
Current Effective Therapeutics in Management of COVID-19


Abstract
:1. Introduction
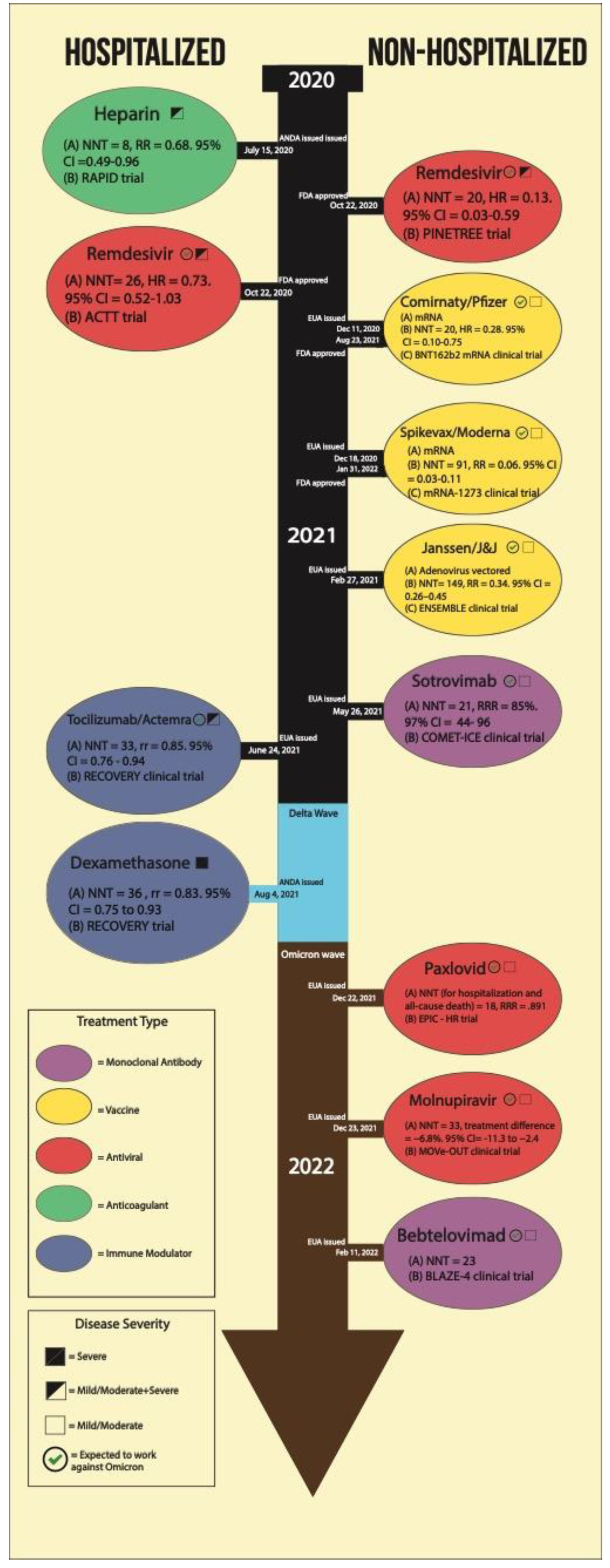
- Outpatient management: monoclonal antibodies, nirmatrelvir [PF-07321332] and ritonavir (Paxlovid), molnupiravir, remdesivir (Veklury) and bebtelovimab.
- Inpatient management: remdesivir, corticosteroids, tocilizumab, baricitinib and anakinra.
2. Outpatient Management
2.1. Monoclonal Antibodies
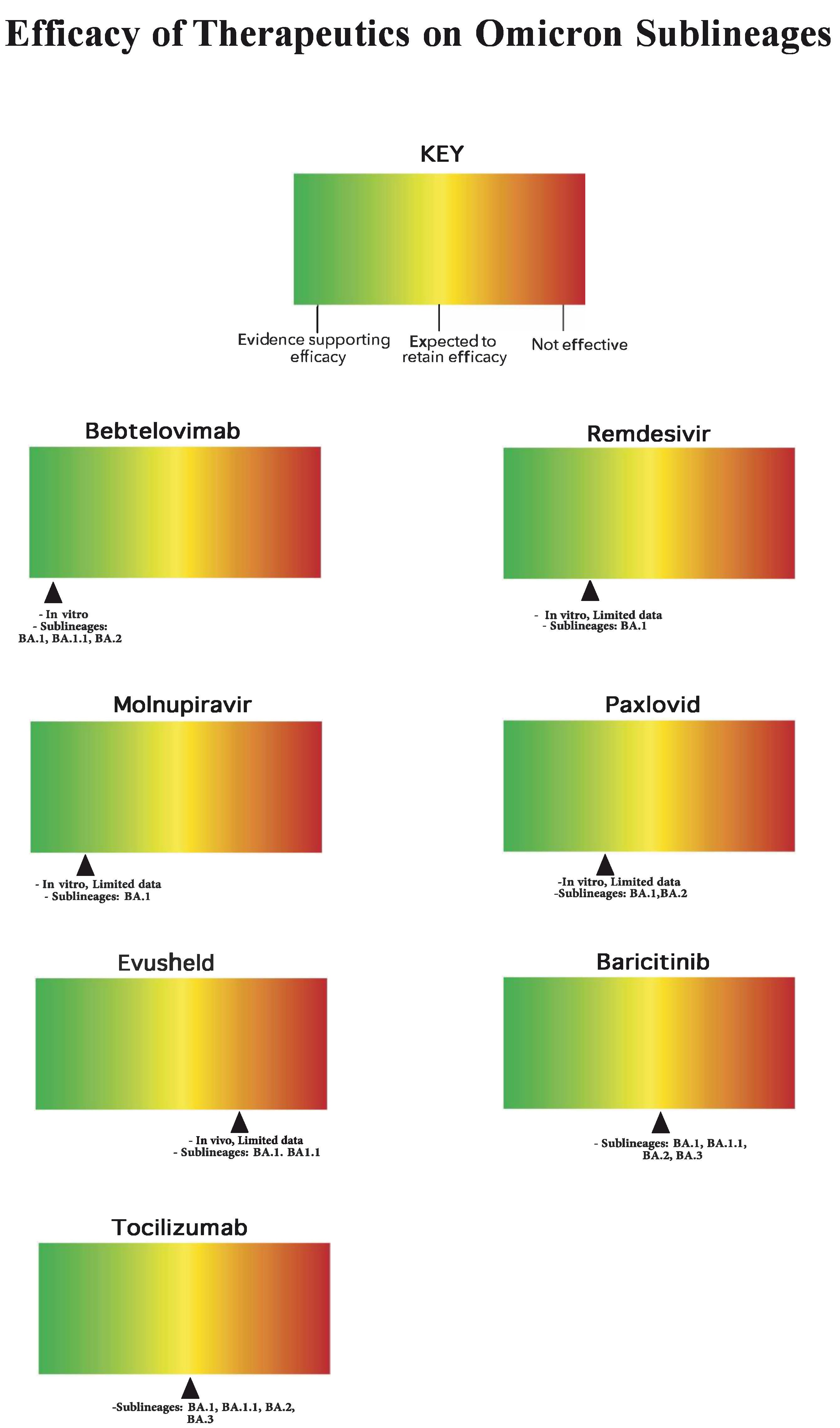
2.2. Bebtelovimab
2.3. Remdesivir
2.4. Molnupiravir
2.5. Nirmatrelvir+Ritonavir (Paxlovid)
2.6. Evusheld
3. Inpatient Management
3.1. Remdesivir
3.2. Corticosteroids
3.3. Heterogeneity of Response across the Clinical Severity Spectrum
3.4. Impact on Long-Term Autoreactivity
3.5. Predictors of Early Response
3.6. Reactivation of Latent Infections
3.7. Baricitinib
3.8. Tocilizumab
3.9. Anakinra
3.10. Anticoagulation
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. COVID Data Tracker. Centers for Disease Control and Prevention. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 15 June 2022).
- World Health Organization. WHO COVID-19 Dashboard. World Health Organization. Published 2022. Available online: https://covid19.who.int/ (accessed on 16 June 2022).
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Mahamat-Saleh, Y.; Fiolet, T.; Rebeaud, M.E.; Mulot, M.; Guihur, A.; El Fatouhi, D.; Laouali, N.; Peiffer-Smadja, N.; Aune, D.; Severi, G. Diabetes, hypertension, body mass index, smoking and COVID-19-related mortality: A systematic review and meta-analysis of observational studies. BMJ Open 2021, 11, e052777. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32020029 (accessed on 18 May 2022). [CrossRef]
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discov. 2020, 6, 16. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32194981 (accessed on 18 May 2022). [CrossRef] [Green Version]
- Fiolet, T.; Guihur, A.; Rebeaud, M.E.; Mulot, M.; Peiffer-Smadja, N.; Mahamat-Saleh, Y. Effect of hydroxychloroquine with or without azithromycin on the mortality of coronavirus disease 2019 (COVID-19) patients: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 19–27. [Google Scholar] [CrossRef]
- Molento, M.B. Ivermectin against COVID-19: The unprecedented consequences in Latin America. One Health. 2021, 13, 100250. [Google Scholar] [CrossRef]
- CDC. Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention. Published 11 February 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html#:~:text=Conclusions- (accessed on 16 June 2022).
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-Harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 10242. [Google Scholar] [CrossRef]
- Nonhospitalized Adults: Therapeutic Management. COVID-19 Treatment Guidelines. Published 8 April 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management/nonhospitalized-adults--therapeutic-management/#:~:text=Bebtelovimab%20is%20a%20recombinant%20neutralizing (accessed on 7 May 2022).
- Anti-SARS-CoV-2 Monoclonal Antibodies. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/anti-sars-cov-2-antibody-products/anti-sars-cov-2-monoclonal-antibodies/ (accessed on 16 June 2022).
- FDA. Emergency Use Authorization (EUA) for Sotrovimab. Published 5 April 2022. Available online: https://www.fda.gov/media/157556/download (accessed on 17 May 2022).
- ATTACC, ACTIV-4a, REMAP-CAP investigators. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef]
- Mazzaferri, F.; Mirandola, M.; Savoldi, A.; de Nardo, P.; Morra, M.; Tebon, M.; Armellini, M.; de Luca, G.; Calandrino, L.; Sasset, L.; et al. Exploratory data on the clinical efficacy of monoclonal antibodies against SARS-COV-2 omicron variant of concern. medRxiv 2022. Available online: https://www.medrxiv.org/content/10.1101/2022.05.06.22274613v1 (accessed on 9 May 2022).
- Mader, A.L.; Tydykov, L.; Glück, V.; Bertok, M.; Weidlich, T.; Gottwald, C.; Stefl, A.; Vogel, M.; Plentz, A.; Köstler, J.; et al. Omicron’s binding to sotrovimab, casirivimab, imdevimab, CR3022, and Sera from previously infected or vaccinated individuals. iScience 2022. Available online: https://www.sciencedirect.com/science/article/pii/S2589004222003467 (accessed on 7 May 2022).
- Center for Drug Evaluation and Research. FDA updates Sotrovimab Emergency Use Authorization. U.S. Food and Drug Administration. Published 5 April 2022. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-updates-sotrovimab-emergency-use-authorization (accessed on 7 May 2022).
- Iketani, S.; Liu, L.; Guo, Y.; Liu, L.; Chan, J.F.; Huang, Y.; Wang, M.; Luo, Y.; Yu, J.; Chu, H.; et al. Antibody evasion properties of SARS-CoV-2 Omicron sublineages. Nature 2022, 604, 553–556. Available online: https://www.ncbi.nlm.nih.gov/pubmed/35240676 (accessed on 18 May 2022). [CrossRef]
- Hastie, K.M.; Li, H.; Bedinger, D.; Schendel, S.L.; Dennison, S.M.; Li, K.; Rayaprolu, V.; Yu, X.; Mann, C.; Zandonatti, M.; et al. Defining variant-resistant epitopes targeted by SARS-CoV-2 antibodies: A global consortium study. Science 2021, 374, 472–478. [Google Scholar] [CrossRef]
- Westendorf, K.; Žentelis, S.; Wang, L.; Foster, D.; Vaillancourt, P.; Wiggin, M.; Lovett, E.; van der Lee, R.; Hendle, J.; Pustilnik, A.; et al. LY-CoV1404 (bebtelovimab) potently neutralizes SARS-CoV-2 variants. Preprint bioRxiv 2022. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Nirula, A.; Chen, P. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19: A Randomized Clinical Trial |Global Health |JAMA| JAMA Network. jamanetwork.com. Published 21 January 2021. Available online: https://jamanetwork.com/journals/jama/fullarticle/2775647 (accessed on 18 May 2022).
- Office of the Commissioner. Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant. FDA. Published 15 February 2022. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-new-monoclonal-antibody-treatment-covid-19-retains#:~:text=The%20EUA%20for%20bebtelovimab%20is (accessed on 10 May 2022).
- Remdesivir. COVID-19 Treatment Guidelines. Published 24 February 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/remdesivir/ (accessed on 5 May 2022).
- Coronavirus Disease 2019 (COVID-19) Daily Research Briefs. www.aafp.org. Published 17 March 2022. Available online: https://www.aafp.org/journals/afp/content/covid-briefs.html (accessed on 18 May 2022).
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. New England Journal of Medicine. 2021, 386, 305–315. [Google Scholar] [CrossRef]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, Molnupiravir and Nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antiviral Res. 2022, 198, 105252. [Google Scholar] [CrossRef]
- Kabinger, F.; Stiller, C.; Schmitzová, J.; Dienemann, C.; Kokic, G.; Hillen, H.S.; Höbartner, C.; Cramer, P. Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat. Struct. Mol. Biol. 2021, 28, 740–746. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N Engl. J Med. 2021, 386. [Google Scholar] [CrossRef]
- Caraco, Y.; Crofoot, G.E.; Moncada, P.A.; Galustyan, A.N.; Musungaie, D.B.; Payne, B.; Kovalchuk, E.; Gonzalez, A.; Brown, M.L.; Williams-Diaz, A.; et al. Phase 2/3 Trial of Molnupiravir for Treatment of Covid-19 in Nonhospitalized Adults. NEJM Evidence 2021, 1. [Google Scholar] [CrossRef]
- Pfizer. Pfizer Announces Additional Phase 2/3 Study Results Confirming Robust Efficacy of Novel COVID-19 Oral Antiviral Treatment Candidate in Reducing Risk of Hospitalization or Death | Pfizer. Pfizer.com. Published 2021. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-additional-phase-23-study-results. (accessed on 5 May 2022).
- Findlay, V.J. Ritonavir. In xPharm: The Comprehensive Pharmacology Reference; Enna, S.J., Bylund, D.B., Eds.; Elsevier: Amsterdam, The Netherlands, 2007; pp. 1–6. ISBN 9780080552323. [Google Scholar] [CrossRef]
- Pfizer. Pfizer’s Novel COVID-19 Oral Antiviral Treatment Candidate Reduced Risk of Hospitalization or Death by 89% in Interim Analysis of Phase 2/3 EPIC-HR Study | Pfizer. Pfizer.com. Published 2021. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate (accessed on 5 May 2022).
- Hull, M.W.; Montaner, J.S.G. Ritonavir-boosted protease inhibitors in HIV therapy. Ann. Med. 2011, 43, 375–388. [Google Scholar] [CrossRef]
- Commissioner O of the Coronavirus (COVID-19) Update: FDA Authorizes First Oral Antiviral for Treatment of COVID-19. FDA. Published December 22, 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19#:~:text=Today%2C%20the%20U.S.%20Food%20and (accessed on 5 May 2022).
- Frequently Asked Questions on the Emergency Use Authorization for Paxlovid for Treatment of COVID-19. 2021. Available online: https://www.fda.gov/media/155052/download (accessed on 18 May 2022).
- Fact Sheet for Healthcare Providers: Emergency Use Authorization for Paxlovid. FDA; 2022. Available online: https://www.fda.gov/media/155050/download (accessed on 16 May 2022).
- Pfizer Receives U.S. FDA Emergency Use Authorization for Novel COVID-19 Oral Antiviral Treatment | Pfizer. Pfizer.com. Published 2021. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-receives-us-fda-emergency-use-authorization-novel (accessed on 7 May 2022).
- Dyer, O. Covid-19: Doctors will refuse to limit use of antiviral drug to unvaccinated patients, say ethicists. BMJ 2021, 375, n2855. [Google Scholar] [CrossRef]
- 39. Research C for DE and. FDA Updates on Paxlovid for Health Care Providers. FDA. Published online 4 May 2022. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-updates-paxlovid-health-care-providers (accessed on 18 May 2022).
- Langreth, R.; Muller, M. U.S. Seeks “Urgent” Data on Covid Relapses After Using Pfizer’s Drug. Bloomberg.com. Published 29 April 2022. Available online: https://www.bloomberg.com/news/articles/2022-04-29/u-s-seeks-urgent-data-on-covid-relapses-after-pfizer-drug (accessed on 7 May 2022).
- Catlin, N.; Bowman, C.; Campion, S.; Cheung, J.; Nowland, W.; Sathish, J.; Stethem, C.; Updyke, L.; Cappon, G. Reproductive and developmental safety of nirmatrelvir (PF-07321332), an oral SARS-CoV-2 Mpro inhibitor in animal models. Reprod. Toxicol. 2022, 108, 56–61. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, L. In the age of Omicron variant: Paxlovid raises new hopes of COVID-19 recovery. J. Med Virol. 2021, 94, 1766–1767. [Google Scholar] [CrossRef]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Halfmann, P.; Watanabe, S.; Maeda, K.; et al. Efficacy of antiviral agents against the SARS-CoV-2 Omicron subvariant BA.2. N Engl J Med. 2022, 386, 1475–1477. Available online: https://www.ncbi.nlm.nih.gov/pubmed/35263535 (accessed on 18 May 2022). [CrossRef]
- Evusheld Antibody Treatment for COVID-19 High-risk Groups | SCDHEC. scdhec.gov. Available online: https://scdhec.gov/covid19/monoclonal-antibodies/evusheld-antibody-treatment-covid-19-high-risk-groups (accessed on 18 May 2022).
- About EVUSHELD. Published March 2022. Available online: https://www.evusheld.com/en/hcp (accessed on 10 May 2022).
- Fact Sheet for Healthcare Providers: Emergency use Authorization for Evusheldtm (Tixagevimab Co-packaged with Cilgavimab) Highlights of Emergency Use Authorization (eua) These Highlights of the Eua do not Include all the Information Needed to Use Evusheldtm under the Eua. See the Full Fact Sheet for Healthcare Providers for Evusheld. The U.S. Food and Drug Administration. 2022. Available online: https://den8dhaj6zs0e.cloudfront.net/50fd68b9-106b-4550-b5d0-12b045f8b184/6d1d5fea-2532-46e9-a1d4-1504f6dd41b2/6d1d5fea-2532-46e9-a1d4-1504f6dd41b2_viewable_rendition__v.pdf (accessed on 10 May 2022).
- Research C for DE and. FDA authorizes revisions to Evusheld dosing. FDA. Published online 24 February 2022. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-authorizes-revisions-evusheld-dosing (accessed on 18 May 2022).
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Seegobin, S.; Templeton, A.; Yuan, Y.; Ambery, P.; Arends, R.H.; et al. LB5. PROVENT: Phase 3 Study of Efficacy and Safety of AZD7442 (Tixagevimab/Cilgavimab) for Pre-exposure Prophylaxis of COVID-19 in Adults. Open Forum Infect. Dis. 2021, 8, S810. [Google Scholar] [CrossRef]
- Office of the Commissioner. Coronavirus (COVID-19) Update: FDA Authorizes New Long-Acting Monoclonal Antibodies for Pre-exposure Prevention of COVID-19 in Certain Individuals. FDA. Published 8 December 2021. 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-new-long-acting-monoclonal-antibodies-pre-exposure (accessed on 18 May 2022).
- Case, J.B.; Mackin, S.; Errico, J.; Chong, Z.; Madden, E.A.; Guarino, B.; Schmid, M.A.; Rosenthal, K.; Ren, K.; Jung, A.; et al. Resilience of S309 and Azd7442 Monoclonal Antibody Treatments Against Infection by SARS-COV-2 Omicron Lineage Strains. BioRxiv. Published 1 January 2022. Available online: https://www.biorxiv.org/content/10.1101/2022.03.17.484787v1 (accessed on 13 May 2022).
- Prevention of SARS-CoV-2. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/prevention-of-sars-cov-2/ (accessed on 18 May 2022).
- Jorgensen, S.C.; Kebriaei, R.; Dresser, L.D. Remdesivir: Review of Pharmacology, Pre-clinical Data, and Emerging Clinical Experience for COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 659–671. [Google Scholar] [CrossRef]
- Ali, K.; Azher, T.; Baqi, M.; Binnie, A.; Borgia, S.; Carrier, F.M.; Cavayas, Y.A.; Chagnon, N.; Cheng, M.P.; Conly, J.; et al. Remdesivir for the treatment of patients in hospital with COVID-19 in Canada: A randomized controlled trial. Can. Med Assoc. J. 2022, 194, E242–E251. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Remdesivir and three other drugs for hospitalised patients with COVID-19: Final results of the WHO Solidarity randomised trial and updated meta-analyses. Lancet 2022, 399, 1941–1953. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed antiviral drugs for COVID-19—interim WHO Solidarity trial results. N Engl J Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Hospitalized Adults: Therapeutic Management. COVID-19 Treatment Guidelines. Published 24 February 2022. 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/. (accessed on 5 May 2022).
- Benfield, T.; Bodilsen, J.; Brieghel, C.; Harboe, Z.B.; Helleberg, M.; Holm, C.; Israelsen, S.B.; Jensen, J.; Jensen, T.; Johansen, I.S.; et al. Improved Survival Among Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) Treated With Remdesivir and Dexamethasone. A Nationwide Population-Based Cohort Study. Clin. Infect. Dis. 2021, 73, 2031–2036. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19—preliminary report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- Keller, M.J.; A Kitsis, E.; Arora, S.; Chen, J.-T.; Agarwal, S.; Ross, M.J.; Tomer, Y.; Southern, W. Effect of Systemic Glucocorticoids on Mortality or Mechanical Ventilation in Patients With COVID-19. J. Hosp. Med. 2020, 15, 489–493. [Google Scholar] [CrossRef]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Woodruff, M.C.; Ramonell, R.P.; Lee, F.E.; Sanz, I. Broadly-targeted autoreactivity is common in severe SARS-CoV-2 Infection. medRxiv [Preprint] 2020. [Google Scholar]
- Ramaswamy, A.; Brodsky, N.N.; Sumida, T.S.; Comi, M.; Asashima, H.; Hoehn, K.B.; Li, N.; Liu, Y.; Shah, A.; Ravindra, N.G.; et al. Post-infectious inflammatory disease in MIS-C features elevated cytotoxicity signatures and autoreactivity that correlates with severity. medRxiv [Preprint]. 2020. [Google Scholar]
- Wang, E.Y.; Mao, T.; Klein, J.; Dai, Y.; Huck, J.D.; Jaycox, J.R.; Liu, F.; Zhou, T.; Israelow, B.; Wong, P.; et al. Diverse functional autoantibodies in patients with COVID-19. Nature 2021, 595, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Merritt, Z.; Assa, A.; Mustehsan, H.; Chung, E.; Liu, S.; Kumtheka, A.; Ayesha, B.; McCort, M.; Palaiodimos, L.; et al. Early and Significant Reduction in C-Reactive Protein Levels After Corticosteroid Therapy Is Associated With Reduced Mortality in Patients With COVID-19. J. Hosp. Med. 2021, 16, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Auto-antibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Boggild, A.; Libman, M.; Greenaway, C.; McCarthy, A. CATMAT statement on disseminated strongyloidiasis: Prevention, assessment and management guidelines. Can. Commun. Dis. Rep. 2016, 42, 12–19. [Google Scholar] [CrossRef]
- Krolewiecki, A.; Nutman, T.B. Strongyloidiasis: A neglected tropical disease. Infect Dis Clin North Am. 2019, 33, 135–151. [Google Scholar] [CrossRef]
- Stauffer, W.M.; Alpern, J.D.; Walker, P.F. COVID-19 and Dexamethasone: A Potential Strategy to Avoid Steroid-Related Strongyloides Hyperinfection. JAMA 2020. [Google Scholar] [CrossRef]
- Cliffe, A.R.; Arbuckle, J.H.; Vogel, J.L.; Geden, M.J.; Rothbart, S.B.; Cusack, C.L.; Strahl, B.D.; Kristie, T.M.; Deshmukh, M. Neuronal Stress Pathway Mediating a Histone Methyl/Phospho Switch Is Required for Herpes Simplex Virus Reactivation. Cell Host Microbe 2015, 18, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Du, T.; Zhou, G.; Roizman, B. HSV-1 gene expression from reactivated ganglia is disordered and concurrent with suppression of latency-associated transcript and miRNAs. Proc. Natl. Acad. Sci. U.S.A 2011, 108, 18820–18824. [Google Scholar] [CrossRef] [Green Version]
- Sheffy, B.E.; Davies, D.H. Reactivation of a bovine herpesvirus after corticosteroid treatment. Proc Soc Exp Biol Med. 1972, 140, 974–976. [Google Scholar] [CrossRef] [PubMed]
- Bousoik, E.; Montazeri Aliabadi, H. "Do We Know Jack" About JAK? A Closer Look at JAK/STAT Signaling Pathway. Front Oncol. 2018, 8, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R.; et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Zhang, S.; Li, L.; Shen, A.; Chen, Y.; Qi, Z. Rational use of tocilizumab in the treatment of novel coronavirus pneumonia. Clin Drug Investig. 2020, 40, 511–518. [Google Scholar] [CrossRef] [Green Version]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- European Medicines Agency. Kineret - European Medicines Agency. European Medicines Agency. Published 17 September 2018. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/kineret (accessed on 5 May 2022).
- Kyriazopoulou, E.; Poulakou, G.; Milionis, H.; Metallidis, S.; Adamis, G.; Tsiakos, K.; Fragkou, A.; Rapti, A.; Damoulari, C.; Fantoni, M.; et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: A double-blind, randomized controlled phase 3 trial. Nature Medicine 2021, 27. [Google Scholar] [CrossRef]
- The REMAP-CAP Investigators. Effectiveness of Tocilizumab, Sarilumab, and Anakinra for critically ill patients with COVID-19 The REMAP-CAP COVID-19 Immune Modulation Therapy Domain Randomized Clinical Trial, Cold Spring Harbor Laboratory. 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.06.18.21259133v2 (accessed on 18 May 2022).
- CORIMUNO-19 Collaborative Group. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomised controlled trial. Lancet Respir Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- European Medicines Agency. Kineret (Anakinra) an Overview of Kineret and Why It Is Authorised in the EU. 2021. Available online: https://www.ema.europa.eu/en/documents/overview/kineret-epar-medicine-overview_en.pdf (accessed on 16 June 2022).
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of February 23, 2022. Pol Arch Intern Med. 2022, 132, 16230. [Google Scholar] [CrossRef]
- Liu, J.; Li, J.; Arnold, K.; Pawlinski, R.; Key, N.S. Using heparin molecules to manage COVID-2019. Res Pract Thromb Haemost. 2020, 4, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sholzberg, M.; da Costa, B.R.; Tang, G.H.; Rahhal, H.; AlHamzah, M.; Baumann Kreuziger, L.; Ní Áinle, F.; Almarshoodi, M.O.; James, P.D.; Lillicrap, D.; et al. Randomized trials of therapeutic heparin for COVID-19: A meta-analysis. Res Pract Thromb Haemost. 2021, 5, e12638. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1. Aged ≥ 65 years |
| 2. Obesity (BMI > 30) |
| 3. Diabetes mellitus type 2 |
| 4. History of CAD, hypertension, congenital heart disease |
| 5. History of respiratory disease, such as COPD, moderate or severe persistent asthma, interstitial lung disease, cystic fibrosis, pulmonary hypertension |
| 6. Sickle cell disease |
| 7. Immunosuppressive regimen |
| 8. History of: cancer, chronic liver disease, chronic lung diseases, dementia or other neurological conditions, diabetes, Down syndrome, HIV infection, Immunocompromised, mental health conditions: depression, schizophrenia, sickle cell disease, tuberculosis, substance use disorders, stroke or cerebrovascular disease, organ or blood stem cell transplant |
| 9. Chronic kidney disease |
| 10. Are overweight, obese, pregnant, smoke [14]. |
| Corticosteroids are beneficial |
| 1. Moderate to severe ARDS (defined using Berlin Criteria) and need for invasive mechanical ventilation |
| 2. Moderate to severe ARDS requiring non-invasive mechanical ventilation (high flow nasal cannula) |
| 3. Mild ARDS (pao2/fio2 < 300) and requiring oxygen support |
| 4. Pneumonia severity index (PSI) > 130 |
| Corticosteroids may be beneficial |
| 1. ARDS and elevated inflammatory markers (CRP > 20 mg/dL) |
| Corticosteroids may be harmful |
| 1. Mild to moderate disease not requiring oxygen support |
| 2. Mild to moderate disease and low inflammatory markers (CRP < 20 mg/dL) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atluri, K.; Aimlin, I.; Arora, S. Current Effective Therapeutics in Management of COVID-19. J. Clin. Med. 2022, 11, 3838. https://doi.org/10.3390/jcm11133838
Atluri K, Aimlin I, Arora S. Current Effective Therapeutics in Management of COVID-19. Journal of Clinical Medicine. 2022; 11(13):3838. https://doi.org/10.3390/jcm11133838
Chicago/Turabian StyleAtluri, Kavya, Iris Aimlin, and Shitij Arora. 2022. "Current Effective Therapeutics in Management of COVID-19" Journal of Clinical Medicine 11, no. 13: 3838. https://doi.org/10.3390/jcm11133838