
Asymptomatic Left Ventricular Hypertrophy Is a Potent Risk Factor for the Development of HFpEF but Not HFrEF: Results of a Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
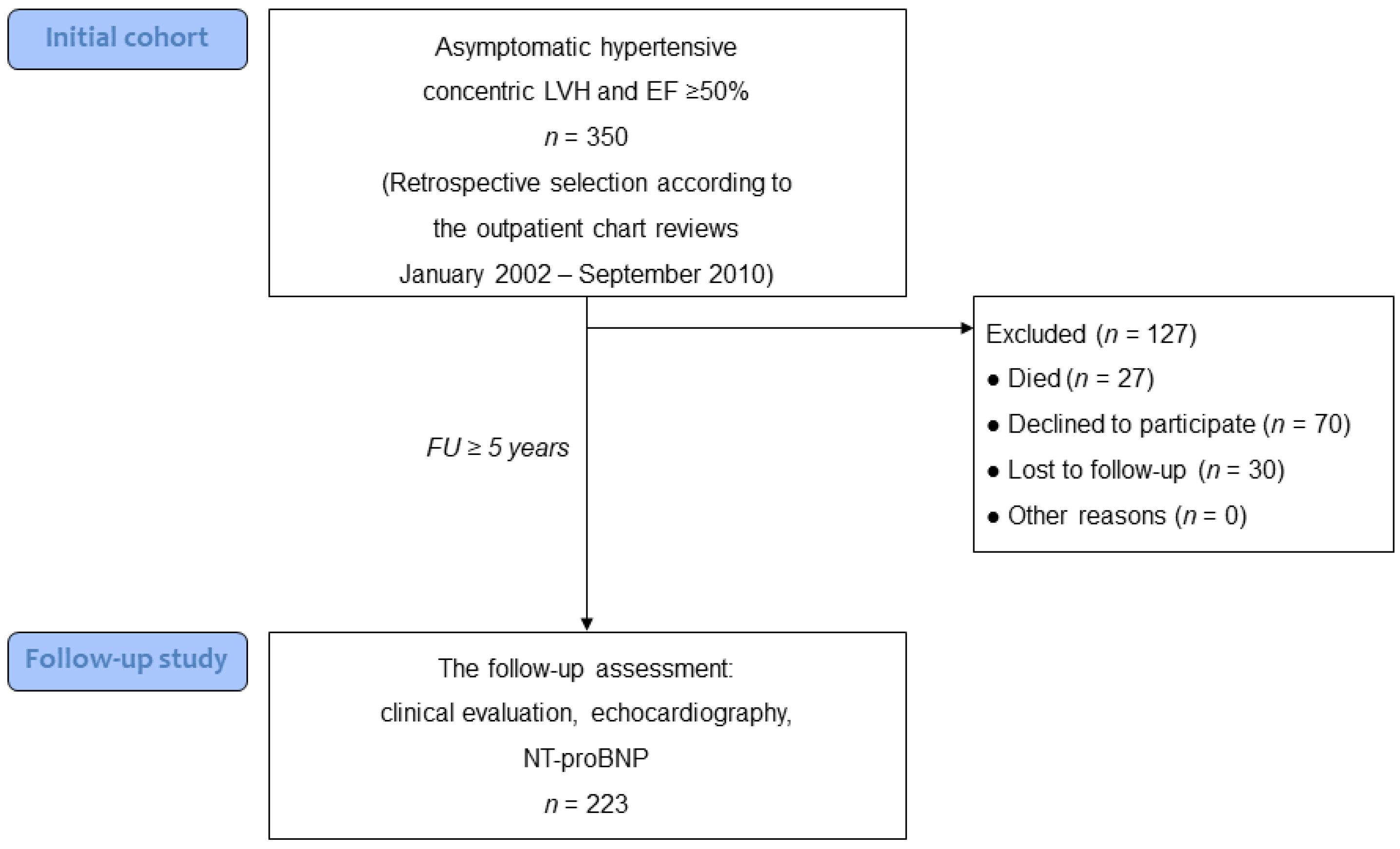
2.1. Study Population
2.2. Study Design
2.3. Echocardiography
2.4. NT-proBNP
2.5. Study Endpoint
2.6. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
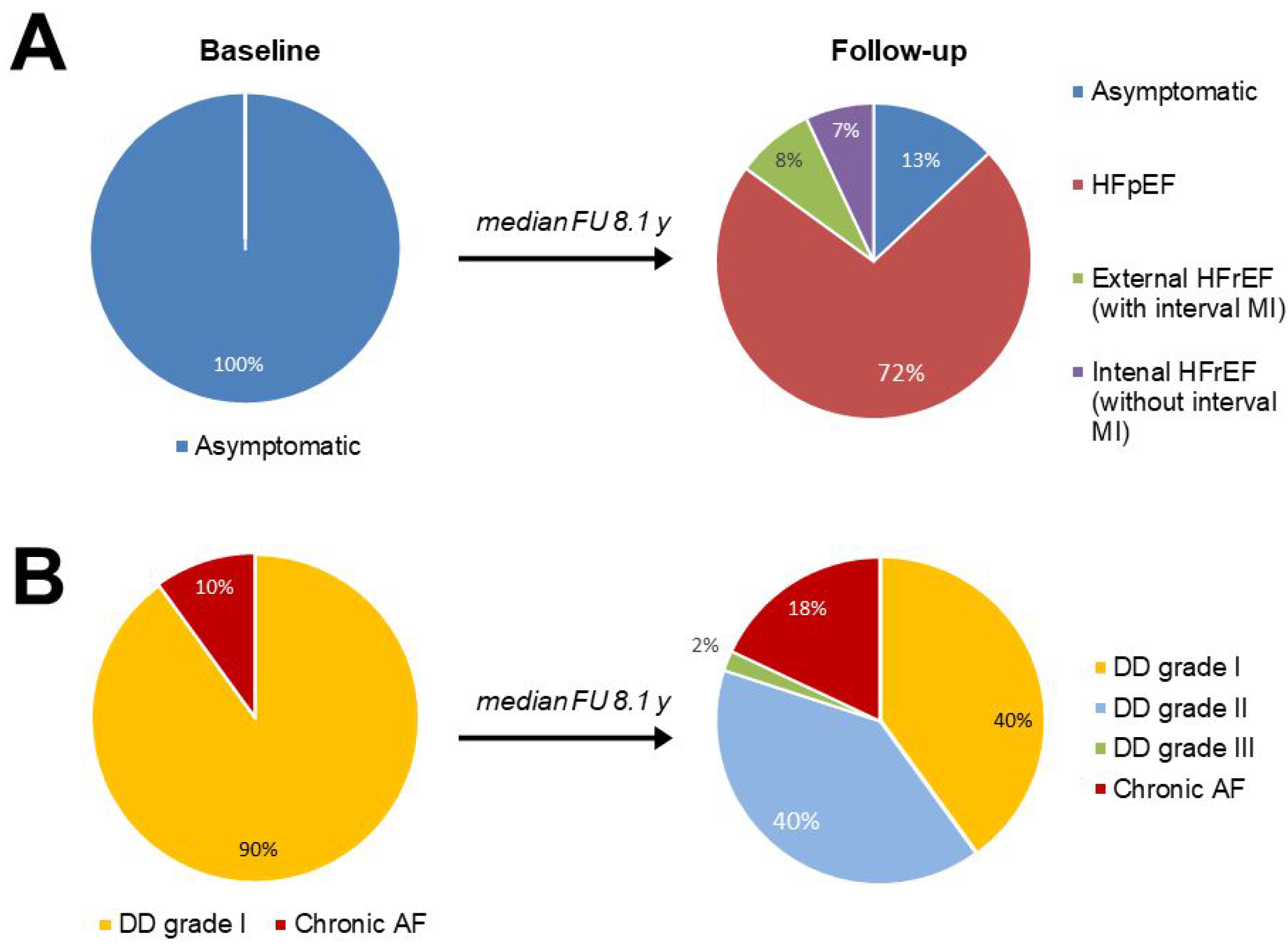
3.2. Patient Follow-Up Characteristics
3.3. The Comparison of Patients with New-Onset Heart Failure and Those Who Remained Asymptomatic after the Follow-Up
3.4. The Predictors of HF Development
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; di Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Sala, C.; Negri, F.; Mancia, G.; Morganti, A.; Italian Society of Hypertension. Prevalence of left-ventricular hypertrophy in hypertension: An updated review of echocardiographic studies. J. Hum. Hypertens. 2012, 26, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosse, P.; Cremer, A.; Vircoulon, M.; Coulon, P.; Jan, E.; Papaioannou, G.; Yeim, S. Prognostic value of the extent of left ventricular hypertrophy and its evolution in the hypertensive patient. J. Hypertens. 2012, 30, 2403–2409. [Google Scholar] [CrossRef]
- Seliger, S.L.; de Lemos, J.; Neeland, I.J.; Christenson, R.; Gottdiener, J.; Drazner, M.H.; Berry, J.; Sorkin, J.; deFilippi, C. Older Adults, “Malignant” Left Ventricular Hypertrophy, and Associated Cardiac-Specific Biomarker Phenotypes to Identify the Differential Risk of New-Onset Reduced Versus Preserved Ejection Fraction Heart Failure: CHS (Cardiovascular Health Study). JACC Heart Fail. 2015, 6, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Abate, K.H.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Drazner, M.H. The progression of hypertensive heart disease. Circulation 2011, 123, 327–334. [Google Scholar] [CrossRef]
- Gaasch, W.H.; Zile, M.R. Left ventricular structural remodeling in health and disease: With special emphasis on volume, mass, and geometry. J. Am. Coll. Cardiol. 2011, 58, 1733–1740. [Google Scholar] [CrossRef] [Green Version]
- Frohlich, E.D.; Apstein, C.; Chobanian, A.V.; Devereux, R.B.; Dustan, H.P.; Dzau, V.; Fauad-Tarazi, F.; Horan, M.J.; Marcus, M.; Massie, B.; et al. The heart in hypertension. N. Engl. J. Med. 1992, 327, 998–1008. [Google Scholar] [CrossRef]
- Iriarte, M.; Murga, N.; Sagastagoitia, D.; Morillas, M.; Boveda, J.; Molinero, E.; Etxebeste, J.; Salcedo, A.; Rodriguez, E.; Ormaetxe, J.M. Classification of hypertensive cardiomyopathy. Eur. Heart J. 1993, 14 (Suppl. J), 95–101. [Google Scholar]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.K.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo Esachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Takeuchi, M.; Borden, W.B.; Nakai, H.; Nishikage, T.; Kokumai, M.; Nagakura, T.; Otani, S.; Lang, R.M. Reduced and delayed untwisting of the left ventricle in patients with hypertension and left ventricular hypertrophy: A study using two-dimensional speckle tracking imaging. Eur. Heart J. 2007, 28, 2756–2762. [Google Scholar] [CrossRef] [Green Version]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramasubbu, K.; Estep, J.; White, D.L.; Deswal, A.; Mann, D.L. Experimental and clinical basis for the use of statins in patients with ischemic and nonischemic cardiomyopathy. J. Am. Coll. Cardiol. 2008, 51, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Akahori, H.; Tsujino, T.; Naito, Y.; Matsumoto, M.; Sasaki, N.; Iwasaku, T.; Eguchi, A.; Sawada, H.; Hirotani, S.; Masuyama, T. Atorvastatin ameliorates cardiac fibrosis and improves left ventricular diastolic function in hypertensive diastolic heart failure model rats. J. Hypertens. 2014, 32, 1534–1541. [Google Scholar] [CrossRef]
- Yamada, Y.; Takeuchi, S.; Yoneda, M.; Ito, S.; Sano, Y.; Nagasawa, K.; Matsuura, N.; Uchinaka, A.; Murohara, T.; Nagata, K. Atorvastatin reduces cardiac and adipose tissue inflammation in rats with metabolic syndrome. Int. J. Cardiol. 2017, 240, 332–338. [Google Scholar] [CrossRef]
- Patel, R.; Nagueh, S.F.; Tsybouleva, N.; Abdellatif, M.; Lutucuta, S.; Kopelen, H.A.; Quinones, M.A.; Zoghbi, W.A.; Entman, M.L.; Roberts, R.; et al. Simvastatin induces regression of cardiac hypertrophy and fibrosis and improves cardiac function in a transgenic rabbit model of human hypertrophic cardiomyopathy. Circulation 2001, 104, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Okura, H.; Asawa, K.; Kubo, T.; Taguchi, H.; Toda, I.; Yoshiyama, M.; Yoshikawa, J.; Yoshida, K. Impact of statin therapy on systemic inflammation, left ventricular systolic and diastolic function and prognosis in low risk ischemic heart disease patients without history of congestive heart failure. Intern. Med. 2007, 46, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Yagi, S.; Akaike, M.; Aihara, K.-I.; Iwase, T.; Ishikawa, K.; Yoshida, S.; Sumitomo-Ueda, Y.; Kusunose, K.; Niki, T.; Yamaguchi, K.; et al. Effect of low-dose (1 mg/day) pitavastatin on left ventricular diastolic function and albuminuria in patients with hyperlipidemia. Am. J. Cardiol. 2011, 107, 1644–1649. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Zheng, X.-X.; Xu, Y.-L.; Ru, J.; Hui, R.T.; Huang, X.H. Meta-analysis of the effect of statins on mortality in patients with preserved ejection fraction. Am. J. Cardiol. 2014, 113, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Drexel, H.; Coats, A.J.S.; Spoletini, I.; Bilato, C.; Mollace, V.; Perrone Filardi, P.; Rosano, G.M.C. An expert opinion paper on statin adherence and implementation of new lipid-lowering medications by the ESC Working Group on Cardiovascular Pharmacotherapy: Barriers to be overcome. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 115–121. [Google Scholar] [CrossRef]
- Heckbert, S.R.; Post, W.; Pearson, G.D.; Arnett, D.K.; Gomes, A.S.; Jerosch-Herold, M.; Hundley, W.G.; Lima, J.A.; Bluemke, D.A. Traditional cardiovascular risk factors in relation to left ventricular mass, volume, and systolic function by cardiac magnetic resonance imaging: The Multiethnic Study of Atherosclerosis. J. Am. Coll. Cardiol. 2006, 48, 2285–2292. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.V.; Abbasi, S.A.; Heydari, B.; Rickers, C.; Jacobs, D.R., Jr.; Wang, L.; Kwong, R.Y.; Bluemke, D.A.; Lima, J.A.; Jerosch-Herold, M. Insulin resistance, subclinical left ventricular remodeling, and the obesity paradox: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2013, 61, 1698–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, A.; Katz, R.; Jenny, N.S.; Astor, B.; Bluemke, D.A.; Lima, J.A.; Siscovick, D.; Bertoni, A.G.; Shlipak, M.G. Left ventricular hypertrophy in mild and moderate reduction in kidney function determined using cardiac magnetic resonance imaging and cystatin C: The multi-ethnic study of atherosclerosis (MESA). Am. J. Kidney Dis. 2008, 52, 839–848. [Google Scholar] [CrossRef] [Green Version]
- Massie, B.M.; Carson, P.E.; McMurray, J.J.; Komajda, M.; McKelvie, R.; Zile, M.R.; Anderson, S.; Donovan, M.; Iverson, E.; Staiger, C.; et al. Irbesartan in patients with heart failure and preserved ejection fraction. N. Engl. J. Med. 2008, 359, 2456–2467. [Google Scholar] [CrossRef] [Green Version]
- Cleland, J.G.; Tendera, M.; Adamus, J.; Freemantle, N.; Polonski, L.; Taylor, J.; PEP-CHF Investigators. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J. 2006, 27, 2338–2345. [Google Scholar] [CrossRef] [Green Version]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for heart failure with preserved ejection fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; Rizkala, A.R.; Gong, J.; Wang, W.; Anand, I.S.; Ge, J.; Lam, G.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; et al. Angiotensin Receptor Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction: Rationale and Design of the PARAGON-HF Trial. JACC Heart Fail. 2017, 5, 471–482. [Google Scholar] [CrossRef]
- Zile, M.R.; Gottdiener, J.S.; Hetzel, S.J.; McMurray, J.J.; Komajda, M.; McKelvie, R.; Baicu, C.F.; Massie, B.M.; Carson, P.E.; I-PRESERVE Investigators. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation 2011, 124, 2491–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meerzon, F.Z. Compensatory hyperfunction of the heart and cardiac insufficiency. Circ. Res. 1962, 10, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeffer, J.M.; Pfeffer, M.A.; Mirsky, I.; Braunwald, E. Regression of left ventricular hypertrophy and prevention of left ventricular dysfunction by captopril in the spontaneously hypertensive rat. Proc. Natl. Acad. Sci. USA 1982, 79, 3310–3314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molkentin, J.D.; Lu, J.R.; Antos, C.L.; Markham, B.; Richardson, J.; Robbins, J.; Grant, S.R.; Olson, E.N. A calcineurin-dependent transcriptional pathway for cardiac hypertrophy. Cell 1998, 93, 215–228. [Google Scholar] [CrossRef] [Green Version]
- Kosmala, W.; Plaksej, R.; Strotmann, J.M.; Weigel, C.; Herrmann, S.; Niemann, M.; Mende, H.; Störk, S.; Angermann, C.E.; Wagner, J.A.; et al. Progression of left ventricular functional abnormalities in hypertensive patients with heart failure: An ultrasonic two-dimensional speckle tracking study. J. Am. Soc. Echocardiogr. 2008, 21, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Khoury, D.S.; Yue, Y.; Torre-Amione, G.; Nagueh, S.F. Preserved left ventricular twist and circumferential deformation, but depressed longitudinal and radial deformation in patients with diastolic heart failure. Eur. Heart J. 2008, 29, 1283–1289. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J.; Miyazaki, C.; Bruce, C.J.; Ommen, S.; Miller, F.A.; Oh, J.K. Left ventricular torsion by two-dimensional speckle tracking echocardiography in patients with diastolic dysfunction and normal ejection fraction. J. Am. Soc. Echocardiogr. 2008, 21, 1129–1137. [Google Scholar] [CrossRef]
- Rame, J.E.; Ramilo, M.; Spencer, N.; Blewett, C.; Mehta, S.K.; Dries, D.L.; Drazner, M.H. Development of a depressed left ventricular ejection fraction in patients with left ventricular hypertrophy and a normal ejection fraction. Am. J. Cardiol. 2004, 93, 234–237. [Google Scholar] [CrossRef]
- Drazner, M.H.; Rame, J.E.; Marino, E.K.; Gottdiener, J.S.; Kitzman, D.W.; Gardin, J.M.; Manolio, T.A.; Dries, D.L.; Siscovick, D.S. Increased left ventricular mass is a risk factor for the development of a depressed left ventricular ejection fraction within five years: The Cardiovascular Health Study. J. Am. Coll. Cardiol. 2004, 43, 2207–2215. [Google Scholar] [CrossRef] [Green Version]
- Krishnamoorthy, A.; Brown, T.; Ayers, C.R.; Gupta, S.; Rame, J.E.; Patel, P.C.; Markham, D.W.; Drazner, M.H. Progression from normal to reduced left ventricular ejection fraction in patients with concentric left ventricular hypertrophy after long-term follow-up. Am. J. Cardiol. 2011, 108, 997–1001. [Google Scholar] [CrossRef]
- Gopinathannair, R.; Sullivan, R.; Olshansky, B. Tachycardia-mediated cardiomyopathy: Recognition and management. Curr. Heart Fail. Rep. 2009, 6, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Okin, P.M.; Bang, C.N.; Wachtell, K.; Hille, D.A.; Kjeldsen, S.E.; Dahlöf, B.; Devereux, R.B. Relationship of sudden cardiac death to new-onset atrial fibrillation in hypertensive patients with left ventricular hypertrophy. Circ. Arrhythm. Electrophysiol. 2013, 6, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducharme, A.; Swedberg, K.; Pfeffer, M.A.; Cohen-Solal, A.; Granger, C.B.; Maggioni, A.P.; Michelson, E.L.; McMurray, J.J.; Olsson, L.; Rouleau, J.L.; et al. Prevention of atrial fibrillation in patients with symptomatic chronic heart failure by candesartan in the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Am. Heart J. 2006, 152, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, A.P.; Latini, R.; Carson, P.E.; Singh, S.N.; Barlera, S.; Glazer, R.; Masson, S.; Cerè, E.; Tognoni, G.; Cohn, J.N.; et al. Valsartan reduces the incidence of atrial fibrillation in patients with heart failure: Results from the Valsartan Heart Failure Trial (Val-HeFT). Am. Heart J. 2005, 149, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, R.; Chamberlain, A.M.; Roger, V.L.; Redfield, M.M. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: A community-based study. Circulation 2013, 128, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Levy, D.; Garrison, R.J.; Savage, D.D.; Kannel, W.B.; Castelli, W.P. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N. Engl. J. Med. 1990, 322, 1561–1566. [Google Scholar] [CrossRef]
- Pieske, B.; Tschöpe, C.; de Boer, R.A.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to diagnose heart failure with preserved ejection fraction: The HFA-PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 40, 3297–3317. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Hypertensive LV Hypertrophy | p Value | |
|---|---|---|---|
| n = 223 | |||
| Baseline | Follow-Up | ||
| Clinical parameters: | |||
| Age, y | 59 (52–68) | ||
| Men | 65% | ||
| Duration of hypertension, y | 20 (11–30) | ||
| Hypertension a | 100% | 100% | 1 |
| Chronic atrial fibrillation | 10% | 18% | 0.027 |
| Ischemic heart disease | 35% | 44% | 0.053 |
| Myocardial infarction | 18% | 28% | 0.01 |
| Myocardial revascularization | 14% | 19% | 0.097 |
| Diabetes mellitus | 20% | 31% | 0.009 |
| Body mass index, kg/m2 | 30.4 (27.2–34.4) | 30.8 (27.8–35.0) | 0.06 |
| Obesity b | 52% | 57% | 0.34 |
| Chronic kidney disease c | 29% | 40% | 0.013 |
| Chronic obstructive pulmonary disease | 9% | 13% | 0.22 |
| Clinical status of LV hypertrophy: | |||
| Asymptomatic | 100% | 13% | <0.001 |
| HFpEF | 0% | 72% | |
| HFrEF | 0% | 15% | |
| A follow-up (interval) therapy: | |||
| ACEI/ARB | 66% | ||
| β-Blockers | 56% | ||
| Calcium channel blockers | 24% | ||
| Loop diuretics | 43% | ||
| Thiazide diuretics | 23% | ||
| Mineralocorticoid receptors antagonists | 9% | ||
| Statins | 40% | ||
| ≥2 antihypertensive drugs | 68% | ||
| Echocardiographic measures | |||
| LV mass index, g/m2 | 136 (116–158) | 136 (116–171) | 0.17 |
| LV end-diastolic dimension, cm | 5.2 (5.0–5.6) | 4.8 (4.5–5.0) | <0.001 |
| Relative wall thickness | 0.46 (0.44–0.49) | 0.54 (0.51–0.60) | <0.001 |
| Type of LV hypertrophy: | 0.061 | ||
| Concentric | 100% | 98% | |
| Eccentric | 0% | 2% | |
| LA anteroposterior diameter, cm | 4.1 (3.9–4.4) | 4.5 (4.2–4.9) | <0.001 |
| LV diastolic dysfunction,d grade: | <0.001 | ||
| I | 100% | 48% | |
| II | 0% | 49% | |
| III | 0% | 3% | |
| Pulmonary artery systolic pressure, mm Hg | 24 (23–30) | 32 (27–40) | <0.001 |
| Pulmonary hypertension,e n (%) | 13% | 40% | <0.001 |
| Variables | Asymptomatic (n = 28) | Transition to HFpEF (n = 161) | Transition to Internal HFrEF (n = 16) | |||
|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Initial Visit | Follow-Up Visit | Initial Visit | Follow-Up Visit | |
| Clinical parameters: | ||||||
| Age, y | 54 (48–64) | 61 (52–69) § | 58 (54–63) | |||
| Men | 57% | 62% | 81% | |||
| Duration of follow-up, y | 8.2 (6.4–9.6) | 8.1 (6.9–10.2) | 9.1 (6.9–11.4) | |||
| Duration of hypertension, y | 15 (10–20) | 20 (14.5–30) § | 25 (10–30) § | |||
| Chronic atrial fibrillation | 0% | 0% | 8% | 15% *§ | 38% §§µµ | 63% §§µµ |
| Ischemic heart disease | 29% | 32% | 37% | 43% | 6% µ | 13% µ |
| Previous MI | 14% | 25% | 21% | 23% | 6% | 6% |
| Myocardial revascularization | 11% | 18% | 15% | 19% | 6% | 6% |
| Diabetes mellitus | 14% | 25% | 21% | 31% | 19% | 44% |
| Body mass index, kg/m2 | 29.8 (26.4–34.6) | 30.8 (27.8–35.9) | 30.0 (27.5–34.0) | 30.5 (28.0–33.8) | 32.2 (29.7–38.0) | 35.4 (29.3–40.1) µ* |
| Obesity a | 50% | 57% | 50% | 54% | 75% | 75% |
| Chronic kidney disease b | 18% | 29% | 33% | 44% | 25% | 44% |
| COPD | 14% | 18% | 6% | 9% | 19% | 25% |
| Systolic BP, mm Hg | 138 (123–159) | 138 (122–156) | 148 (130–159) | 149 (131–161) | 152 (138–159) | 154 (139–160) |
| Diastolic BP, mm Hg | 85 (81–102) | 83 (78–101) | 85 (82–102) | 85 (83–102) | 94 (85–102) | 94 (86–103) |
| Heart rate, bpm | 67 (60–76) | 65 (60–76) | 69 (64–77) | 65 (60–73) ** | 72 (70–78) | 78 (70–90) *§§µµ |
| LDL-cholesterol, mmol/L | – | 3.1 (2.8–3.5) | – | 2.9 (2.4–3.3) | – | 3.1 (2.3–3.3) |
| Interval therapy (between the baseline and follow-up studies) | ||||||
| ACEI/ARB | – | 79% | – | 61% | – | 81% |
| β-Blockers | – | 64% | – | 53% | – | 63% |
| Calcium channel blockers | – | 21% | – | 24% | – | 25% |
| Loop diuretics | – | 0% | – | 47% §§ | – | 69% §§ |
| Thiazide diuretics | – | 32% | – | 21% | – | 38% |
| MRA | – | 7% | – | 9% | – | 13% |
| Statins | – | 57% | – | 34% § | – | 13% §§ |
| Number of antihypertensive drugs, n | – | 2.0 (1.5–3.0) | – | 2.0 (1.0–3.0) | – | 2.5 (2.0–3.5) |
| Variables | Asymptomatic (n = 28) | Transition to HFpEF (n = 161) | Transition to Internal HFrEF (n = 16) | |||
|---|---|---|---|---|---|---|
| Baseline | Δ from Baseline (95% CI) | Baseline | Δ from Baseline (95% CI) | Baseline | Δ from Baseline (95% CI) | |
| LV mass index, g/m2 | 118 (112–142) | −13 (−26, −1) * | 136 (116–160) | 6 (−0.1, 12) §§ | 151 (122–158) | 6 (−6, 21) § |
| LV end-diastolic dimension, cm | 5.1 (4.9–5.3) | −0.5 (−0.7, −0.4) ** | 5.3 (4.9–5.5) | −0.6 (−0.6, −0.5) ** | 5.7 (5.4–5.8) §§µµ | −0.4 (−0.7, −0.1) ** |
| Relative wall thickness | 0.48 (0.43–0.51) | 0.07 (0.05, 0.09) ** | 0.46 (0.44–0.49) | 0.10 (0.09–0.11) **§ | 0.44 (0.43–0.45) §µµ | 0.07 (0.02–0.11) ** |
| LV ejection fraction, % | 61 (56–65) | 2 (−1, 5) | 60 (58–64) | 2 (−1, 4) | 58 (54–60) §µµ | −13 (−16, −10) **§§µµ |
| LA anteroposterior diameter, cm | 4.0 (3.8–4.0) | 0.3 (0.2, 0.35) ** | 4.1 (3.9–4.3) §§ | 0.45 (0.35, 0.5) **§ | 4.5 (4.4–4.7) §§µµ | 0.6 (0.3–0.9) **§ |
| Progression of LVDD a | 0 | 85 (62) §§ | 4 (67) §§ | |||
| PASP, mm Hg | 25 (23–30) | 0 (−3, 4) | 25 (23–29) | 8 (6, 10) **§§ | 24 (23–38) | 13 (7, 20) **§§ |
| Pulmonary hypertension b | 4% | 7% | 12% | 42% **§§ | 25%§ | 69% **§§µ |
| Mitral E/e′ ratio c | 8.2 (7.5–9.1) | 11.9 (10.3–14.3) §§ | 11.9 (11.2–13.4) §§µµ | |||
| LA volume index, mL/m2, c | 32 (28–37) | 41 (37–50) §§ | 54 (40–63) §§µµ | |||
| Variables | Coefficient | Standard Error | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| Interval statin treatment | −1.165 | 0.456 | 0.31 | 0.128 to 0.762 | 0.011 |
| Duration of hypertension | 0.048 | 0.023 | 1.05 | 1.001 to 1.099 | 0.044 |
| Age | 0.045 | 0.022 | 1.047 | 1.003 to 1.094 | 0.039 |
| Interval change in LV mass index | 0.017 | 0.006 | 1.017 | 1.005 to 1.029 | 0.006 |
| Variables | Coefficient | Standard Error | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| Interval chronic atrial fibrillation | 1.856 | 0.885 | 6.40 | 1.33 to 17.6 | 0.017 |
| Baseline LV end-diastolic dimension | 1.575 | 0.660 | 4.84 | 1.13 to 36.3 | 0.036 |
| Baseline LV ejection fraction | −0.175 | 0.0818 | 0.84 | 0.72 to 0.99 | 0.032 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ovchinnikov, A.; Belyavskiy, E.; Potekhina, A.; Ageev, F. Asymptomatic Left Ventricular Hypertrophy Is a Potent Risk Factor for the Development of HFpEF but Not HFrEF: Results of a Retrospective Cohort Study. J. Clin. Med. 2022, 11, 3885. https://doi.org/10.3390/jcm11133885
Ovchinnikov A, Belyavskiy E, Potekhina A, Ageev F. Asymptomatic Left Ventricular Hypertrophy Is a Potent Risk Factor for the Development of HFpEF but Not HFrEF: Results of a Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(13):3885. https://doi.org/10.3390/jcm11133885
Chicago/Turabian StyleOvchinnikov, Artem, Evgeny Belyavskiy, Alexandra Potekhina, and Fail Ageev. 2022. "Asymptomatic Left Ventricular Hypertrophy Is a Potent Risk Factor for the Development of HFpEF but Not HFrEF: Results of a Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 13: 3885. https://doi.org/10.3390/jcm11133885