1. Introduction
The coronavirus disease (COVID-19) was first reported in Wuhan, Hubei Province, People’s Republic of China, in December 2019, and the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread worldwide and has caused more than 500 million cases and 6 million deaths as of May 2022. In South Korea, COVID-19 had afflicted more than 17 million individuals and had caused more than 20,000 deaths by May 2022.
The transmission of SARS-CoV-2 from an individual prior to symptom onset—that is, pre-symptomatic transmission—is a well-documented phenomenon and ranges from 45.9% (95% confidence interval [CI] 42.9–49.0%) to 69.1% (95% CI 66.2–71.9%) globally [
1]. According to the U.S. Centers for Disease Control and Prevention (CDC), 35% and 24% of all SARS-CoV-2 transmission could be attributed to pre-symptomatic individuals and those who remained asymptomatic, respectively [
2]. Pre-symptomatic individuals with SARS-CoV-2 infection are highly infectious immediately before and around the time of symptom onset and appear to transmit the virus efficiently, particularly within households [
3]. A study of a SARS-CoV-2 outbreak in a long-term care facility showed that the infectious virus could be isolated in cultures from the real-time reverse transcription–polymerase chain reaction (RT-PCR)-positive upper respiratory tract specimens of pre-symptomatic patients as early as 6 days prior to symptom onset [
4]. The risk of transmission from pre-symptomatic individuals is reported to be less than that from symptomatic individuals [
5,
6,
7]. However, pre-symptomatic individuals are less likely to isolate themselves from other people and, thus, the extent to which transmission from such individuals contributes to the pandemic is unknown. In addition, modeling studies have indicated that the widespread worldwide occurrence of COVID-19 would not have been possible without substantial pre-symptomatic transmission [
3]. A recent mathematical modeling study demonstrated the role of asymptomatic infection in the transmission potential of COVID-19 at the population level but did not explicitly incorporate the role of pre-symptomatic transmission [
8].
This study was conducted to estimate the proportion of pre-symptomatic transmission during the Delta variant’s predominance in South Korea by using individual-level data from a large number of confirmed local cases. Individual-level observations, including the timing of exposure, symptom onset, and onward transmission, are required to calculate the probability of pre-symptomatic transmission. However, due to the limited availability of individual-level data, we estimated the probability of pre-symptomatic transmission using the density distribution of the incubation period and the serial interval. Furthermore, we present our analysis of the incubation period and serial interval in accordance with the earlier and later phases of the outbreaks, given that control measures, such as expanded testing and implementation of social distancing strategies, were introduced during the time frame of the data that were analyzed.
2. Materials and Methods
In this retrospective population-based study, individual-level records, including age, sex, state of residence, autochthonous (local transmission)/imported case, and date of death, of confirmed COVID-19 cases were obtained from the database provided by the Korea Disease Control and Prevention Agency (KDCA) and Central Disease Control Headquarters. Some of these records included information on the date of contact with an infector and date of symptom onset and reporting. Specifically, data from 279,059 cases, recorded between 25 July 2021 and 4 December 2021 during the Delta variant’s predominance in South Korea, were extracted from the database and used to identify case reports that included information on contact tracing with matched pairs (i.e., case numbers of infectors or infectees) and dates of symptom onset. The dataset was filtered to obtain the data for dates of symptom onset, and 187,936 out of 279,059 cases in Period 2 were reported to have developed symptoms; this indicates that 33% of the reported cases were asymptomatic. Furthermore, the dataset was filtered to obtain the data for case numbers of infectors or infectees. Based on these infection pairs, we estimated the serial interval and incubation period distribution, which were then used to identify the proportion of pre-symptomatic transmission that is defined as the proportion of onward transmission during the infector’s incubation period. Specifically, we approximated the probability of pre-symptomatic transmission as the fraction of samples where the serial interval is shorter than the incubation period [
9]. We assume that, if the incubation period of an infector and of an infectee are taken to be independent and identically distributed, then the serial interval can be used to approximate the generation time [
1].
To estimate the proportion of pre-symptomatic transmission without and with expanded testing and social distancing strategies, we considered the two study periods (Period 1: 20 January 2020 to 10 February 2020; Period 2: 25 July 2021 to 4 December 2021). In South Korea, the first confirmed case was reported on 20 January 2020, and during Period 1, 28 COVID-19 cases were reported and limited expanded testing or implementation of social distancing strategies was undertaken. Following the identification of the local transmission cluster linked to members of the Shincheonji religious group in Daegu on 20 February, testing was expanded to include suspected cases based on the physicians’ judgement and individuals with no travel history. Period 2 has been chosen to incorporate the effects of interventional strategies including expanded testing during the Delta variant’s predominance into our analysis, given that the detection rate of the Delta variant accounted for more than 50% of local cases after 25 July 2021. To reduce the change in the serial interval by virus mutation, Period 2 was limited to the duration before the first appearance of the Omicron variant—that is, until 4 December 2021.
For Period 1, we used the reported mean incubation period (5.5 days; 95% CI 4.0–8.1 days) and serial interval (6.5 days; 95% CI 4.3–9.7 days), both of which were estimated based on the first 28 cases in South Korea [
10]. For the mean incubation period in Period 2, we used the prior estimate for the Delta variant (i.e., 4.4 days; 95% CI 3.9–5.0 days), and estimated the serial interval based on individual-level records, including information on date of contact with an infector, date of symptom onset, and date of reporting of confirmed COVID-19 cases to the KDCA and Central Disease Control Headquarters. Specifically, 187,936 COVID-19 cases were identified during Period 2 in South Korea. In the abovementioned datasets, some case reports included information pertaining to contact tracing with matched pairs (i.e., case numbers of infectors and infectees). The serial interval was defined as the time interval between symptom onset for both the infector and the infectee in the transmission chain (
Figure 1). To estimate the serial intervals, we identified transmission pairs that comprised the date of symptom onset for both the infector and infectee; accordingly, 29,009 transmission pairs were identified in Period 2.
To calculate the proportion of pre-symptomatic transmission, we randomly inferred the incubation period and serial interval distributions before comparing each pair. In general, a serial interval that is shorter than the incubation period is considered indicative of pre-symptomatic transmission (
Figure 1). To examine the proportion of pre-symptomatic transmission assuming no correlation between incubation period and serial interval, we randomly drew samples from the distributions and paired them randomly. By contrast, when considering positive and negative correlations, we aligned samples of the incubation period and serial interval either both in ascending order or with one in ascending and the other in descending order (rank ordering) prior to calculating the proportion of pre-symptomatic transmission, respectively [
9].
3. Results
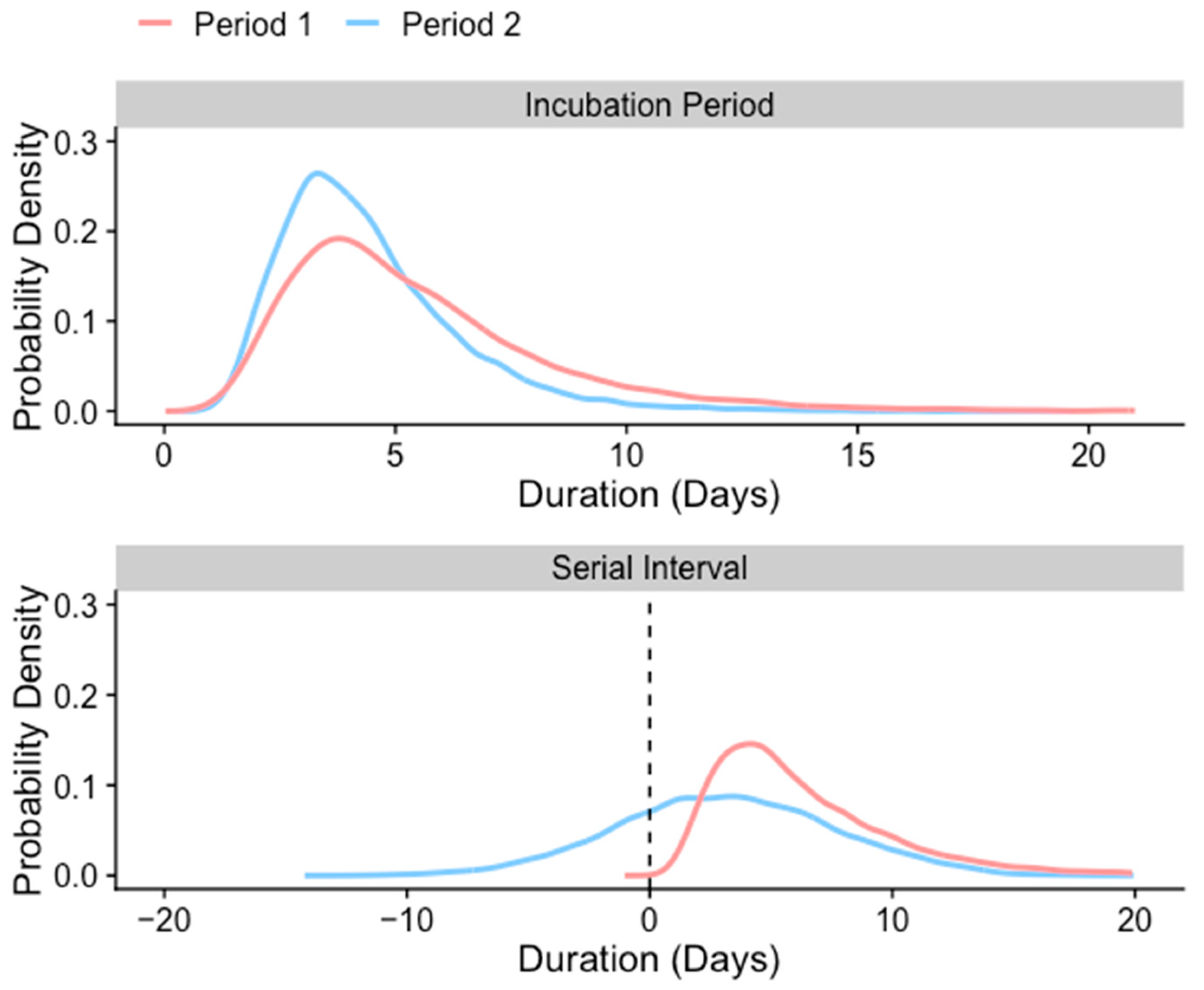
For Period 1, wherein there was no expanded testing or implementation of social distancing strategies, the probability density functions for the reported incubation period and serial interval were reported by fitting the log-normal distribution (mean 5.5 days, 95% CI 4.0–8.1 days and mean 6.5 days, 95% CI 4.3–9.7 days, respectively) from an earlier study (
Figure 2) [
10]. For Period 2, when the Delta variant was the predominant SARS-CoV-2 variant in South Korea, the incubation period was previously estimated by fitting the lognormal distribution (mean 4.4 days, 95% CI 3.9–5.0 days) [
11], and we estimated the serial interval (mean 3.2 days, 95% CI 3.1–3.2 days) from the individual-level COVID-19 case records in South Korea (
Figure 2 and
Figure S1 in the
Supplementary Materials).
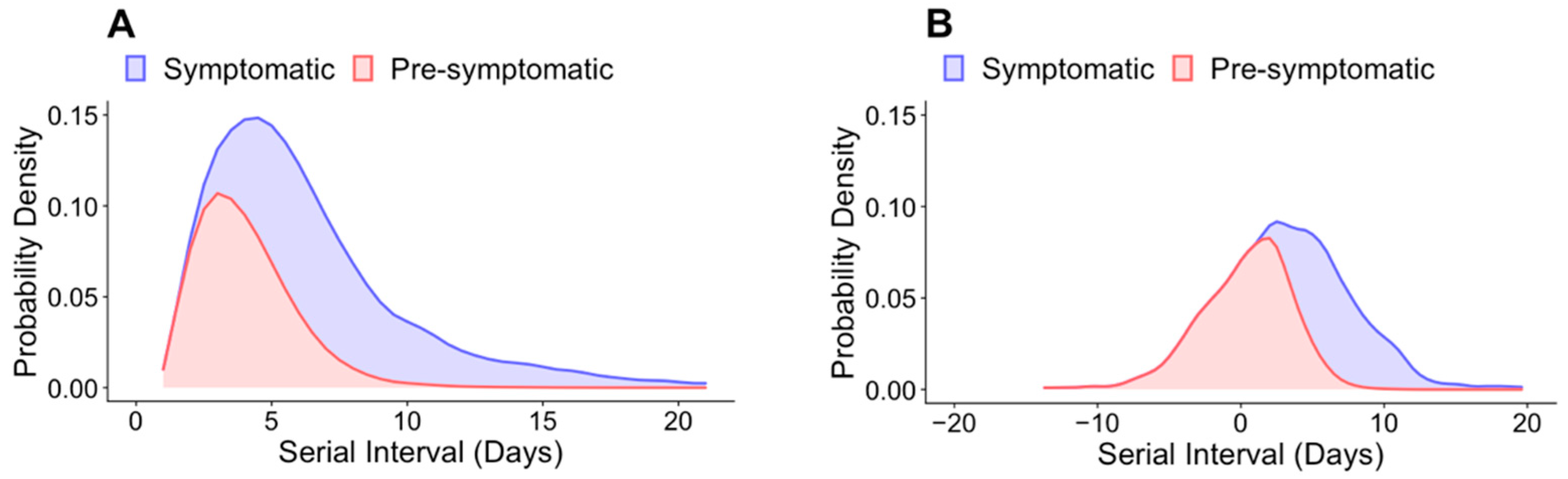
Using these estimates for the incubation period and serial intervals, we examined the proportion of onward transmission that occurred during the pre-symptomatic period in South Korea. Assuming that the serial interval and incubation period distributions were uncorrelated, we estimated that, in the absence of expanded testing or implementation of social distancing strategies, the proportion of pre-symptomatic transmission of SARS-CoV-2 was 43.5% (range accounting for correlation: 9.9–45.4%;
Figure 3A and
Table 1). With the implementation of expanded case-finding efforts and subsequent isolation on symptom onset, it is anticipated that pre-symptomatic transmission would account for a greater proportion of all transmission events. In support of this hypothesis, the results of our simulation show that 60.0% of transmission events in Period 2 occurred prior to symptom onset in the primary case, assuming uncorrelated serial interval and incubation period distributions (
Figure 3B and
Table 1). Furthermore, in both periods, the pre-symptomatic transmission ratio gradually decreased as the serial interval increased (
Figure 3). For periods 1 and 2, the proportion of symptomatic transmission was greater than 0.5 when the serial interval was at least 4.9 and 4 days, respectively (
Figure 3).
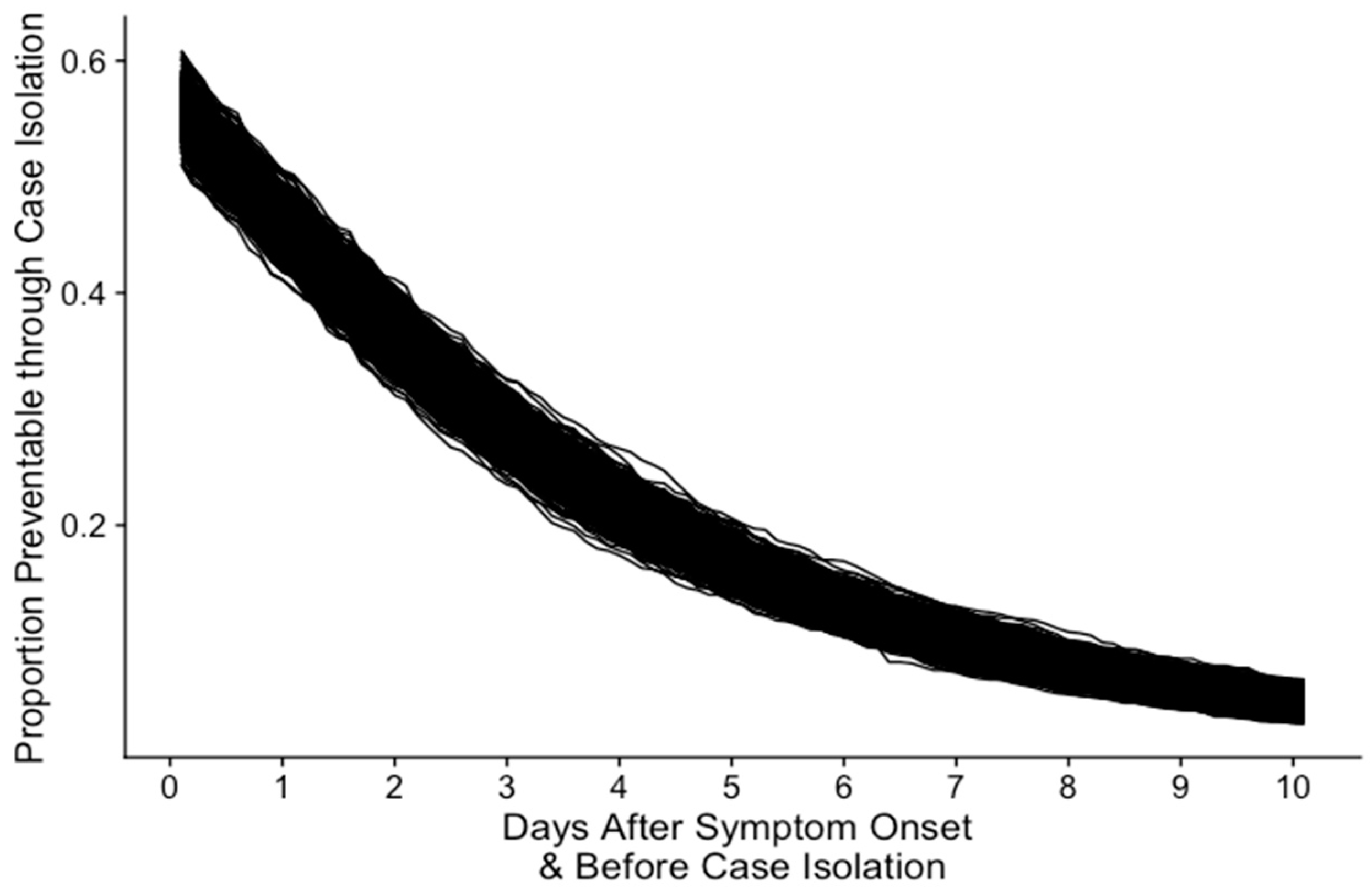
Depending on the time of case isolation after symptom onset, a proportion of symptomatic transmission is preventable. If the case isolation is performed immediately after symptom onset, our results show that up to 60% of symptomatic transmission could be prevented (
Figure 4). However, if the case isolation is performed after approximately three days, the proportion of preventable symptomatic transmission is decreased by half and is followed by the less preventable symptomatic transmission.
4. Discussion
We calculated the proportion of pre-symptomatic transmission of COVID-19 cases in South Korea based on the extent of overlap in the distribution of the incubation period and the serial interval. We found differences in the estimated serial intervals between the periods wherein social distancing measures including expanded testing or implementation of social distancing strategies were present or absent. Consistent with the results of other studies [
12], our results indicate that the serial interval in South Korea decreased with a relatively high level of restrictions. Moreover, our study shows that interventions, such as rapid isolation of symptomatic individuals, would result in the occurrence of a greater proportion of transmission earlier in the infectious period, leading to more pre-symptomatic transmission, which is consistent with the results of earlier studies [
1,
12,
13].
The portion of pre-symptomatic transmission is a central quantity for infection control; however, for COVID-19, there is a substantial amount of uncertainty in the contribution of asymptomatic infections to the total transmission dynamics [
14]. The possibility of pre-symptomatic transmission in COVID-19 cases is supported by the findings that both the viral genome and the live virus have been detected in upper respiratory samples prior to symptom onset [
1,
4,
15] and that symptom onset in the infectee preceded symptom onset in the infector [
16,
17]. Pre-symptomatic transmission of SARS-CoV-2 in COVID-19 is further supported by quantitative studies based on the estimation of serial intervals or by similar or shorter generation times than the incubation period [
17,
18,
19]. In addition, virus shedding peaks on or before symptom onset, and the peak transmission period is between the 2 days before and the 3 days after symptom onset, thereby indicating the transmission potential of the virus before symptom onset [
20].
A prior meta-analysis that analyzed data from China, Iran, Italy, South Korea, Singapore, and Vietnam estimated that the proportion of pre-symptomatic transmission rate of COVID-19 cases ranges from 45.9% (95% CI 42.9–49.0%) to 69.1% (95% CI 66.2–71.9%), with which our estimates match (
Table 2) [
1]. In addition, Chun et al. used a dataset (72 transmission pairs) that was obtained from South Korea between 23 January 2020 and 31 March 2020 and estimated that 37% (95% CI 16–52%) of the transmission occurred pre-symptomatically; the authors thus concluded that the peak transmission occurred 0.72 days before symptom onset [
21]. Similarly, based on data (40 transmission pairs) from several countries, Ferretti et al. inferred that 37% (95% CI 27.5–45%) of transmission was pre-symptomatic [
22]. Furthermore, the analysis of the data in Beijing, China indicates that pre-symptomatic transmission may range from 15% to 81% [
23]. He et al. investigated 77 transmission pairs from multiple countries and estimated that 44% (95% CI 30–57%) of transmission was pre-symptomatic [
17].
Our study has some limitations. First, we approximated the generation time using the serial interval, which is the time between symptom onset in the infector and infectee, because generation time is difficult to observe directly. In our analysis, we assumed that the subtraction of the incubation period from generation time would yield the transmission time relative to symptom onset, thus facilitating an evaluation of whether transmission occurred prior to symptom onset. Second, we used population-level estimates of the serial interval and incubation period rather than individual-level estimates. Potential biases may arise from the correlation of the two estimates at the individual level, which we addressed by carrying out additional analyses under the assumption of positive or negative correlation.
5. Conclusions
Our study clearly indicates that substantial pre-symptomatic transmission occurs, which is consistent with the evidence reported from virological studies, case reports, and other modeling studies. Our findings highlight the need for rapid and effective case detection, contact tracing, and quarantine measures before potential symptom manifestation to ensure effective control strategies.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jcm11143925/s1. Figure S1: Histogram and the distribution of serial intervals in Period 2. Red line shows the fitted probability density function. Table S1: The fitted probability density functions, with the estimated mean, variance, and other parameters of the probability density functions. Pseudo-code for estimating the proportion of pre-symptomatic transmission.
Author Contributions
Conceptualization, E.S.; methodology, E.S.; software, Y.S.; investigation, E.S.; data curation, Y.S.; writing—original draft preparation, E.S. and Y.S.; writing—review and editing, E.S. and Y.S.; visualization, Y.S.; supervision, E.S.; project administration, E.S.; funding acquisition, E.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1A6A1A10044154).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and was exempt from ethical approval due to a waiver that was granted by the Institutional Review Board of Soongsil University (SSU-202202-HR-381-1).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We appreciate the Korea Disease Control and Prevention Agency (KDCA) and the Central Disease Control Headquarters for providing the data from the database of reported COVID-19 cases.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Casey-Bryars, M.; Griffin, J.; McAloon, C.; Byrne, A.; Madden, J.; Mc Evoy, D.; Collins, A.; Hunt, K.; Barber, A.; Butler, F.; et al. Presymptomatic transmission of SARS-CoV-2 infection: A secondary analysis using published data. BMJ Open 2021, 11, e041240. [Google Scholar] [CrossRef]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 Transmission from People without COVID-19 Symptoms. JAMA Netw. Open 2021, 4, e2035057. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Nergiz, A.I.; Maraolo, A.E.; Bogoch, I.I.; Low, N.; Cevik, M. The role of asymptomatic and pre-symptomatic infection in SARS-CoV-2 transmission—A living systematic review. Clin. Microbiol. Infect. 2021, 27, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Madewell, Z.J.; Yang, Y.; Longini, I.M., Jr.; Halloran, M.E.; Dean, N.E. Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2031756. [Google Scholar] [CrossRef]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Ipekci, A.M.; Salanti, G.; Low, N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med. 2020, 17, e1003346. [Google Scholar] [CrossRef]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong, S.E.; Toh, M.P.; Lee, V.J. Presymptomatic Transmission of SARS-CoV-2—Singapore, January 23–March 16, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Chen, Z.; He, Y.; Liu, T.; Cheng, X.; Xiao, J.; Feng, H. Why Controlling the Asymptomatic Infection Is Important: A Modelling Study with Stability and Sensitivity Analysis. Fractal Fract. 2022, 6, 197. [Google Scholar] [CrossRef]
- Liu, Y.; Centre for Mathematical Modelling of Infectious Diseases nCoV Working Group; Funk, S.; Flasche, S. The contribution of pre-symptomatic infection to the transmission dynamics of COVID-2019. Wellcome Open Res. 2020, 5, 58. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.S.; Kim, J.-H.; Ahn, C.Y.; Lee, H. Subcritical Transmission in the Early Stage of COVID-19 in Korea. Int. J. Environ. Res. Public Health 2021, 18, 1265. [Google Scholar] [CrossRef]
- Zhang, M.; Xiao, J.; Deng, A.; Zhang, Y.; Zhuang, Y.; Hu, T.; Li, J.; Tu, H.; Li, B.; Zhou, Y. Transmission dynamics of an outbreak of the COVID-19 Delta variant B. 1.617. 2—Guangdong Province, China, May–June 2021. China CDC Wkly. 2021, 3, 584–586. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.T.; Wang, L.; Lau, E.H.Y.; Xu, X.K.; Du, Z.; Wu, Y.; Leung, G.M.; Cowling, B.J. Serial interval of SARS-CoV-2 was shortened over time by nonpharmaceutical interventions. Science 2020, 369, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- Fraser, C.; Riley, S.; Anderson, R.M.; Ferguson, N.M. Factors that make an infectious disease outbreak controllable. Proc. Natl. Acad. Sci. USA 2004, 101, 6146–6151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavezzo, E.; Franchin, E.; Ciavarella, C.; Cuomo-Dannenburg, G.; Barzon, L.; Del Vecchio, C.; Rossi, L.; Manganelli, R.; Loregian, A.; Navarin, N.; et al. Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’. Nature 2020, 584, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Chaw, L.; Koh, W.C.; Alikhan, M.F.; Jamaludin, S.A.; Poh, W.W.P.; Naing, L. Epidemiological Investigation of the First 135 COVID-19 Cases in Brunei: Implications for Surveillance, Control, and Travel Restrictions. Am. J. Trop. Med. Hyg. 2020, 103, 1608–1613. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Nishiura, H.; Linton, N.M.; Akhmetzhanov, A.R. Serial interval of novel coronavirus (COVID-19) infections. Int. J. Infect. Dis. 2020, 93, 284–286. [Google Scholar] [CrossRef]
- Ren, X.; Li, Y.; Yang, X.; Li, Z.; Cui, J.; Zhu, A.; Zhao, H.; Yu, J.; Nie, T.; Ren, M.; et al. Evidence for pre-symptomatic transmission of coronavirus disease 2019 (COVID-19) in China. Influenza Other Respir. Viruses 2021, 15, 19–26. [Google Scholar] [CrossRef]
- Torjesen, I. Covid-19: Peak of viral shedding is later with omicron variant, Japanese data suggest. BMJ 2022, 376, o89. [Google Scholar] [CrossRef]
- Chun, J.Y.; Baek, G.; Kim, Y. Transmission onset distribution of COVID-19. Int. J. Infect. Dis. 2020, 99, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dorner, L.; Parker, M.; Bonsall, D.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, 1686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Muscatello, D.; Tian, Y.; Chen, Y.; Li, S.; Duan, W.; Ma, C.; Sun, Y.; Wu, S.; Ge, L.; et al. Role of presymptomatic transmission of COVID-19: Evidence from Beijing, China. J. Epidemiol. Community Health 2021, 75, 84–87. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).








{kind=link}
{kind=link}
{kind=link}
{kind=link}