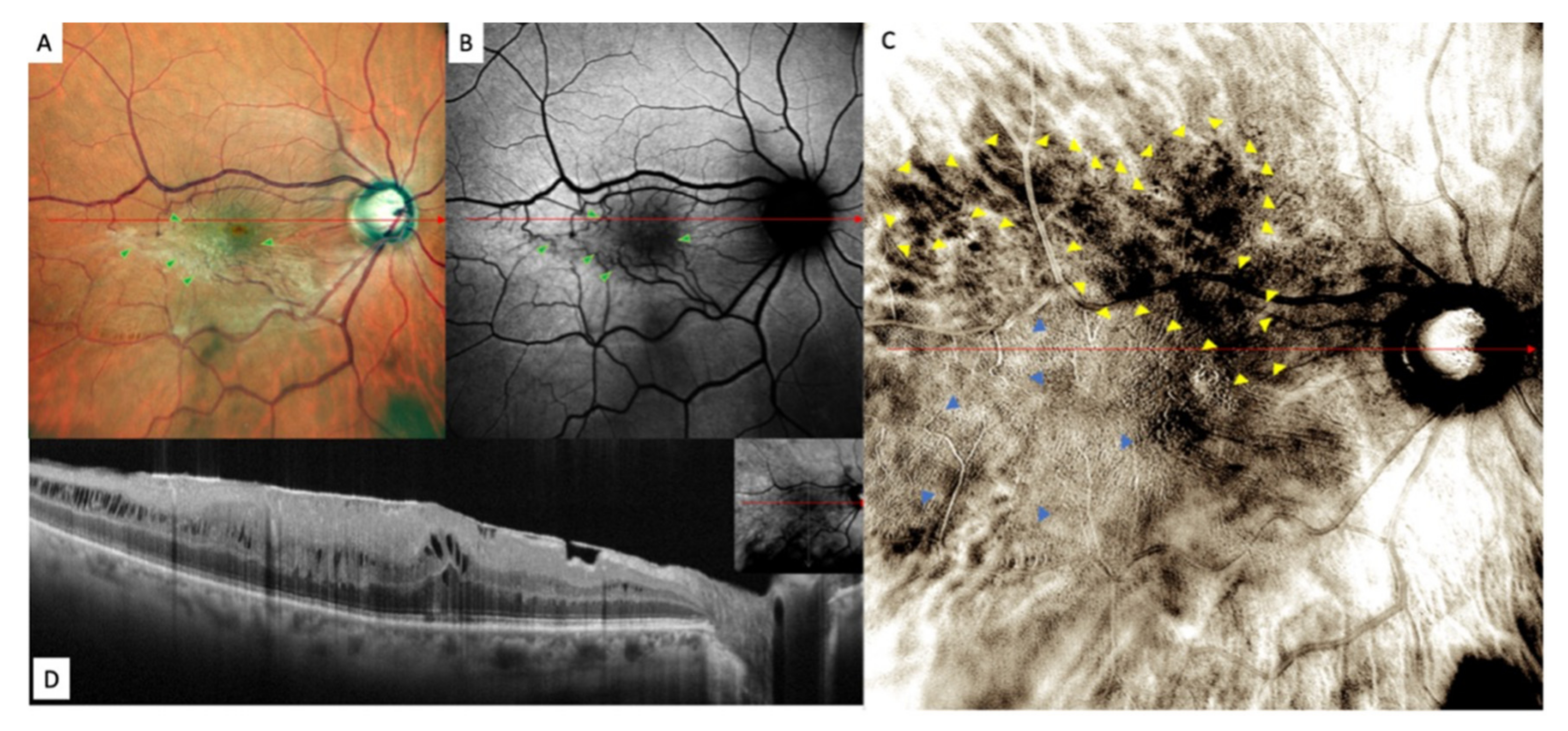
Retromode images demonstrated areas of increased reflectance with fingerprint patterns containing radiating retinal striae centered on the fovea (blue arrowheads), along with areas of decreased reflectance with more prominent large choroidal vessels in the pericentral area (dark choroid aspect observed in 5 of 21 eyes) (multiple yellow arrowheads) (
Figure 4).
The areas of increased reflectance, with fingerprint patterns containing radiating retinal striae centered on the fovea in RMI and the retinal folds in the FAF and fundus photography, are displayed in
Figure 5.
FAF images showed an irregular-shaped area of hypo autofluorescence with distorted retinal vessels (green arrowheads). This area corresponded to the extent of the ERM (
Figure 4).
Fundus photography, on the other hand, displayed the epiretinal proliferation as a whitish reflex and evident retinal folds in the macular area that were strictly related to distorted retinal vessels in the FAF images and to fingerprint appearance in the retromode images.
Overall, the lesions in the retromode images seemed more extensive than those in the FAF images. However, retromode imaging showed numerous ovoidal or polygonal cystoid spaces located in only two eyes. Both displayed a large cystoid space beneath the fovea and surrounding small cystic spaces for OCT, and the wider the area of exudation was for RMI, the higher the retinal profile was for optical coherence tomography (OCT).
While examining ERM’s pathological findings themselves, in this study we also aimed at investigating the correspondence between retromode images and color fundus photographs. Particularly, we analyzed ERM patterns such as the cystic area (in both retromode and horizontal B-scan images) and the area of retinal folding (on FAF, fundus photograph, retromode, horizontal B-scan). The comparison between the different imaging modalities in the 21 enrolled eyes is shown in
Table 2.
There were significant differences between FAF and retro-mode imaging in the detection of retinal folds (i.e., macular traction) (p < 0.05).
The mean area of retinal folds detected by RMI was significantly higher than that detected by FAF (11.85 ± 3.92 mm2 and 5.67 ± 2.15 mm2, respectively, p < 0.05), similar to that detected by fundus photography (11.85 ± 3.92 mm2 and 10.58 ± 3.45 mm2, respectively, p = 0.277).
Pearson’s correlation test revealed a positive correlation between the areas of retinal folds detected by RMI and those detected by fundus photographs, FAF and OCT (r = −0.90, p < 0.001, r = −0.63, p < 0.001, r = −0.35, p = 0.003, respectively).
4. Discussion
In this study we evaluated the pathological findings related to ERMs using and comparing three imaging techniques: retromode imaging, color fundus photography and fundus autofluorescence.
Thanks to its innovative features, retromode imaging could ease the identification of some ERM features, such as the retinal folds, vessel traction and cystic area, compared to other imaging modalities [
4]. The matching between the SD-OCT scans and retromode images of ERMs using pixel-drawing software (ImageJ) has already been described [
10]. Indeed, the pseudo-3D effect obtained by filtering the infrared light through a laterally deviated confocal aperture with a central stop creates a directional shadow according to the laterality of the annular aperture and is very effective at detecting retinal folds [
4].
Among the classic imaging modalities able to document structural changes caused by ERMs, fundus photography is very useful, as this is a fast, noninvasive and easy test that enables clinicians to gain a direct view of the fundus [
11]. Retromode imaging is similar to fundus photography in that it provides a similar field of view and can be performed very quickly in a noninvasive manner. Our comparison between these two techniques indicates a high clinical value of RMI, as it provides a good detection of the involved area. For fundus photography, ERM-related retinal changes are frequently represented by a yellowish/whitish appearance of the membrane associated with vessel tortuosity. retromode imaging can detect the involved macular area in pseudo-3D images with great sensitivity, delivering a more complete view of the anatomical conformation of the retina to the surgeon.
Moreover, monitoring the progression of the hyporeflective areas of the ERM on RMI may be very useful during the follow-up of affected patients, as their enlargement is very easy to detect.
As previously mentioned, retromode images demonstrated areas of increased reflectance with fingerprint patterns, containing radiating retinal striae centered on the fovea. We speculate these may represent areas of splitting of the horizontally oriented internal cone fibers, [
12] whereas the areas of decreased reflectance corresponded to the presence of more prominent large choroidal vessels (“dark choroid” aspect). Ahn, S.J. et al. [
13] identified a similar finding as well. We observed similar results as in a previous study on myopic patients, but, still, the precise explanation for this remains obscure [
12]. One explanation might be that the ERM causes a shadow effect, which obscures the underlying choroid.
RMI enhances the detection quality of ERM’s features compared to other common imaging techniques. In our cohort, this technique allowed to better visualize vessel traction and retinal folds compared to the other imaging modalities (FAF and fundus photography, p < 0.05). The ERM surface area detected using retromode was significantly larger than that detected by FAF (p < 0.05) and quite similar to that detected by fundus photography (p = 0.277). These results suggest that retromode imaging may be useful as a supplementary test for ERM detection.
Even though retromode imaging offers several advantages, it also displays some limitations. Above all, in this study, the detection rate of cystoid spaces on RMI was very low (only 2/21 eyes), whereas horizontal B-scanning revealed these lesions to be present in 100% of patients. In fact, the comparison of lesions in retromode imaging is often difficult, as many fundus details were obscured in these images. Moreover, as with most of the newly introduced imaging techniques, another drawback of RMI is its high cost.
Two major limitations of this study are its limited sample size and the fact that all images were manually cropped and superimposed. By comparing the measurements obtained by two retinal experts however, we feel like the risk of measurement errors was limited to the minimum. In the future, automated systems able to precisely compare different imaging modalities would be of help. Moreover, we did not analyze progression of ERMs’ associated pathological features and whether RMI features could be able to predict surgical results.
5. Conclusions
In conclusion, this study showed that retromode imaging is a new effective tool that can be used to gain a more accurate visualization of the real extension of an epiretinal membrane. Retromode analysis in cases of ERM allows for a pseudo-3D visualization of epiretinal changes and a 360-degree visualization around the fovea. There is no other imaging modality that can simultaneously provide all this information. Alongside the current imaging modalities, retromode imaging may serve as a useful supplementary test for the preoperative evaluation of ERMs. Clinicians should be aware of RMI’s advantages and should be able to use them to warrant a wide range of information and, thus, a more personalized therapeutic approach.
Author Contributions
Conceptualization, A.S., M.C.S., M.R. and S.R.; methodology, M.R.; software, M.R.; validation, M.C.S., S.R. and A.S.; formal analysis, M.R.; investigation, M.R.; resources, A.S., T.C., C.R., D.B., R.K., M.C.S., M.R. and S.R.; data curation, M.R.; writing—original draft preparation, M.R.; writing—review and editing, M.R., A.S. and R.K.; visualization, M.R.; supervision, A.S.; project administration, M.C.S.; funding acquisition, M.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Ministero della Salute Ricerca Corrente.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Policlinico Agostino Gemelli IRRCS (protocol ID number 3680/20).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Inoue, M.; Kadonosono, K. Macular Diseases: Epiretinal Membrane. Dev. Ophthalmol. 2014, 54, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, J.R.; Puliafito, C.A.; Hee, M.R.; Duker, J.S.; Reichel, E.; Coker, J.G.; Schuman, J.S.; Swanson, E.A.; Fujimoto, J.G. Characterization of Epiretinal Membranes Using Optical Coherence Tomography. Ophthalmology 1996, 103, 2142–2151. [Google Scholar] [CrossRef]
- Rispoli, M.; Rouic, J.F.L.; Lesnoni, G.; Colecchio, L.; Catalano, S.; Lumbroso, B. Retinal Surface En Face Optical Coherence Tomography: A New Imaging Approach in Epiretinal Membrane Surgery. Retina 2012, 32, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Lee, B.R.; Shin, Y.U. Retromode Imaging: Review and Perspectives. Saudi J. Ophthalmol. 2014, 28, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.; Zhang, X.; Wu, K.; Ji, Y.; Zuo, C.; Li, M.W.F. The Noninvasive Retro-Mode Imaging of Confocal Scanning Laser Ophthalmoscopy in Myopic Maculopathy: A Prospective Observational Study. Eye 2014, 28, 998–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, R.; Zhang, X.; Su, Y.; Li, M.; Wu, K.; Wen, F. The Noninvasive Retro-Mode Imaging Modality of Confocal Scanning Laser Ophthalmoscopy in Polypoidal Choroidal Vasculopathy: A Preliminary Application. PLoS ONE 2013, 8, e75711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savastano, A.; Lenzetti, C.; Finocchio, L.; Bacherini, D.; Giansanti, F.; Tartaro, R.; Piccirillo, V.; Savastano, M.C.; Virgili, S.R. Combining Cataract Surgery with 25-Gauge High-Speed Pars Plana Vitrectomy: Results from a Retrospective Study. Ophthalmology 2014, 121, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Lyon, J.A.; Garcia-Milian, R.; Norton, H.F.; Tennant, M.R. The Use of Research Electronic Data Capture (REDCap) Software to Create a Database of Librarian-Mediated Literature Searches. Med. Ref. Serv. Q. 2014, 33, 241–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorelick, M.H.; Yen, K. The Kappa Statistic Was Representative of Empirically Observed Inter-Rater Agreement for Physical Findings. J. Clin. Epidemiol. 2006, 59, 859–861. [Google Scholar] [CrossRef] [PubMed]
- Abràmoff, M.D.; Magalhães, P.J.; Ram, S.J. Image Processing with ImageJ. Biophotonics Int. 2004, 11, 36–41. [Google Scholar] [CrossRef]
- Song, J.H.; Moon, K.Y.; Jang, S.; Moon, Y.R. Comparison of MultiColor Fundus Imaging and Colour Fundus Photography in the Evaluation of Epiretinal Membrane. Acta Ophthalmol. 2019, 97, e533–e539. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Shimada, N.; Ohno-Matsui, K.; Hayashi, W.; Hayashi, K.; Moriyama, M.; Yoshida, T.; Tokoro, T.; Mochizuki, M. Retromode Retinal Imaging of Macular Retinoschisis in Highly Myopic Eyes. Am. J. Ophthalmol. 2010, 149, 635–640.e1. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Lee, S.U.; Lee, S.H.; Lee, B.R. Evaluation of Retromode Imaging for Use in Hydroxychloroquine Retinopathy. Am. J. Ophthalmol. 2018, 196, 44–52. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}